
Abstract
Objective:
Immigrants’ mental health is a growing public health concern. Neighbourhood characteristics in the host society may contribute to the poor mental health observed among immigrants. In this study, we aimed to investigate the association between neighbourhood-level social fragmentation and socioeconomic characteristics with psychological distress among immigrants and non-immigrants living in Australia.
Methodology:
We conducted cross-sectional secondary data analysis of 228,039 participants from the Sax Institute’s 45 and Up Study, with psychological distress measured with the Kessler 10 (K10) and area-level social fragmentation and economic advantage/disadvantage measured at the statistical area level 1 (areas containing approximately 400 people). Multilevel logistic models were used to examine the extent to which differences across the least and most fragmented and economic advantage/disadvantage neighbourhoods contributed to the prevalence of high psychological distress (K10 score ⩾ 22).
Results:
Immigrants accounted for about 23% of the sample. Slightly more immigrants (34.8%) compared to non-immigrants (32.9%) lived in fragmented areas. Although immigrants were over represented in areas with socioeconomic advantage (40% vs 33.9%), the prevalence of high psychological distress in neighbourhoods with higher social fragmentation and socioeconomic disadvantage was higher in immigrants than non-immigrants. Immigrants had 17% (95% confidence interval = [12%, 22%]) higher odds of having high psychological distress compared to non-immigrants. There was no evidence of an interaction between social fragmentation or socioeconomic disadvantage and immigrant status. Living in fragmented or socioeconomically disadvantaged areas was associated with higher psychological distress among immigrants and non-immigrants. English as a second language and low annual income were significant predictors of psychological distress in immigrants over and above area-level characteristics.
Conclusion:
Immigrants are vulnerable to mental health issues, but the characteristics of the area they live in are also important. Helping immigrants settle into well-integrated and economically advantaged areas may decrease the possibility of mental health issues.
Introduction
There is an unprecedented and rapid increase in the number of international migrants worldwide, from 173 million in 2007 to 258 million in 2017 (United Nations, 2017). Australia is considered a country of immigrants. Australia was inhabited by the Indigenous people before the British settlers arrived in 1788 (Krupinski, 1984). Australian immigration increased rapidly with the introduction of skilled-base visas in 1970. In recent years, new immigrants have been from diverse ethnical and cultural backgrounds compared to the previous White and European immigrants (Bastian, 2012). In addition, since 1977, programmes have also been granted to refugees, and recent estimates now reveal that approximately 4% of Australian immigrants are refugees (Karlsen, 2016). At present, Australia has the ninth largest immigrant population in the world (United Nations, 2017) and foreign-born immigrants account for one-third of the Australian population (Australian Bureau of Statistics, 2017–2018).
Immigrants leave their origin countries for a variety of reasons, including lifestyle and career-related factors, economic hardships, escape from war, persecution and natural disasters (Stimson and Minnery, 2016). Despite some evidence which suggests that immigrants have better mental health when compared to the host population (Alegria et al., 2017), migration is associated with higher risk of mental illness in pre-migration, migration and post-migration resettlement phases (Kirmayer et al., 2011). Life events before immigration and reasons for immigration are likely to contribute to the higher risk of mental illness (Arévalo et al., 2015; Breslau et al., 2007), and the immigration phase is itself also a stressful experience with potentially negative impacts on mental health (Castaneda et al., 2015). Furthermore, following immigration, the process and experience of acculturation can impact on mental health (Alegria et al., 2017; Breslau et al., 2007). While this acculturation process is affected by individual characteristics (including living conditions, decrease in social or socioeconomic status, lack of social support, language competency and exposure to discrimination and acculturative stress) that may lead to social exclusion of immigrants and increase their vulnerability to poor mental health, the characteristics of the host country are additional factors affecting acculturation (Castaneda et al., 2015). Therefore, characteristics of the host society are factors that should be considered when seeking to understand determinants of immigrants’ mental health.
One host society characteristic likely to be important is social connectedness, which identifies the relationship among members within the community (Manca, 2014). The absence or underdevelopment of connectedness between social groups can lead to socially fragmented communities. A large body of evidence has shown that people living in socially fragmented communities have poor mental health (Congdon, 2012; Curtis et al., 2006; Ivory et al., 2011), potentially mediated by lower levels of social support, which is associated with better mental health (Allardyce et al., 2018; Congdon, 2012). Some evidence has shown that even perceptions of social support can reduce psychological distress among individuals (Brown et al., 2009). Given that immigrants may receive even less support than their non-immigrant counterparts, their mental health may be more affected when living in socially fragmented communities. However, the extent to which neighbourhood social fragmentation affects immigrants’ mental health is currently unclear, including whether the association between neighbourhood social fragmentation and mental health differs between immigrants and non-immigrants.
