
Abstract
Objective:
To report nationally representative findings on the prevalence, correlates, psychiatric comorbidity and treatment of DSM-IV Cannabis Use and Cannabis Use Disorders in Australia.
Method:
The 2007 National Survey of Mental Health and Wellbeing was a nationally representative household survey of 8841 Australians (16–85 years) that assessed symptoms of the most prevalent DSM-IV mental disorders.
Results:
Prevalence of lifetime and 12-month cannabis use was 18% and 6%; prevalence of lifetime and 12-month cannabis use disorder was 6% and 1%. The conditional prevalence (proportion of ever users who met criteria for a disorder) of lifetime and 12-month cannabis use disorder was 32.2% and 14.3%. Current cannabis use disorders were more common in males (OR 2.0) and younger users (OR 4.6). Strong associations were observed between current cannabis use disorders and alcohol use disorders (OR 3.6) and current affective disorders (OR 3.0). Only 36.2% of those with current cannabis use disorders sought any treatment.
Conclusions:
The prevalence of cannabis use disorders in the Australian population is comparable with that in the USA. Current cannabis use disorders are highly concentrated in young Australians who have high levels of comorbidity. The low rates of treatment seeking warrant attention in treatment and prevention strategies.
Introduction
Cannabis is the most commonly used illicit drug by young people in high-income countries (Hall and Degenhardt, 2009; United Nations Office on Drugs and Crime, 2009) and cannabis users in the general population frequently endorse symptoms of cannabis use disorders (Swift et al., 2001). Despite earlier suggestions that cannabis use was relatively benign, problems associated with use of the drug are now well recognised (Copeland and Swift, 2009; De Graaf et al., 2010; Hall and Degenhardt, 2009; Hall and Pacula, 2003). While uncertainties exist about the number of people who use cannabis worldwide, it is estimated that 166 million adults did so in 2006 (3.9% of the global population aged 15–64 years) (Hall and Degenhardt, 2009). Use was highest in the USA, Australia, and New Zealand, followed by Europe (Hall and Degenhardt, 2009). In Australia, it is estimated that cannabis use causes around 16% of all illicit drug related hospital costs—second only to opioids (Collins et al., 2008).
The prevalence of cannabis use disorders has been the focus of large-scale epidemiological surveys across the world. In the more recent surveys using DSM-IV criteria the prevalence of cannabis use disorders in the past year has ranged from 1.4% in New Zealand to 2.2% in the Australian population(Compton et al., 2007; Swift et al., 2001; Wells et al., 2006). The most recent estimate of the prevalence of cannabis use disorders in the lifetime is 8.5% in the US population (Compton et al., 2007; Swift et al., 2001).
The first, and most recent, study of cannabis use disorders in Australia occurred in the 1997 National Survey of Mental Health and Wellbeing (NSMHWB) which provided only 12-month estimates of disorders. It found that approximately 1 in 12 Australians (7.1%) had used cannabis more than 5 times in the past 12 months. Within the adult population, 2.2% met criteria for a DSM-IV cannabis use disorder and the conditional prevalence (proportion of ever users who met criteria for a disorder) was 31.7% (Swift et al., 2001). A cross-national comparison with the US National Comorbidity Survey found that although rates of use of cannabis were similar in the two countries, rates of cannabis dependence and the probability of dependence among users were higher in Australia than in the USA (McBride et al., 2009; Teesson et al., 2006).
It is crucial that epidemiological information be as up-to-date and accurate as possible to reflect dynamic changes in patterns of drug use (Hasin et al., 2007). Surveys of the US population have indicated that while rates of cannabis use remained stable between 1992 and 2002, the rates of DSM-IV cannabis use disorders increased significantly across this period (Compton et al., 2004). These surveys of the US population were based on the same diagnostic instrument, with only minor language edits as, detailed in Compton et al., (2004). Ongoing population-based surveys are needed to capture these shifts in the prevalence of cannabis use disorders. Cross-national research conducted as part of the World Health Organization (WHO) World Mental Health Surveys has also shown that cannabis use was highest in the USA and New Zealand (both 42%) and that, internationally, drug use was most common among males, with the gender gap closing in younger cohorts (Degenhardt et al., 2008). However, current cross-national comparisons lack an up-to-date Australian perspective.
This article uses data from the 2007 NSMHWB to provide the first estimates of the lifetime rates of cannabis use disorders in Australia and the age at which they are most likely to develop. Such timely findings on the prevalence, patterns, severity and treatment rates for cannabis use disorders are essential to guide an informed policy and treatment response.
This article aims to
provide lifetime and 12-month estimates of the prevalence of cannabis use and cannabis use disorders in the Australian population;
compare the demographic characteristics of groups defined by cannabis involvement (non-users, users without a cannabis use disorder, users with a cannabis use disorder);
investigate the associations between cannabis use disorders and other mental disorders;
examine the relationship between cannabis use disorders and health service utilization.
Methods
Sample
The 2007 NSMHWB was commissioned by the Australian Government Department of Health and Ageing, and conducted by the Australian Bureau of Statistics from August to December 2007. Respondents were selected at random from a stratified, multistage area probability sample of private dwellings. The population was persons aged 16–85 years who were usual residents of private dwellings. Household information was provided by any householder aged over 17 years and an algorithm randomly selected a householder to interview. The youngest (16–24 years) and oldest (65–85 years) age groups had a higher probability of being selected to ensure sufficient samples sizes (Slade et al., 2009). Sampling procedures generated an initial sample of 17,352 dwellings. Following loss of ineligible dwellings, owing to all household members being out of scope or vacant dwellings, the sample size was 14,805. Of these, 8841 respondents completed the interview, a 60% response rate. The sample of 8841 represents an estimated population count of 16,015,000 adults. Table 1 shows the total sample counts and estimated population counts across demographic characteristics.
Demographic characteristics of survey respondents in the 2007 National Survey of Mental Health and Wellbeing.
