
Abstract
Objective:
Most data on duration of untreated psychosis (DUP) derives from high-income countries. An inverse relationship between DUP and income and a longer DUP in low- and middle-income (LAMI) countries has been reported. The aim of this study was to compare DUP in a high-income country with that in a LAMI country using the same methodology.
Methods:
The sample consisted of in- and outpatients, aged 15–35 years for the Vienna site and 18–35 years for the Pakistani sites, with first-episode psychosis (FEP). DUP was evaluated using psychiatric interviews, medical charts and the Nottingham Onset Schedule. Differentiated reporting of duration of untreated illness (DUI) from prodrome to start of treatment, and DUP from manifest psychotic symptoms to start of treatment was ensured. Primary outcome measures, DUI and DUP, were measured at a 0.025 level of significance.
Results:
Thirty-one FEP patients in Vienna (mean age 20.03 years, SD 4.2) and 60 FEP patients from the Pakistani sites (mean age 26.15 years, SD 5.29) participated. The mean age in Vienna was younger due to the different age range inclusion criteria. The severity of psychopathology was more pronounced in the Pakistani sample. Log DUP was significantly different between groups (i.e. longer in the Pakistani sample (p=0.001)). Log DUI showed a trend for longer duration in the Vienna sample; however, this did not reach statistical significance (p=0.036). The severity of positive psychotic symptoms was associated with length of DUI in both regions.
Conclusion:
The longer DUP in Pakistan confirms the need to provide affordable treatment for psychosis for young FEP patients in Pakistan and in other LAMI countries. The relatively long period from prodrome to treatment initiation in both regions underlines the need to further establish low-threshold early intervention strategies in order to increase detection rates and reduce factors limiting patients seeking treatment.
Introduction
Since the duration of untreated psychosis (DUP) may be a modifiable factor with a relevant impact, efforts to reduce DUP have been one of the strategies of early detection and intervention research over the last 15 years. Indeed, DUP has been shown to be independently associated with short- and longer-term outcomes in psychosis (Fusar-Poli et al., 2009; Hill et al., 2012; Marshall et al., 2005; Perkins et al., 2005). DUP also seems to correlate with the severity of positive and negative symptoms (Boonstra et al., 2012; Hill et al., 2012) as well as with cognitive deficits (Cuesta et al., 2012). The large majority of data on DUP derives from high-income (HI) countries. Findings in low- and middle-income (LAMI) countries are sparse (Malik et al., 2010; Naqvi et al., 2009; Sharifi et al., 2009; Thirthalli et al., 2011). Large and colleague’s analysis of DUP in LAMI regions found an inverse relationship between DUP and income, as well as an average mean DUP twice as long as that in HI countries (Large et al., 2008a). A meta-analysis has provided evidence that prolonged DUP and poorer outcome exhibit a similar relationship in LAMI and HI countries (Farooq et al., 2009). However, there are only few directly comparative studies (Cascio et al., 2012; Iyer et al., 2010; McLean et al., 2012). Even fewer studies have directly compared DUP in different countries and cultures using the same methods and instruments (Iyer et al., 2010).
The aim of the present analysis was to fill this gap by assessing differences in DUP in a clinical setting in Vienna, Austria, as representative of a HI country, versus DUP in clinical settings in Lahore, Pakistan, as representative of a LAMI country, using the same methodology. Furthermore, we aimed to assess cross-cultural differences in the first presentation of psychotic disorders, such as psychopathology at onset and its relationship to DUP.
Methods
Sample
The sample consisted of a consecutive series of in- and outpatients, aged 15–35 years for the Vienna site and 18–35 years for the Pakistani sites, with a first episode of psychosis (FEP) who were currently psychotic as evidenced by Positive and Negative Syndrome Scale (PANSS; Kay et al., 1987) scores of 3 or more on the items delusions, hallucinations, conceptual disorganisation and unusual thought content. The duration of previous antipsychotic treatment for the diagnosis of FEP was restricted to a maximum of 6 months (± 2 months). Exclusion criteria included the use of illegal psychotropic substances at the time of assessment (in order to exclude acute effects on psychopathology ratings), organic mental diseases, mental retardation and insufficient command of the local language. Patients were recruited at the Medical University of Vienna, Austria, as well as at the psychiatric departments of the following hospitals in Pakistan: Fountain House, Lahore; Sir Ganga Ram Hospital, Lahore; Ahbab Hospital, Lahore and District Headquarter Hospital, Faisalabad. Patients were referred to the study teams by their treating clinicians if they believed that criteria for FEP were met; additionally, in Vienna, in- and outpatient clinicians were regularly addressed by the study team regarding patients with FEP.