This study aimed to investigate (1) whether immigrants are more or less likely to live in socially fragmented and/or socially deprived neighbourhoods compared to non-immigrants, (2) whether immigration status or neighbourhood characteristics are associated with psychological distress and (3) whether the association between neighbourhood characteristics and psychological distress is different for immigrants compared to non-immigrants (interactive effect).
Materials and methods
Study areas and participants
We conducted a cross-sectional secondary analysis using baseline data from the Sax Institute’s 45 and Up Study. The 45 and Up Study is a population-based cohort study conducted in the state of New South Wales (NSW, Australia) (Banks et al., 2007). The study aims to investigate healthy ageing among individuals aged 45 years and over (Banks et al., 2007). Participants were recruited by random sampling from the Services Australia (formerly the Australian Government Department of Human Services) enrolment database. More than 267,153 people (equivalent to 10% of the population aged 45 years and over) completed the baseline survey between January 2006 and December 2009 (Comino et al., 2016).
NSW is the most populous state in Australia and hosts the highest number of immigrants in the country (Australian Bureau of Statistics, 2016a). NSW covers a land area of 809,444 km2 representing 17,094 Statistical Area level 1 (SA1). Each SA1 typically has a population between 200 and 800 persons, which allows the separation of areas with different geographic characteristics within suburb and locality boundaries (Australian Bureau of Statistics, 2016b).
All participants with a valid psychological distress score, who were able to be geocoded to the SA1 area (based on their residential address on the enrolment database), were included in this study.
Measures
Exposure variable
Immigrant status was the exposure variable. Participants were classified as immigrant if they were born outside Australia and neither of their parents were Australians. Participants self-reported on their own and their parents’ countries of birth.
Outcome variable
Psychological distress was the outcome variable, measured using the Kessler10 (K10) (Kessler et al., 2002). The K10 assesses non-specific symptoms of psychological distress by asking 10 questions about anxiety and depressive symptoms that a person has experienced in the 4-week period before interview. A five-value response option is used for each question, from 1 (‘none’) to 5 (‘all of the time’). The responses are summed to a total score (possible range: 10–50) where higher scores indicate higher psychological distress. In this study, participants were classified into high (a K10 score of ⩾22) and low distress (a K10 score of <22) according to ABS Health Surveys 2007–2008 (Australian Bureau of Statistics, 2012).
Other variables
Social fragmentation index
The Australian Neighbourhood Social Fragmentation Index (ANSFI) was used to measure neighbourhood social fragmentation (Bagheri et al., 2019). The ANSFI is a social fragmentation index (SFI) at the SA1 level, developed using publicly available information from the Australian Bureau Statistics (ABS). The composite score of social fragmentation is calculated by using (1) population mobility; people living less than a year in the neighbourhood, (2) privately rented households, (3) single-person households, (4) nonfamily households, (5) unmarried persons, (6) households with school-aged children, (7) recently moved in; arrived less than a year, (8) long term stay; have arrived more than 15 years ago, (9) residents living more than 5 years in the neighbourhood and (10) people who report volunteering.
The ANSFI consists of two main components: ANSFI-family and ANSFI-mobility (Bagheri et al., 2019). The ANSFI-family component reflects property ownership and household relationship and the ANSFI-mobility reflects length of residency in the neighbourhood (i.e. less than 1 year or more than 5 years in the neighbourhood) as well as the number of families with school-aged children. Scores on the ANSFI-family and ANSFI-mobility range from −4.4 to 11.6 and −2.8 to 15.4 across the 52,162 SA1s across Australia, with higher scores indicating greater social fragmentation. For this study, the 2011 Australian census data were used to measure ANSFI at SA1 level in the state of NSW, Australia.
Social-economic indexes for areas
Socio-Economic Indexes for Areas (SEIFA), developed by the ABS, ranks areas in Australia according to relative socioeconomic advantage and disadvantage based on information from the 5-yearly Census (Australian Bureau of Statistics, 2011). SEIFA consists of four indexes, and in this study, we used the Index of Relative Socio-Economic Advantage and Disadvantage (IRSAD). The IRSAD ranks areas based on relative socioeconomic advantage and disadvantage in terms of people’s access to material and social resources, and their ability to participate in society. The score for each area is a summary measure of a group of variables related to household income, education, employment, number of cars, mortgages and number of bedrooms. For convenience of presentation, the raw scores were rescaled to a mean of 1000 and standard deviation of 100 to create a new set of standardised scores. Scores on IRSAD range from 664 to 1126, with higher scores indicating a higher advantage and lower incidence of disadvantage.