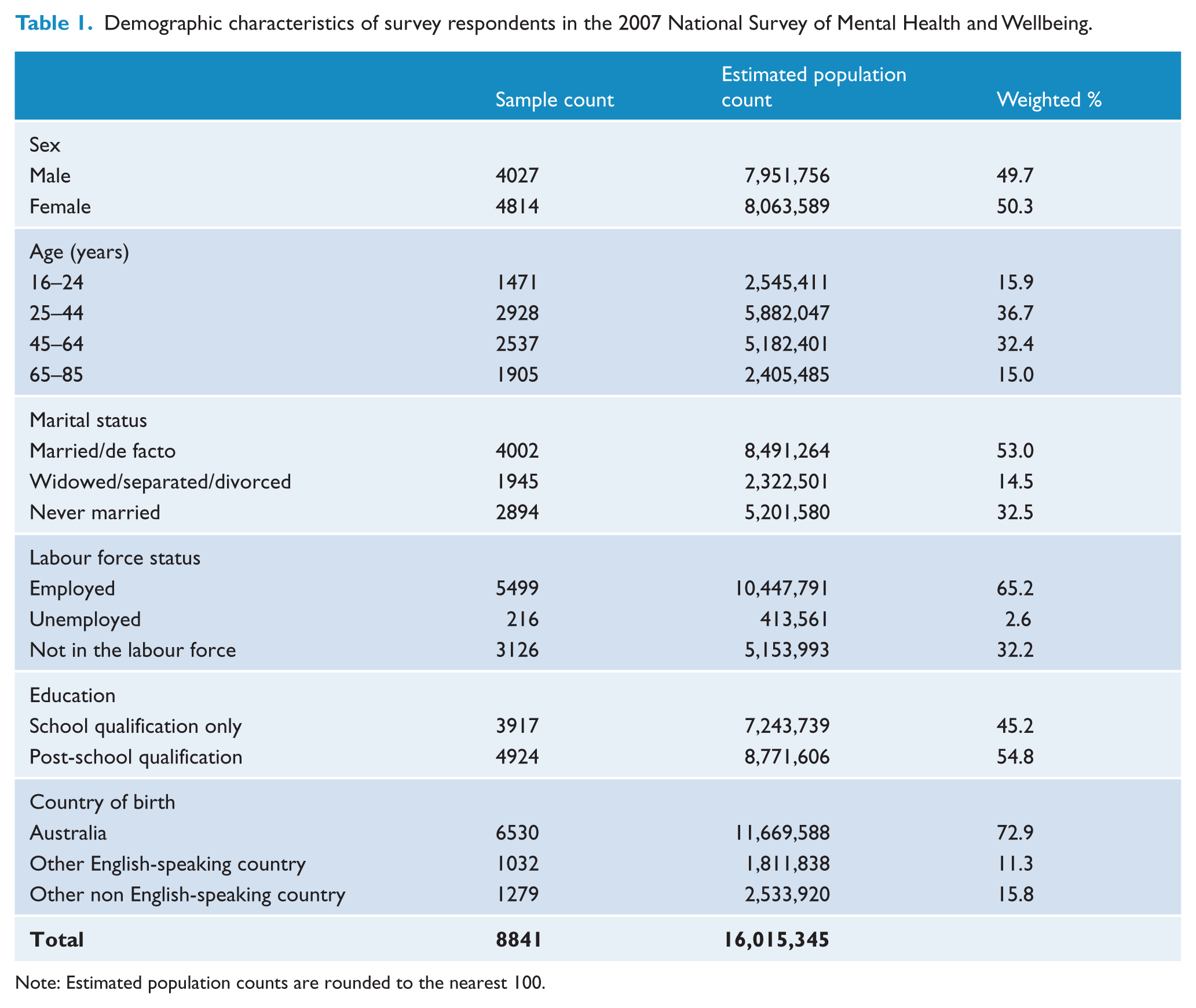
Note: Estimated population counts are rounded to the nearest 100.
Measures
A modified version of the World Mental Health Composite International Diagnostic Interview [WMH-CIDI (Kessler and Ustun, 2004)] was used. A full description of the measures can be found in Slade et al. (2009). The WMH-CIDI (Kessler and Ustun, 2004) has undergone extensive methodological development and testing, and has been used in household surveys in at least 28 countries around the world. This instrument collects diagnostic information on a broad range of mental disorders and on risk factors, impacts, patterns and treatment. The interviews were conducted face-to-face by a trained layperson who recorded responses directly on a laptop computer.
In assessing the presence of DSM-IV cannabis use disorders, participants were asked initially whether they used cannabis at least five times in any one year in their lifetime. Individuals who responded ‘no’ to this question were not asked any additional questions in the cannabis section. Only those who answered this question positively were administered the symptom questions that operationalise the DSM-IV cannabis use disorder diagnostic criteria (N = 1639; 18% of the whole sample). The 2007 NSMHWB interview was expanded to allow collection of drug-specific diagnostic information with regard to four separate classes of drugs (cannabis, sedatives, stimulants and opioids). Sequencing problems in earlier versions of the WMH-CIDI substance use section were also resolved (Degenhardt et al., 2007a, 2007b; Grant et al. 2007)to enable the diagnosis of cannabis dependence to be made in the absence of cannabis abuse. A series of 18 questions operationalised the cannabis use disorders (abuse and dependence criteria). All respondents were asked all required questions. Service use was defined as at least one consultation with any health professional for mental health reasons in the past 12 months.
Analysis
Weighted means, frequencies and cross-tabulations were computed. Adjusted odds ratios (ORs) derived from multiple logistic regression analyses indicated associations between cannabis use disorders and sociodemographic variables, while controlling for all other sociodemographic variables of interest. Associations of cannabis use disorders with psychiatric comorbidity were calculated for single disorders, disorder classes (affective, anxiety, alcohol use disorders) and for the number of comorbid disorders. Standard errors (SEs) of these estimates were obtained through the delete-a-group jack knife variance technique. SEs and confidence intervals were estimated using Software for Survey Data Analysis (SUDAAN) (Research Triangle Institute, 2007). Hazard rates, reflecting lifetime cannabis use and cannabis use disorder risk at specific ages among the population at risk at those ages, were calculated using life table methods. Hazard rate curves were smoothed statistically using rolling averages of five-year age groups.