Procedure
Data derived from the Vienna site were initially collected for a multicentre intervention study, the Cognitive Behavioural Case Management study (Edwards et al., 2008), and approval was given by the latter’s management to publish the Vienna data. Some data from the Pakistani sample were published by Malik and colleagues in 2010 (Malik et al., 2010). The study was approved by the local ethics committees in the relevant countries. Informed consent to participate in the study was obtained from all patients or their guardians before participation in the study.
Assessments
DUP was evaluated using psychiatric interviews, medical charts and the Nottingham Onset Schedule (NOS; Singh et al., 2005). The NOS is an interviewer-rated questionnaire that allows for the assessment of key points in the development of psychosis (i.e. prodromal symptoms, first psychotic symptoms, established illness and start of treatment). All sources of information (i.e. the clinical files, patients and informants) were used to assess onset dates. Two measurements were taken into account for this analysis: duration of untreated illness (DUI), the time from first prodromal symptoms to start of treatment (in weeks); and DUP, the time from first frank psychotic symptoms to start of treatment (in weeks).
Premorbid levels of functioning were derived from the Premorbid Adjustment Scale (PAS; Cannon-Spoor et al., 1982), which evaluates social and academic functioning during the different stages of childhood, adolescence and adulthood.
Current psychopathology and level of psychotic symptomatology for inclusion in the study were assessed with the PANSS (Kay et al., 1987).
Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR) criteria were used for the assessment of diagnoses in both countries. Ascertainment of diagnoses was made by consensus between one psychiatrist and two psychologists in the Pakistani sites; for the Viennese sample consensus diagnoses were reached in accordance with the treating team and two psychiatrists in the study team.
Statistical analysis
Measurement and reporting of DUP was partly achieved following the recommendations of Large et al. (2008b) (i.e. in additional to the mean, standard deviation (SD), medians and range, logarithmic adaptation of DUP scores was reported in order to correct for skewed data). Further analyses using log DUP were performed using the non-parametric Mann–Whitney U-test due to some remaining outliers. Since both log DUI and log DUP were primary outcome measures, they were tested at a significance level of 0.025 instead of 0.05. Secondary outcome measures (i.e. the relationships between DUP and other variables) were calculated using Spearman’s correlation. The analyses of secondary outcome measures were exploratory in nature. The Mann–Whitney U-test was applied for the calculation of between-group means of psychopathology and premorbid adjustment scores. Nominal data were compared using chi-squared calculations.
Results
Description of patient samples
The Vienna site recruited 31 FEP patients (35.5% female). Sixty FEP patients (31.7% female) were recruited at the Pakistani sites. There was no difference in sex distribution between the two regions. As expected, owing to differences in the inclusion age, there was a significant age difference between the sites, with patients in Vienna being younger (20.03 years, SD 4.2) than those in Pakistan (26.15 years, SD 5.29) (p=0.001). Patients also differed with respect to marital and educational status, with higher levels of education in Vienna and more married individuals in the Pakistani sample. Table 1 includes details on the distribution of diagnoses, marital status and education status.
Description of study sample.