Other socio-demographic variables
Other self-reported variables used in our analyses were sex (male, female), language spoken at home (English, other), education level (less than secondary school, secondary school graduation, trade or certificate or diploma, university degree), relationship status (partner, no partner), employment status (full-time, part-time, other, not working), annual household income (in AUD: <5000, 5000–9999, 10,000–19,999, 20,000–29,999, 30,000–39,999, 40,000–49,999, 50,000–69,999, >70,000) and time spent per week with friends, on the phone with friends and in a social group (measured separately). Only variables significantly associated with psychological distress (age, sex and social interactions) were included in the final analysis.
Statistical analysis
Statistical analyses were performed using the R statistical software (version 3.3.2). Multilevel logistic regression analysis (package Stats; version 3.3.2 and package Caret; version 6.3–73) was used to account for the hierarchical nature of the data (individuals within neighbourhoods). The analysis was conducted with exposure variables nested through four models (forward stepwise analyses) with SA1 as the random intercept in all models. The nested models were sequentially adjusted for age and sex (model 1), individual characteristics significantly associated with psychological distress in univariate linear regressions (model 2), ANSFI-family and ANSFI-mobility (model 3) and IRSAD (model 4). Additionally, for each model, we tested for an interaction between immigrant status and each nested variable separately.
Subgroup analyses were conducted among immigrants to determine the association between individual characteristics (age, sex, education, annual income, relationship status, age at the time of immigration and the time since immigration) and psychological distress.
Ethical approval and data access