Results
Prevalence and correlates of cannabis use and DSM-IV cannabis use disorders
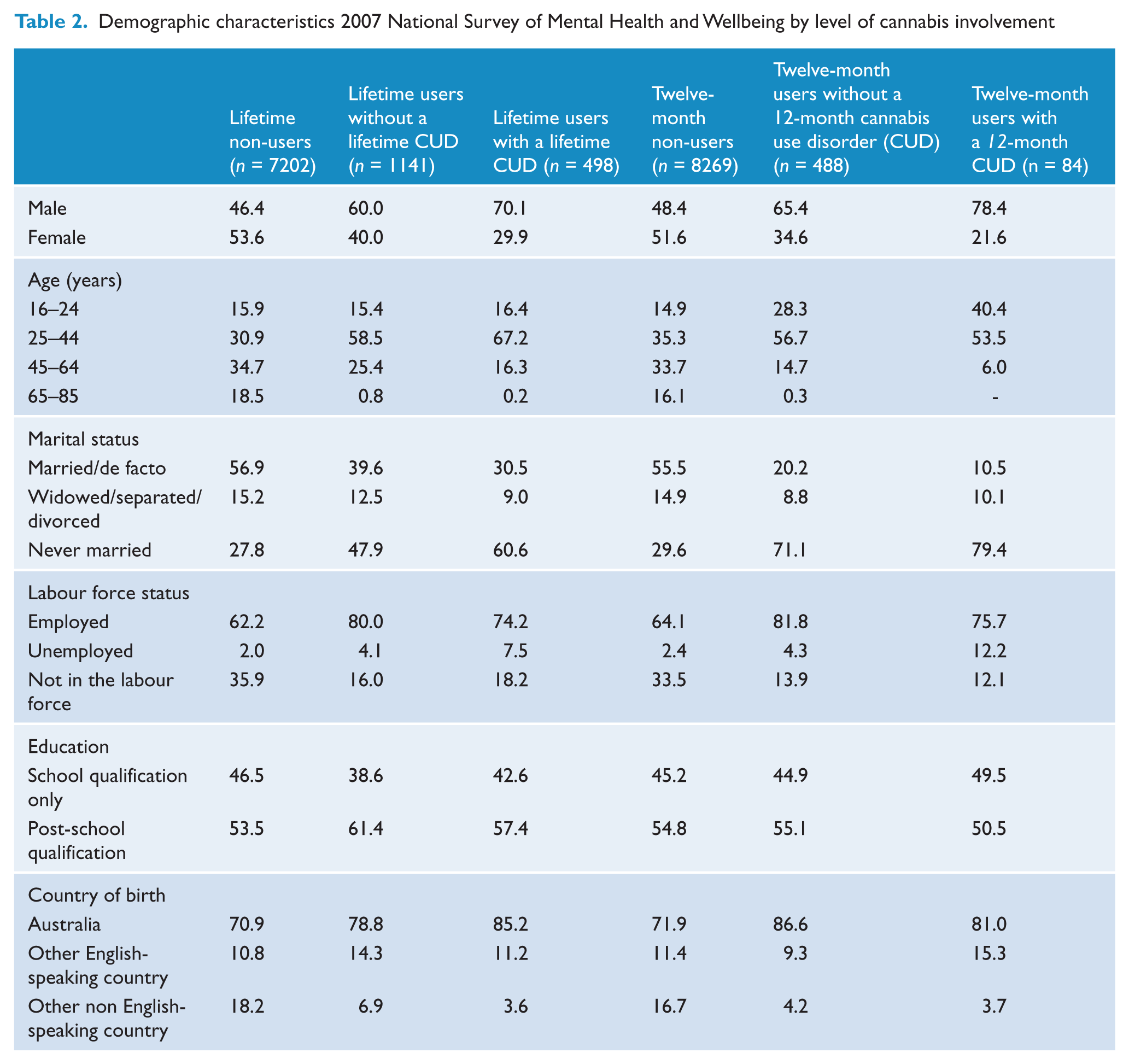
The prevalence of lifetime and 12-month use of cannabis at least 5 times was 18% and 6%. The demographic characteristics of users and non-users are presented in Table 2. The prevalence of lifetime and 12-month cannabis use disorders was 6.2% and 1.0% (Table 3). The conditional prevalence of lifetime and 12-month cannabis use disorders was 32.2% and 14.3%. Table 2 shows the characteristics of survey respondents by level of cannabis involvement for lifetime and 12-month cannabis use disorders. Lifetime cannabis use (without disorder) was highest in males, those aged 25–44 years and those who had never married, were Australian –born, employed and with higher educational qualifications. The pattern for 12-month cannabis users and those with lifetime and 12-month disorders was similar.
Demographic characteristics 2007 National Survey of Mental Health and Wellbeing by level of cannabis involvement
Prevalence of lifetime and 12-month DSM-IV Cannabis Use Disorder (CUD) in the total sample and among cannabis users by sociodemographic characteristics in the 2007 National Survey of Mental Health and Wellbeing.