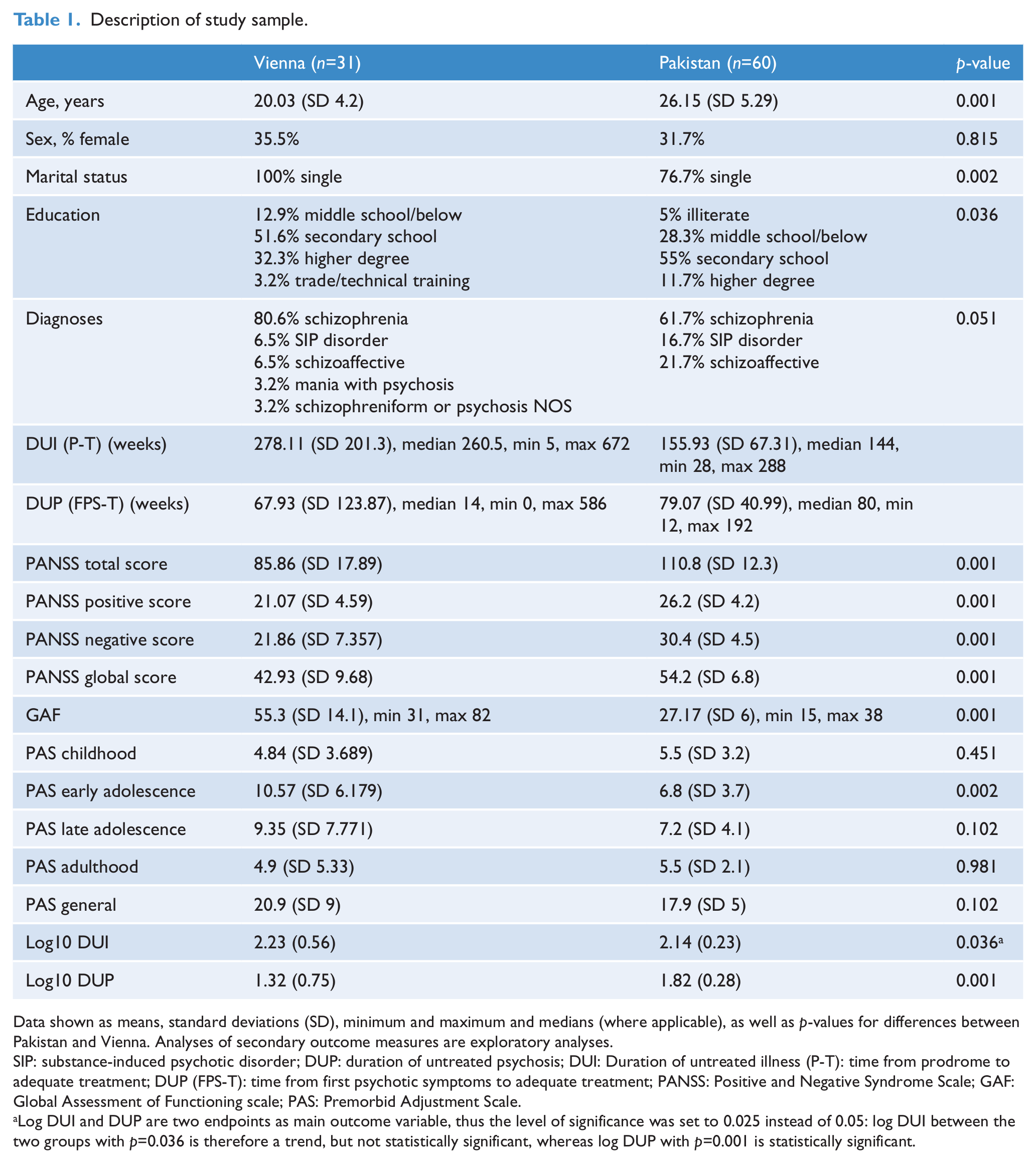
Data shown as means, standard deviations (SD), minimum and maximum and medians (where applicable), as well as p-values for differences between Pakistan and Vienna. Analyses of secondary outcome measures are exploratory analyses.
SIP: substance-induced psychotic disorder; DUP: duration of untreated psychosis; DUI: Duration of untreated illness (P-T): time from prodrome to adequate treatment; DUP (FPS-T): time from first psychotic symptoms to adequate treatment; PANSS: Positive and Negative Syndrome Scale; GAF: Global Assessment of Functioning scale; PAS: Premorbid Adjustment Scale.
Log DUI and DUP are two endpoints as main outcome variable, thus the level of significance was set to 0.025 instead of 0.05: log DUI between the two groups with p=0.036 is therefore a trend, but not statistically significant, whereas log DUP with p=0.001 is statistically significant.