The University of NSW Human Ethics Committee approved the 45 and Up Study. The present specific sub-study was approved by the NSW Population Health Services Research Ethics Committee. Details on accessing 45 and Up Study data are available on the Sax Institute website (www.saxinstitute.org.au/our-work/45-up-study).
Results
Participants’ characteristics
At baseline, 228,039 of 267,000 participants (85%) had K10, SA1 level data and immigration status information (Table 1). Immigrants accounted for about 23% of the sample. Approximately two-thirds of immigrants (69%) originated from predominantly English-speaking countries. Immigrants’ age at arrival varied from infancy to 98 years. Average time since arrival to Australia was 36.5 years. On average, immigrants were a year older and a slightly higher proportion of immigrants (50%) compared to non-immigrants (46%) were male. There was no significant difference in income between groups. A higher proportion of immigrants had a university degree (30%) compared to non-immigrants (23%).
Participants’ characteristics at the baseline of 45 and Up Study.
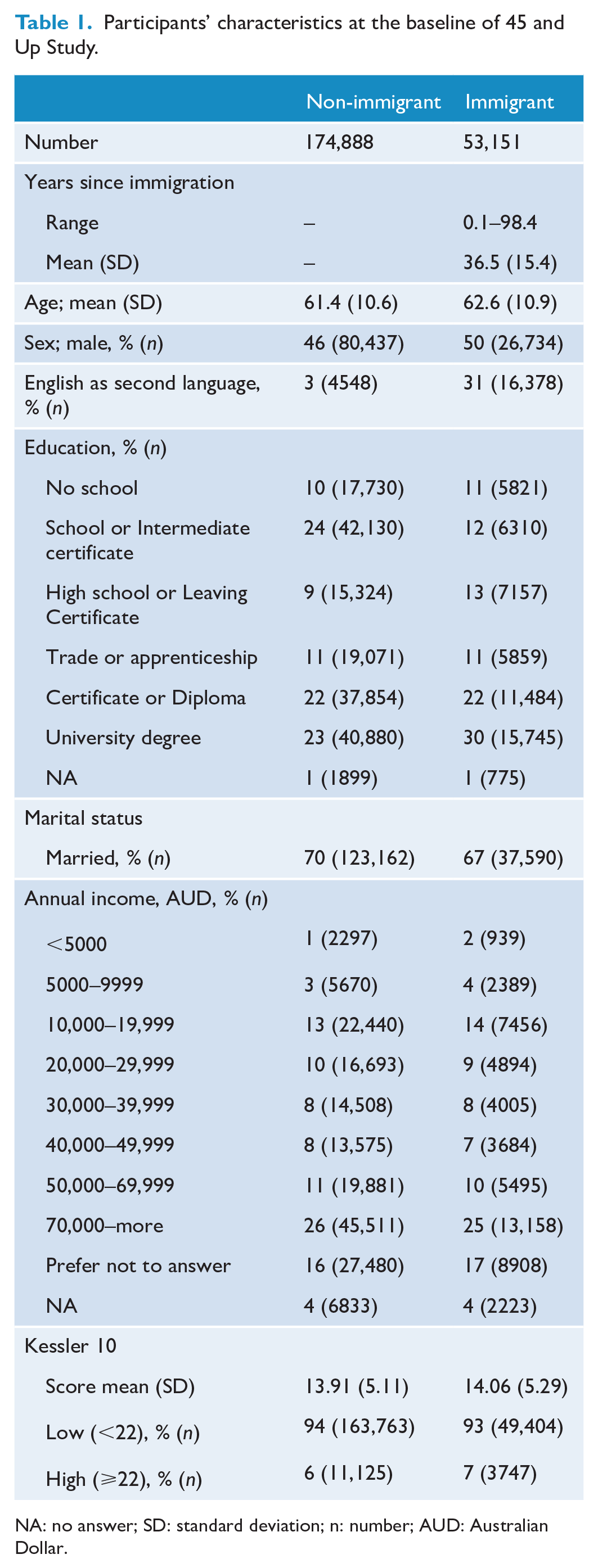
NA: no answer; SD: standard deviation; n: number; AUD: Australian Dollar.
The average K10 score and proportion with high psychological distress was slightly higher among immigrants compared to non-immigrants (14.1% vs 13.9% and 7% vs 6%, respectively; Table 1). Immigrants spent significantly less time interacting socially with friends (visits or telephone conversation) compared to non-immigrants (Table 2).
Individual social interactions in immigrants and non-immigrants and the neighbourhood social fragmentation and socioeconomic status.
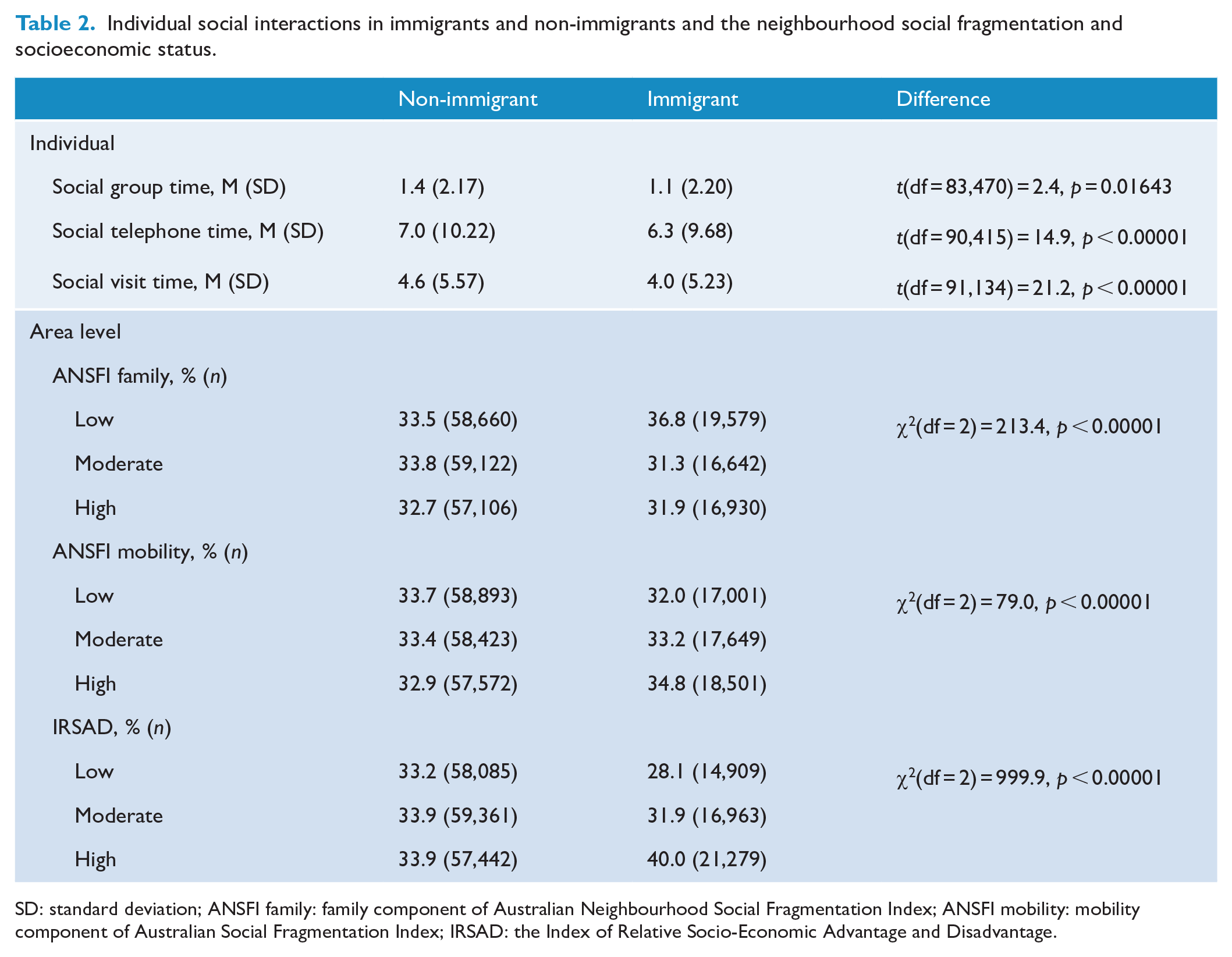
SD: standard deviation; ANSFI family: family component of Australian Neighbourhood Social Fragmentation Index; ANSFI mobility: mobility component of Australian Social Fragmentation Index; IRSAD: the Index of Relative Socio-Economic Advantage and Disadvantage.