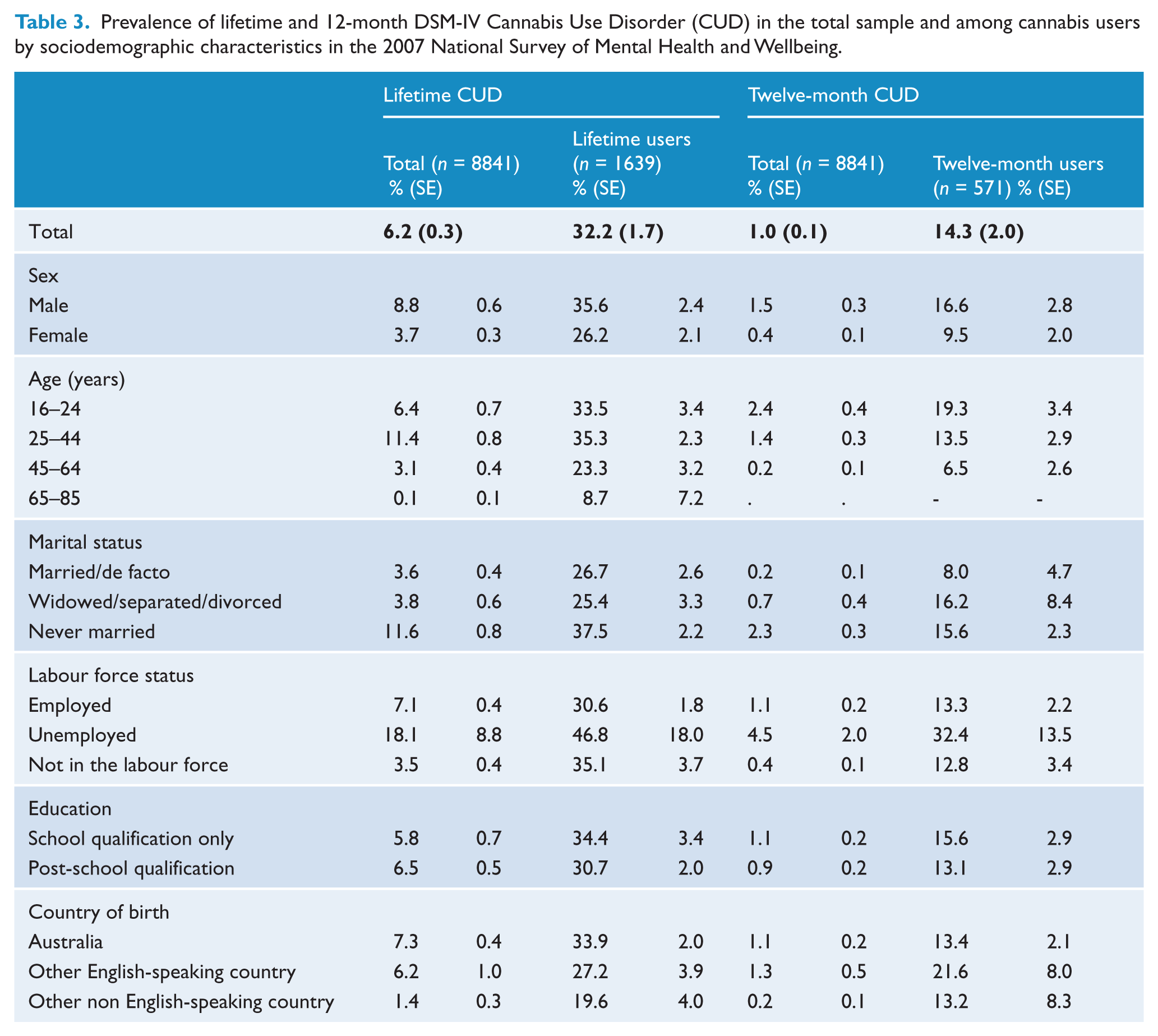
Table 3 shows the prevalence of lifetime and 12-month cannabis use disorders in population subgroups. The prevalence of lifetime cannabis use disorders was highest in males (8.8%), those aged 25–44 years (11.4%), those who had never married (11.6%) and the unemployed (18.1%). Lifetime conditional prevalence was similar across age groups. The prevalence of 12-month cannabis use disorders was highest in males (1.5%), those aged 16–24 years (2.4%), those who had never married (2.3%) and the unemployed (4.5%).
The strength of association between demographic variables and lifetime cannabis use disorders by level of cannabis involvement is presented in Table 4(a). In order to compare cannabis users without a cannabis use disorder with both the non-users and users with a cannabis use disorder, cannabis users without a cannabis use disorder were chosen as the reference category. The odds of lifetime non-use compared with lifetime use (without a cannabis use disorder) was