There were significant differences in all PANSS subscales and in the PANSS total scores, as well as in the Global Assessment of Functioning (GAF) scores, between the groups, with more severe psychopathology and lower global levels of psychosocial functioning in the Pakistani sample (Table 1).
With respect to the PAS, only premorbid functioning during early adolescence differed significantly between the groups, with lower scores (i.e. higher adjustment) in the Pakistani sample (Table 1).
DUP/DUI
The means and medians of the DUI and DUP are reported in Table 1. The median DUI was longer in Vienna, whereas the median DUP was longer in Pakistan. Only the log DUP was significantly different between the groups, with a longer duration from frank psychotic symptoms to start of treatment in the Pakistani sample. The log DUI showed a trend for a longer duration in the Vienna sample; however, this did not reach statistical significance (Figure 1).
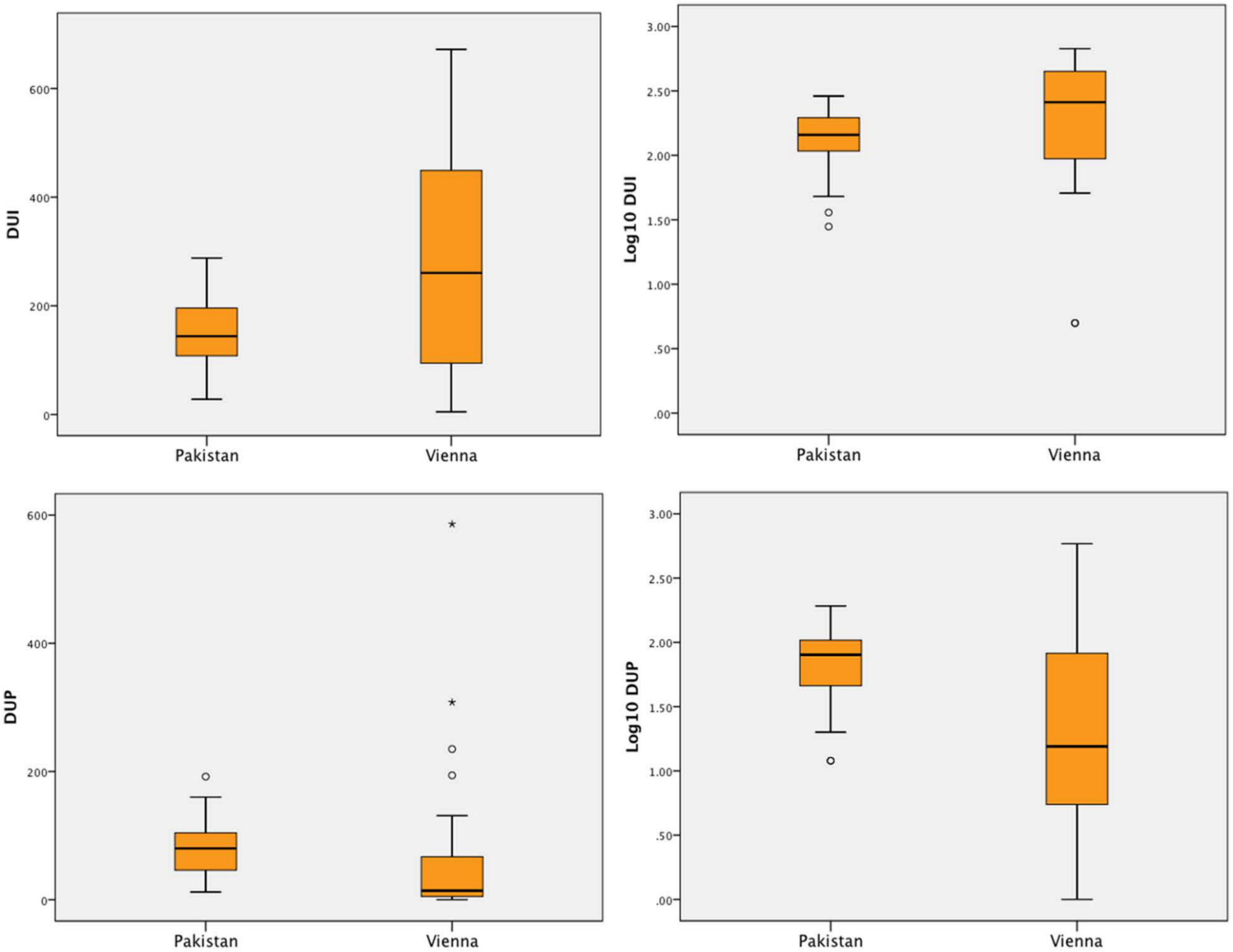
Boxplots of DUI and DUP as well as logarithmised DUI and DUP. (DUI time from prodrome to adequate treatment; DUP time from first psychotic symptoms to adequate treatment.)