Neighbourhood level social fragmentation and socioeconomic status and immigrant status
Non-immigrant Australians were evenly distributed in areas with low, moderate and high ANSFI-family and mobility scores and IRSAD (Table 2). In contrast, a higher proportion of immigrants lived in areas with low (37%) compared to high (32%) ANSFI-family scores (Table 2). Furthermore, a higher proportion of immigrants lived in areas with high (35%) compared to low (32%) ANSFI-mobility scores and high (40%) compared to low (28%) socioeconomic advantage (Table 2).
The prevalence of high psychological distress was higher in immigrants compared to non-immigrants in neighbourhoods with higher social fragmentation (ANSFI-family and ANSFI-mobility) and socioeconomic disadvantage (Figure 1). For example, in highly fragmented neighbourhoods (high ANSFI-family and ANSFI-mobility) with high socioeconomic disadvantage (low IRSAD), the prevalence of high psychological distress was 12.7% in immigrants whereas it was 10.7% in non-immigrants. In contrast, in less fragmented neighbourhoods (low ANSFI-family and ANSFI-mobility) with low socioeconomic disadvantage (high IRSAD), there was no significant difference in psychological distress among immigrants and non-immigrants. The effect of social fragmentation (ANSFI-family and ANSFI-mobility) on the prevalence of psychological distress was more consistent in non-immigrants than immigrants. For example, at low levels of IRSAD, the prevalence of high psychological distress among immigrants was higher at low levels of ANSFI-family than moderate or high levels and it was relatively similar in all ANSFI-mobility levels. In general, the figure shows that the effect of IRSAD on the prevalence of psychological distress is greater than social fragmentation among both immigrants and non-immigrants.