lower among males, younger respondents and those who had been married. The odds of lifetime cannabis use disorder compared with lifetime use alone were greater among males, those aged 25–44 years, those who had never married and those who were Australian born.
Adjusted odds ratios (OR) of lifetime DSM-IV any cannabis use disorder (CUD) by sociodemographic characteristics and level of cannabis involvement
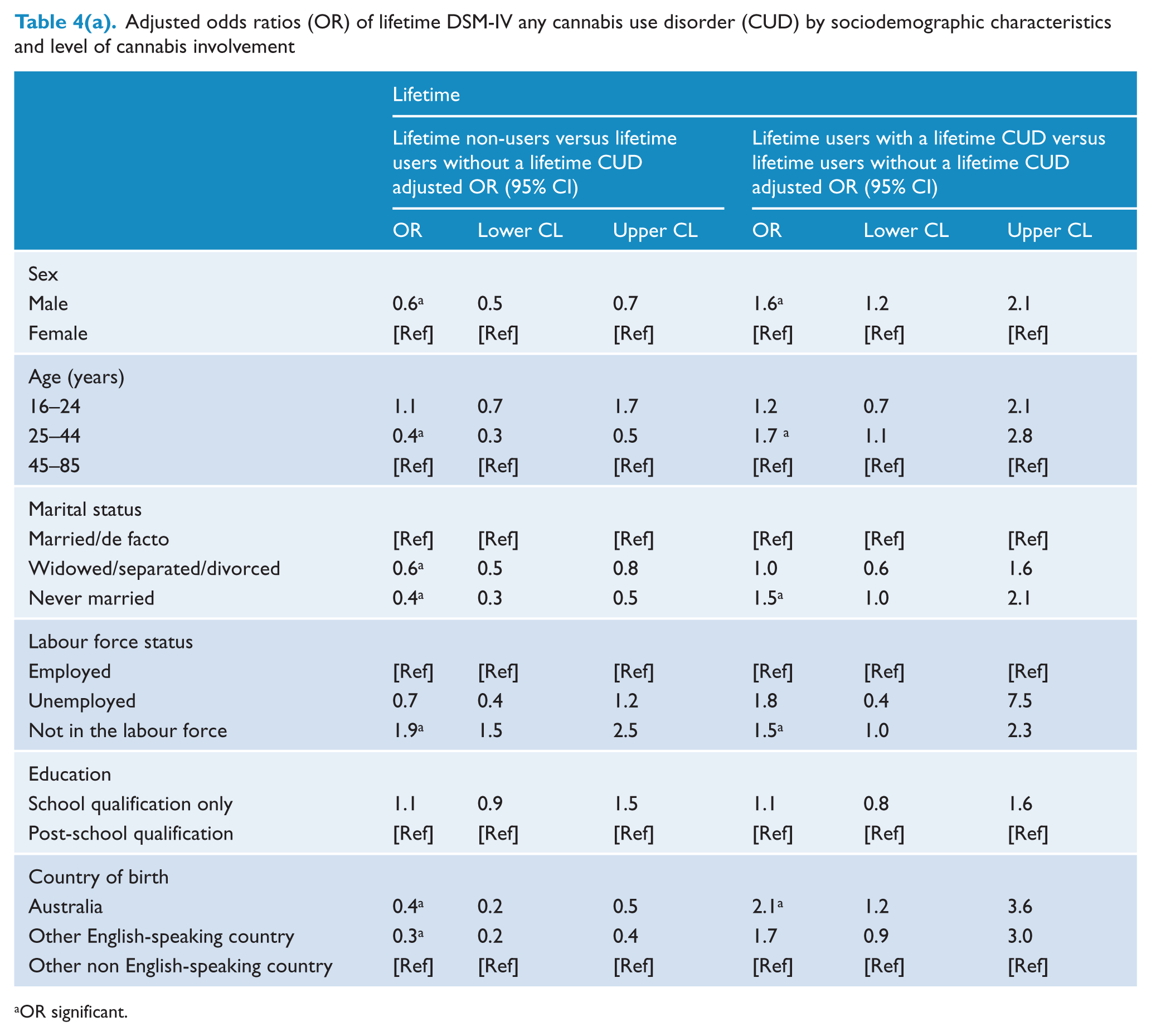
OR significant.
For 12-month disorders (Table 4b), the odds of non-use of cannabis compared with cannabis use without disorder were lower among men and among respondents who were aged 25–44 years, and higher among those who were married and not in the labour force. The odds of 12-month cannabis use disorder in users were higher in males and those aged 16–24 years.
Adjusted odds ratios of 12-month DSM-IV any cannabis use disorder (CUD) by sociodemographic characteristics and level of cannabis involvement
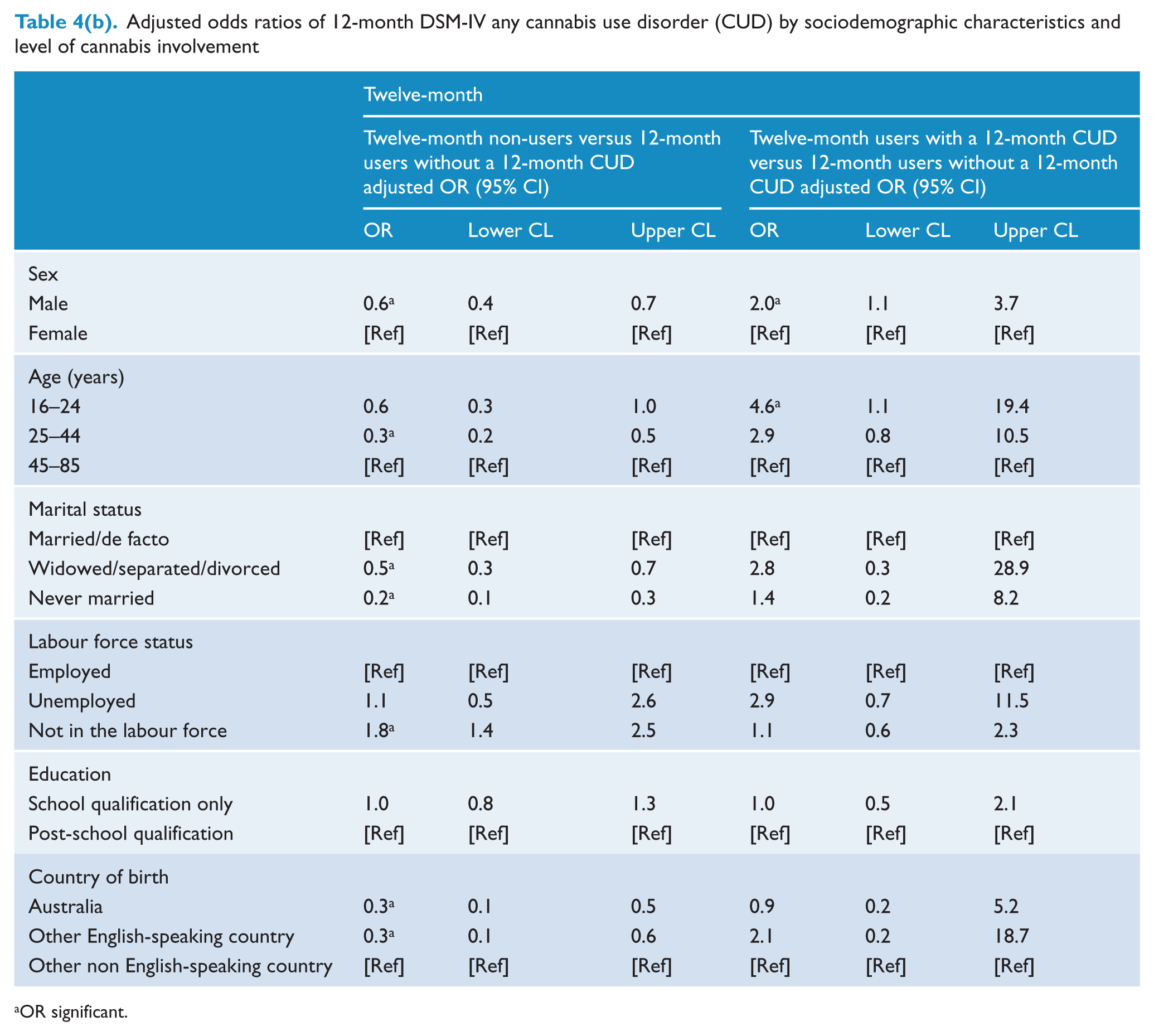
OR significant.