In the Vienna sample, 43.3% (n=13/30) of FEP patients received adequate antipsychotic treatment within 12 weeks, whereas only 3.3% (n=2) of patients did so in the Pakistani sample. A total of 16.6% (n=5/30) of patients in the Vienna sample had a DUP of more than 2 years compared to 26.6% (n=16) in the Pakistani sample.
Relationship between DUP and other variables
In the Pakistani sample, the log DUI and log DUP correlated positively with age (r=0.37, p=0.004 and r=0.26, p=0.045, respectively), and positive (r=0.36, p=0.004 and r=0.29, p=0.022, respectively), global (r=0.32, p=0.013 and r=0.35, p=0.006, respectively) and total scores (r=0.41, p=0.001 and r=0.43, p=0.001, respectively) on the PANSS, and negatively with premorbid functioning in late adolescence (r=−0.30, p=0.018 and r=−0.32, p=0.013, respectively).
In the Vienna sample, there was a single positive correlation between log DUI and PANSS positive scores (r=0.42, p=0.033).
Neither sex, diagnosis, education nor marital status were significantly associated with the log DUI or DUP in either of the two regions.
Discussion
The main findings of this comparative study of DUP in two culturally and economically different regions show that DUP is significantly longer in Pakistan, representative of a LAMI country, compared to Vienna, Austria, a HI country. There were no differences in the length of time between the onset of prodromal symptoms and the beginning of treatment (DUI), although on a descriptive level, the median DUI was longer in Vienna. Previously, a systematic analysis of DUP in LAMI countries has shown an average DUP of 125 weeks compared to 63 weeks in HI countries (Large et al., 2008a). In this sample, DUP, although significantly longer in Pakistan than in Vienna, was lower than the average reported (Farooq et al., 2009; Large et al., 2008a; McLean et al., 2012). However, reports of DUP in LAMI countries exhibit a wide range, from between 23 weeks in a specialised early psychosis setting in Chennai, India – equal to DUP in the compared Canadian site (Iyer et al., 2010) – to 47 weeks in a multi-specialty hospital in north India (Gupta et al., 2010), 64 weeks in Karachi, Pakistan (Naqvi et al., 2009) and 2.6 years in Tamil Nadu, India (McLean et al., 2012).
When looking at the details of DUP distribution, it is noteworthy that there was a large imbalance in the time of presentation in the two regions: more than 40% of FEP patients in Vienna presented for initial treatment within a period of 3 months of onset of psychotic symptoms, while only about 3% of patients in the Pakistani sample did so. On the other hand, patients in the Pakistani group were more severely ill at presentation, and there was an association between the severity of positive, global and general psychopathology and the length of DUP. It is possible that the Pakistani patients were either more severely affected by their psychotic symptoms due to their longer DUP or, conversely, that they initially suffered more severe manifestations of FEP, leading to poorer insight and thus longer pathways to care and hence longer DUP. It is noteworthy that patients in Pakistan were older than in Vienna and that both DUI and DUP were positively associated with age. Furthermore, almost one-third of patients in the Pakistani sample had a DUP of more than 2 years, pointing to a somewhat more chronic course of FEP.
Factors that have been shown to influence DUP in LAMI countries include the accessibility and cost of treatment (Naqvi et al., 2009), gross domestic product (Large et al., 2008a), pathways to care, cultural concepts of illness and help-seeking with traditional healers and non-biomedical strategies (Chaturvedi, 2009; Kulhara and Chakrabarti, 2001; Kulhara et al., 2000; Saravanan et al., 2008; Zafar et al., 2008). All these might underlie the differences found in this analysis; unfortunately, these variables have not been assessed, thus limiting further interpretation at this level. In Pakistan, the state health care system is poorly developed, with only about 2% of the gross domestic product being spent on health and with an out-of-pocket health expenditure of approximately 50% of total health expenditure (World Health Organization, 2012). The mental health system is even less developed, with fewer than 0.5 psychiatrists per 100,000 population for LAMI countries such as Pakistan (World Health Organization, 2012) compared to 14.2 per 100,000 in Austria (OECD, 2011).