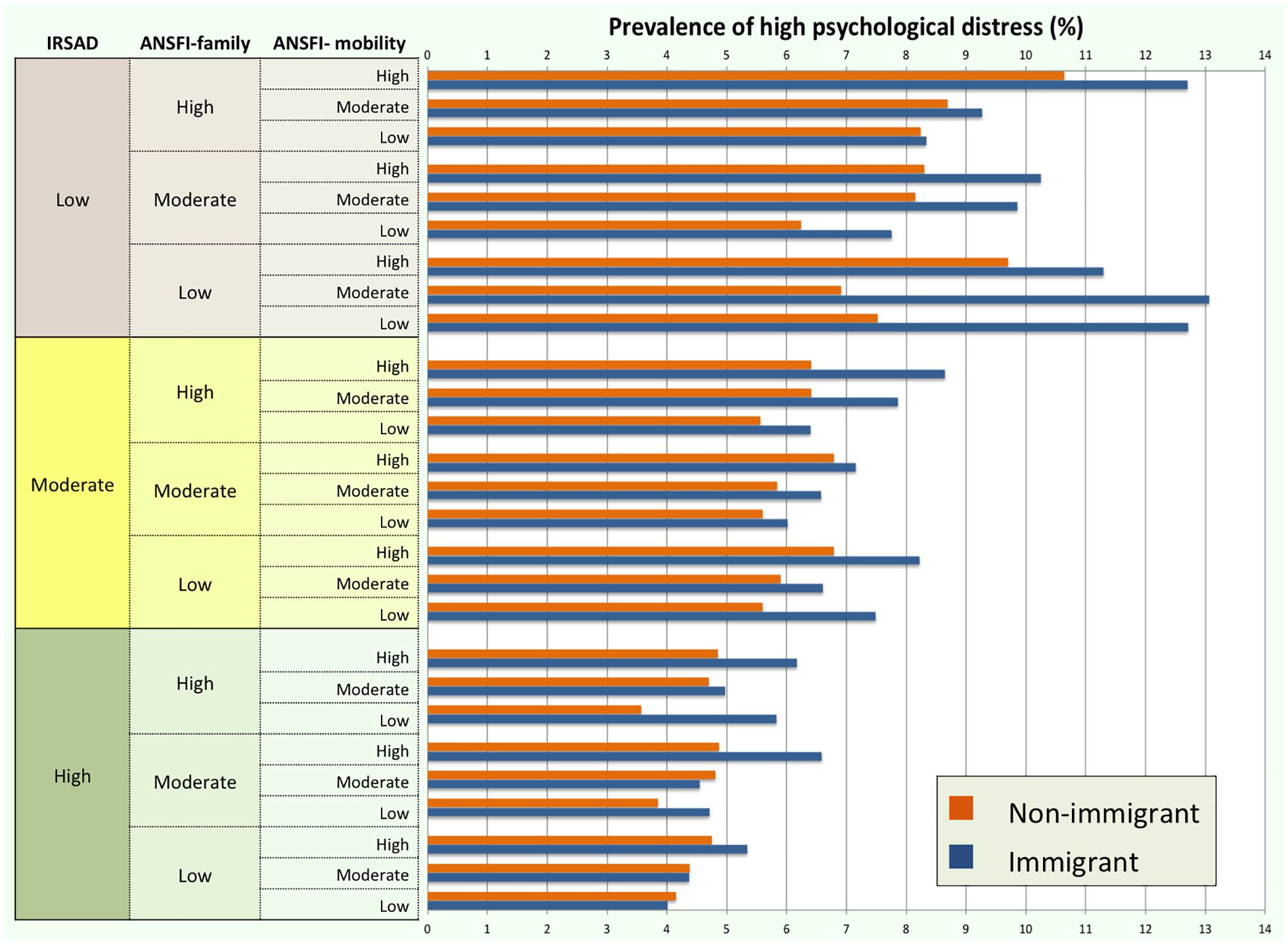
The prevalence of high psychological distress among immigrants and non-immigrants in relation to neighbourhood social fragmentation and socioeconomic measures.
Multilevel logistic analyses
Immigrants had 16% (95% confidence interval [CI] = [11%, 20%]) higher odds of having high psychological distress compared to non-immigrants after adjusting for age and sex (model 1, Table 3). Adjustment for social interaction lowered the odds of having high psychological distress for immigrants compared to non-immigrants to 12% (95% CI = [7%, 17%], model 2). Further adjustment for measures of social fragmentation (ANSFI-family and ANSFI-mobility) (model 3) did not further explain the higher psychological distress in immigrants compared to non-immigrant Australians. Model 3 also showed that living in areas with moderate or high compared to low ANSFI- family was associated with 30% (95% CI = [24%, 36%]) and 67% (95% CI = [59%, 75%]) higher odds of high psychological distress, respectively. Similarly, living in areas with moderate or high compared to low ANSFI-mobility was associated with 9% (95% CI = [4%, 14%]) and 24% (95% CI = [19%, 30%]) higher odds of high distress, respectively.
Multilevel logistic regression models; fixed effects of immigrant status, area level social fragmentation and socioeconomic indexes.