Mean ages at onset of cannabis use and cannabis use disorder were 16.9 (median 17) and 19.8 (median 18) years respectively. Hazard rates for onset peaked at age 20 years for both cannabis use and cannabis use disorder, and decreased in both groups with increasing age (Figure 1).
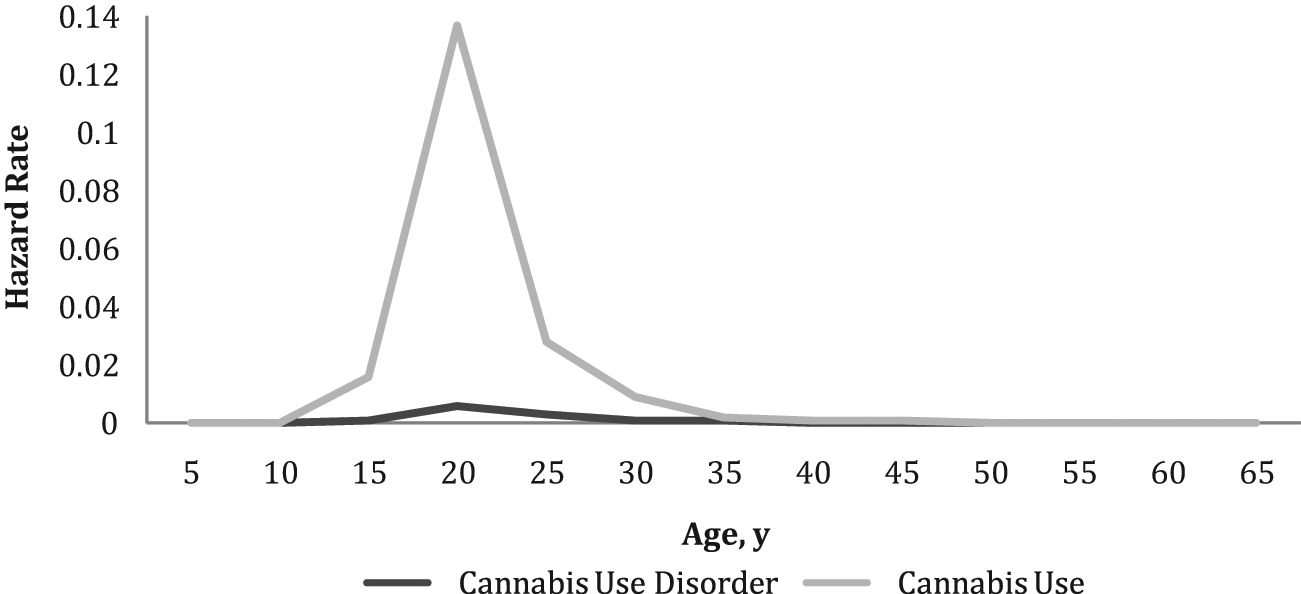
Hazard rates for age at onset of cannabis use and DSM-IV cannabis use disorder.
Associations between 12-month DSM-IV cannabis use disorders and other mental disorders
The weighted prevalence and ORs of comorbid disorders in people with 12-month cannabis use disorders by cannabis involvement and the rest of the sample are presented in Table 5. Cannabis users without a cannabis use disorder had higher rates of major depressive disorder and alcohol abuse and dependence than non-users. Users with cannabis use disorders were more likely than users without such disorders to meet criteria for alcohol abuse (OR 2.8). Persons who had not used cannabis were significantly less likely to have an anxiety disorder (OR 0.7; 95% CI 0.5–0.9) and an alcohol use disorder (OR 0.1; 95% CI 0.1–0.2) than cannabis users without a use disorder. Cannabis users with a cannabis use disorder were significantly more likely to have an affective disorder and an alcohol use disorder than cannabis users without a cannabis use disorder. However, they were no more likely to meet criteria for an anxiety disorder. More than two thirds of persons with a cannabis use disorder had another mental disorder (69.9%; OR 3.8; 95% CI 1.9–7.6) and over half had two or more comorbid mental disorders (52.2%; OR 5.7; 95% CI 2.7–12.0).
Weighted prevalence and odds ratios (OR) of comorbid 12-month DSM-IV disorders.