Furthermore, stigmatisation due to a lack of adequate knowledge of illness concepts may be more prominent in LAMI countries (Saravanan et al., 2008; Thara and Srinivasan, 2000), particularly in Pakistan (Zafar et al., 2008). Zafar and colleagues (2008) have demonstrated that in Pakistan illness attribution, sex, education, religion and family structures play an essential role in the help-seeking behaviour of relatives of people exhibiting psychotic symptoms.
Social structures in HI countries, such as marked individualism and loss of family bonds, as well as the biomedical conception of illness and better access to care, may result in earlier help-seeking or fewer treatment trials of complementary and alternative non-biomedical medicines than in the LAMI countries (Naqvi et al., 2009; Zafar et al., 2008).
The most important association found between DUP and the other variables was that of the untreated period in the prodrome (DUI), as well as from frank psychotic symptoms to treatment (DUP) with psychopathology at first presentation. Since patients in the Pakistani sample were also more significantly affected by psychotic symptoms than those in Vienna, the direction of causality can be speculated upon: does DUP truly differ between these two regions, or is this discrepancy due to an underlying difference in severity of illness? Some authors argue that FEP patients in LAMI countries may seek help with non-biomedical strategies and access medical treatment only when they fail to respond to the former, thus leading to a negative selection bias (Chaturvedi, 2009).
This is one of the few studies comparing DUP in economically and culturally different countries using the same instruments (Iyer et al., 2010) and, even more importantly, using a standardised instrument for the assessment of DUP. Furthermore, care was taken to report DUP measures as adequately and representatively as possible. In order to account for outliers and skewed distribution, logarithmic DUP values were used, as recommended in the previous analysis by Large et al. (2008b). The socio-demographic characteristics of the two groups appear quite representative of their respective regional backgrounds; differences in educational level might indeed enhance the significant differences in length of DUP in the two regions (Srinivasan and Thara 2001; Zafar et al., 2008).
In spite of these strengths, the study suffers from certain limitations related to the nature of a retrospective assessment of DUP, such as possible recall bias. Furthermore, factors such as insight, cultural perception of illness and pathways to care were not available for analysis. This is unfortunate since the positive correlation between positive psychotic symptoms – especially mistrust and paranoid ideations – and longer time from prodrome to treatment in both regions might in fact be due to increased lack of insight, which could be a hindrance in seeking help. Additional, preferably longitudinal, studies, starting at the high-risk for psychosis state, are needed to further explore this association on a cross-cultural level. Lastly, the sample size and the excess of male patients, the reasons for which can only be speculated upon, limits the generalisability of the results, and inter-rater reliability assessments between the two sites were not possible.
Conclusion
Both the DUP and psychopathology at initial presentation were more pronounced in the LAMI sample compared to the HI sample. The longer DUP in Pakistan confirms the need to provide affordable treatment for young FEP patients in Pakistan and in other LAMI countries. The severity of positive psychotic symptoms was associated with the length of DUP in both regions, and loss of insight during the development of illness might influence pathways to care. The relatively long DUI from prodrome to treatment in both regions underlines the need to further establish low-threshold early recognition and intervention strategies for symptomatic high-risk patients in order to increase detection rates and reduce factors limiting help-seeking for this group of vulnerable young people.
Footnotes
Acknowledgements
We acknowledge the approval of the Cognitive Behavioural Case Management (CBCM) trial’s management to publish the Vienna site’s data. Ingrid Salazar and Sherilyn Goldstone edited the manuscript.
Funding
The pharmaceutical companies Lilly and Pfizer, Pakistan, financially supported the parts of the project conducted in Pakistan. The Austrian part of the original Cognitive Behavioural Case Management (CBCM) study was supported by a grant from the Anniversary fund of the Austrian National Bank.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.