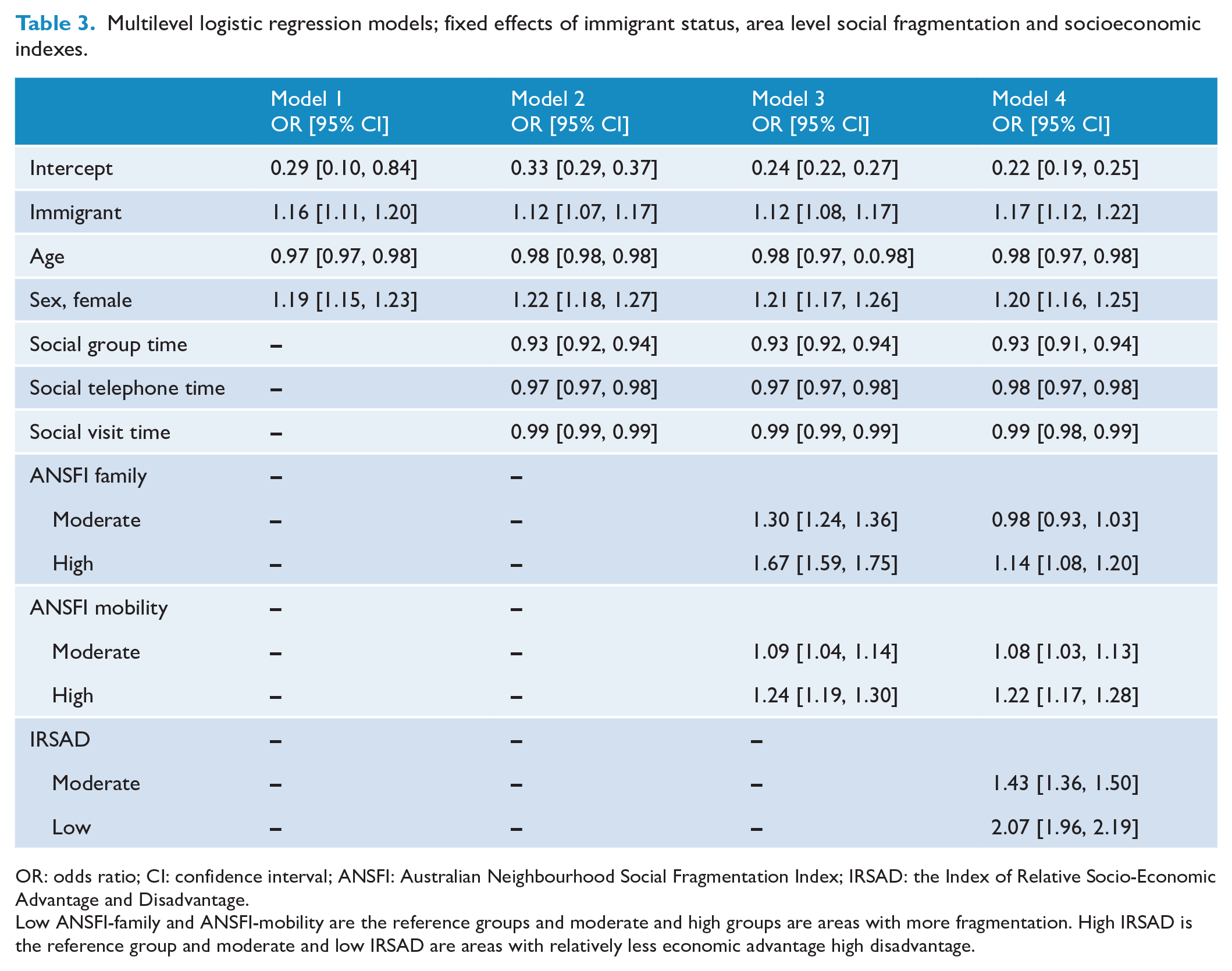
OR: odds ratio; CI: confidence interval; ANSFI: Australian Neighbourhood Social Fragmentation Index; IRSAD: the Index of Relative Socio-Economic Advantage and Disadvantage.
Low ANSFI-family and ANSFI-mobility are the reference groups and moderate and high groups are areas with more fragmentation. High IRSAD is the reference group and moderate and low IRSAD are areas with relatively less economic advantage high disadvantage.
After further adjustment for IRSAD (model 4), the association between ANSFI-family and high psychological distress attenuated, but the association between immigration status and psychological distress was mostly unchanged. Adjustment for IRSAD also had little impact on the association between ANSFI-mobility and psychological distress. The odds of having high psychological distress were 107% (95% CI = [96%, 119%]) and 43% (95% CI = [36%, 50%]) higher in areas with low and moderate compared with a high IRSAD (model 4).
There was no significant interaction between ANSFI family or mobility or IRSAD and migration status, i.e., the effect of ANSFIs and IRSAD on the psychological distress in immigrants and non-immigrants was not different.