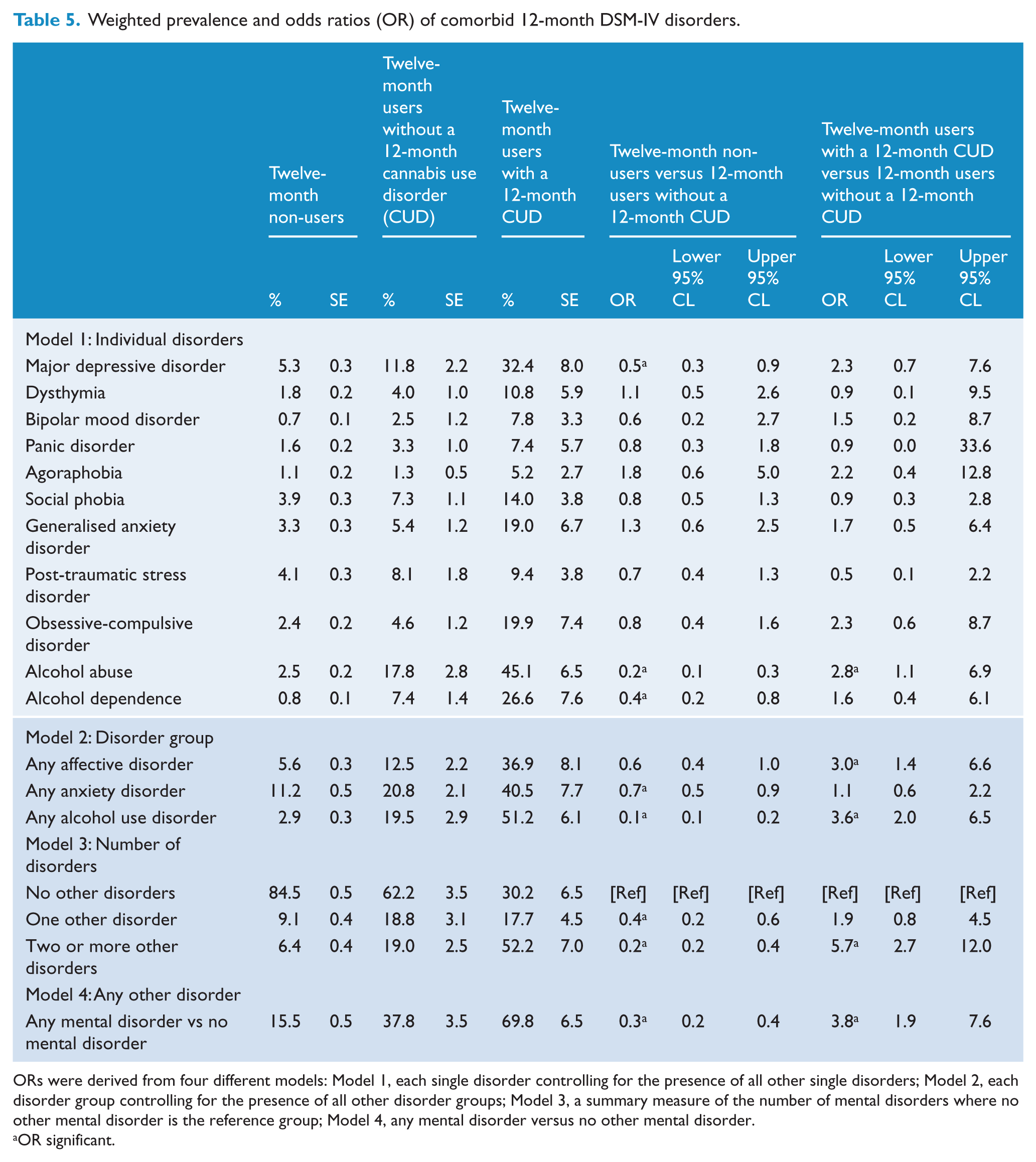
ORs were derived from four different models: Model 1, each single disorder controlling for the presence of all other single disorders; Model 2, each disorder group controlling for the presence of all other disorder groups; Model 3, a summary measure of the number of mental disorders where no other mental disorder is the reference group; Model 4, any mental disorder versus no other mental disorder.
OR significant.
Treatment
One in three (36.2%) people with a 12-month cannabis use disorder reported using health services for mental health problems in the 12 months prior to the interview. There was little difference in help-seeking between males (35.3%) and females (39.3%) with a 12-month cannabis use disorder. The help most commonly sought was from mental health professionals and general practitioners. No demographic characteristics were significantly associated with service use for a cannabis use disorder (sex, age, marital status, labour force status, education, country of birth).
Discussion
In Australia in 2007, 18% of adults had used cannabis at least 5 times in their lifetime and 6% had done so in the past 12 months. One percent of Australian adults experienced a cannabis use disorder in the past 12 months, while 6.2% had done so in their lifetime. Cannabis use and cannabis use disorders were highest among young, unemployed males who had never been married—a finding consistent with previous international studies (Compton et al., 2007). Males had higher rates of cannabis use disorders. reflecting the much higher rates of cannabis use among males when compared with females. The conditional prevalence of cannabis use disorders was also higher among males, although this difference was less marked. Younger age groups also showed greater risk of current cannabis use disorders. Similar findings from the USA (Compton et al., 2007) have been interpreted as reflecting either age differences in cannabis use or, possibly, a younger age of initiation in more recent birth cohorts (Patton, 2007; Swift, 2008; von Sydow, 2001). It may also be a ‘diagnostic bias’, with younger age groups more frequently endorsing cannabis use disorder criteria, although there is little support to date for this hypothesis (Young et al., 2002). In contrast, the highest risk for lifetime cannabis use disorder was in the 25–44 year age group (Hasin et al., 2007).
Several demographic correlates were related to having a cannabis use disorder. Those who were married were less likely than those who were not to have a cannabis use disorder. This may be because being single increases the risk of developing a cannabis use disorder, or because people with cannabis use disorders may be disadvantaged in forming relationships and therefore more likely to be unmarried or divorced, or both. The unemployed were more likely to have a lifetime cannabis use and cannabis use disorder than those in the labour force. This could be because people with cannabis use disorders find it difficult to find employment or, alternatively, because those who become unemployed or who leave the labour force may be more likely to use cannabis, and, hence, are at increased risk of a cannabis use disorder (Fergusson and Boden, 2008). While cross-sectional surveys, such as the current one, provide little data on the causal relationship between cannabis use and outcomes such as employment, evidence from longitudinal studies suggests that increasing cannabis use is associated with failure to obtain school and university qualifications (Horwood et al., 2010). Thus, while the current cross-sectional analysis found no statistically significant relationships between education and cannabis use disorders, previous longitudinal research suggests that educational attainment may mediate the relationship between employment and cannabis-related problems.
Individuals who had a cannabis use disorder in the 2007 NSMHWB also had high rates of other mental disorders, particularly alcohol use and affective disorders. Those with cannabis use disorders were nearly four times more likely to have a comorbid mental disorder than those who used cannabis but did not have a cannabis use disorder. Cannabis use was also associated with affective disorders, with those who had never used cannabis being less likely to have an affective disorder than cannabis users without a disorder. Hypotheses about the nature and casual relationships between comorbid disorders cannot be fully examined in cross-sectional epidemiological studies such as the 2007 NSMHWB, and it is likely that the causal relationships operate in both directions and vary with age (Cerda et al., 2008).
Few individuals with cannabis use disorders sought treatment for their mental health. As the questions on health service use were asked about seeking help for mental health problems these rates may be an underestimate. However, there seems to be very little change in treatment seeking in the 10 years since the last NSMHWB (Proudfoot and Teesson, 2002; Swift et al., 2001). The lack of health service utilisation among those with cannabis use disorders contrasts with much better rates for treatment of depression in Australia (Slade et al., 2009; Teesson et al., 2010). Similar issues have been observed for alcohol use disorders (Teesson et al., 2010). The lack of health service utilisation among those with drug use disorders has been attributed to stigma, clinical lack of knowledge and lack of public awareness of effective treatments. It is also true that the most commonly available intervention, cognitive–behavioural therapy, reduces cannabis use and cannabis-related issues, but only 15% of people remain abstinent 6–12 months after treatment (Copeland and Swift, 2009). Effective prevention initiatives may provide critical areas of activity given the lack of effective treatments available.
Typically, the onset of cannabis use first occurs during late adolescence or early adulthood, with onset later in life rare. Adolescence is a particularly vulnerable period for the onset of cannabis use disorders and an important target for continued aetiologic and prevention research. The current findings highlight clearly the need for effective prevention and early detection of cannabis use disorders, given the significant detrimental psychosocial outcomes associated with cannabis use (Teesson et al., 2005). There are a number of preventive interventions that have shown to be effective in delaying onset of cannabis use (Conrod et al., 2010) and reducing frequency of use (Newton et al., 2010). The latter program has been found to be acceptable to educators and young people, in part because their confidential internet-delivery style avoids stigmatisation and ensures high implementation fidelity.
Comparison with other national surveys of mental health
Comparisons between the 2007 NSMHWB and nationally-representative surveys of the World Mental Health Survey Initiative are possible a result of the use of the same screening questions in the cannabis use disorder section. The current findings indicate that Australia has lower rates of lifetime cannabis use when compared with the USA and New Zealand (both 42%), and higher rates than Asia, Africa and the Middle East (0.3–11.5%). The rates of use reported herein are similar to those reported in European countries, particularly France (19.0), Germany (17.5) and the Netherlands (19.8) (Degenhardt et al., 2008, Kessler and Ustun, 2004, Kessler et al., 2005, Wells et al., 2006). These findings are the first to put Australia in an international context.
Comparison of the lifetime and current cannabis use disorder rates to the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) survey found a marginally lower lifetime prevalence of cannabis use disorder in Australia (6.2%) than the USA (8.5%) (Compton et al., 2007, Wells et al., 2006). This difference may well reflect a real difference in prevalence, as well as differences in screening thresholds and a somewhat larger age range in the Australian sample. Comparisons, such as those undertaken by previous surveys in the US and Australia, are required (McBride et al., 2009; Teeson et al., 2006).
Comparisons between the 1997 and 2007 Australia NSMHWB surveys should be made cautiously. In the 1997 survey, 2.0% met the criteria for a 12-month cannabis use disorder compared with 1.0% in 2007. Overall rates for a 12-month cannabis use disorder are lower in 2007 than in 1997. This may be owing to differences in the sample characteristics (e.g. 1997, 18–85 years), differences in number or type of respondents (e.g. response rates were 78% in 1997 versus 60% in 2007) or differences in interview procedures. Specifically, the 2007 survey included questions about lifetime in addition to past 12-month cannabis use and symptoms, a difference in perspective that may have influenced reporting of symptoms. More research on these methodological issues would be helpful for interpreting cross-survey comparisons. These methodological issues notwithstanding, this article supports previous research (McBride et al., 2009; Teeson et al., 2006) in suggesting that Australia has one of the highest rates of cannabis use and cannabis use disorders worldwide.
Limitations
A potential source of error in the current study is the 60% response rate in the survey. A purposive sample of fully non-responding households in two metropolitan areas that was conducted to gain a qualitative assessment of non-response bias (Slade et al., 2009) indicated that the impact of non-response was small at the aggregate level. Owing to the small, non-random nature of the non-response follow-up sample the results were not incorporated into the survey estimation strategy. However, there may be some underestimation of the prevalence of mental disorders among men and young persons. Thus, the rates reported here probably underestimate the rate of cannabis use disorders in the Australian population.
There are limited data on frequency and quantity of use, and the delta-9-tetrahydrocannabinol (THC) content of cannabis products in Australia. The THC content of Australian cannabis products has not been systematically tested; however, a systematic review of international evidence found that increased potency has been observed in some countries, but there is enormous variation between samples, meaning that cannabis users may be exposed to greater variation in a single year than over years or decades (McLaren et al., 2008). It is also possible that changes in the patterns of cannabis use may also increase the amount of THC that is consumed. These changes could include more regular use of more potent cannabis products, such as the flowering tops of the stems and the greater use of water pipes. Compton et al. (2004) suggested that increases in THC concentration might account for apparent increases in prevalence of cannabis dependence in the USA. However, Chen et al. (2005) did not report an expected increase in the risk of developing cannabis dependence problems soon after onset over the same time period. If the THC concentration has increased it may be that users compensate for increased THC concentration (e.g. smoking fractions of a ‘joint’ as opposed to a complete ‘joint’) (Chen et al., 2005).
Conclusions
Cannabis use disorders were more common among males than females, and the prevalence of current disorders was highest among very young adults. This is of particular concern as recent research suggests that early cannabis use may lead to later drug problems (Degenhardt et al., 2010). Service utilisation was unacceptably low. We require a sustained effort to deliver the most effective prevention and treatment responses to persons affected by these disorders and more effective public health measures to prevent the development of cannabis use disorders, especially among young adults.
Footnotes
Funding
MT, KM and WH are supported by the National Health and Medical Research Council. The research conducted in this paper was supported by the National Health and Research Council Project Grant Scheme. The National Survey of Mental Health and Wellbeing was funded by the Australian Government Department of Health and Aging.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.