Further subgroup analyses in immigrants revealed that age, female sex, speaking a language other than English at home, lower annual income, not having a partner and lower level of education were associated with higher odds of having high psychological distress. The odds of having high psychological distress decreased 3% (95% CI = [3%, 4%]) for each year increased in age, was 8% (95% CI = [1%, 17%]) higher for females than males and 98% (95% CI = [82%, 112%]) higher in those who speak a language other than English at home compared to those who speak English. The odds of having high psychological distress were 35% (95% CI = [30%, 40%]) lower for married people compared to unmarried, 16% (95% CI = [14%, 18%]) lower for each level increase in education and approximately 14% (95% CI = [13%, 15%]) lower for each AUD10,000 increase in annual income. In contrast, age at the time of immigration and total years lived in Australia were not associated with psychological distress.
Discussion
Neighbourhood level characteristics have been investigated as determinants of psychological distress in recent years. In this study, we explored this relationship between immigrants and non-immigrant Australians. Our results showed that in our study sample, immigrants had a slightly higher prevalence of psychological distress compared to non-immigrant Australians, and this appeared independent of their residential neighbourhood characteristics. Additionally, the odds of having high psychological distress were higher in people who lived in socially fragmented neighbourhoods and in areas of higher compared to lower socioeconomic disadvantage, irrespective of immigration status. Living in areas of socioeconomic disadvantage explained some of the association between social fragmentation and increased odds of having psychological distress. Our study further showed that speaking English as a second language and having low annual income was associated with higher psychological distress in immigrants. These findings suggest that factors preventing social engagement, irrespective of whether they are community-level barriers or due to individual barriers such as language or poverty, may increase the risk of psychological distress. Despite being associated with high psychological distress among immigrants, annual income was not associated with high psychological distress among non-immigrants. This is in contrast with findings by Isaacs et al. (2018), who found a strong association between lower income and elevated psychological distress. However, differences in the samples may have also contributed to these differences, for example, the age range in their study was lower (18–64 vs 45–99 years), and the prevalence of high psychological distress was higher than the present study (more than 11% vs 6%). Therefore, it is likely that age-related factors explain, at least in part, the differences in our findings. Non-immigrant middle- and older-age individuals are likely to have stable levels of income, and thus, their income may have a smaller impact on the acute response to recent challenges, given that K10 yields a global measure of distress based on anxiety and depressive symptoms that a person has experienced in the most recent 4-week period.
In this study, immigrants had higher odds of psychological distress in general compared to non-immigrants. This was despite the fact that a larger proportion of immigrants lived in areas of higher socioeconomic advantage. Living in areas of higher socioeconomic advantage was associated with lower psychological distress. Given that immigrants in this study were aged 45 years and over and relatively educated (30% with a university degree), and given that the average time since immigration was more than 36 years, living in areas with higher socioeconomic advantage is not unexpected, particularly when the majority of immigrants were from English-speaking backgrounds. In contrast, new immigrants usually settle in poor neighbourhoods, often in ethnic enclaves (Durbin et al., 2015a), due to financial hardship, a preference to live near people from similar ethnicities or who speak the same language (Castaneda et al., 2015), a lack of recognition of their skills and having lower levels of acculturation due to language barriers (George et al., 2015; Jafari et al., 2010; Tang et al., 2007). Therefore, being older, well educated, from English-speaking backgrounds and longer time since immigration may help immigrants to settle in areas of higher socioeconomic advantage. However, living in areas with economic advantage and still having higher odds of psychological distress indicate that the impact of immigration on mental health may not be limited to recent arrivals, potentially indicating a group requiring ongoing mental health support.
Consistent with previous evidence (Ivory et al., 2011), this study found an association between social fragmentation and higher levels of psychological distress. In this study, we used ANSFI-family to evaluate the attachment and sharing values and the ANSFI-mobility to evaluate mobility and transience in society (Bagheri et al., 2019). Although each of these component indexes measure different aspects of social fragmentation, both were associated with high psychological distress. It is important to note that the proportion of immigrants was slightly higher in areas with low levels of ANSFI-family but lower in areas of low ANSFI-mobility. However, living in fragmented areas did not explain the higher odds of psychological distress in immigrants compared to non-immigrants. Additionally, the association between living in fragmented areas and psychological distress was similar in immigrants and non-immigrants.
English as a second language and low annual income emerged as two predictors of psychological distress among immigrants, over and above area-level characteristics. These findings are consistent with evidence which shows that language difficulties and economic uncertainty interfere with effective acculturation and settlement processes and can increase the risk of mental health issues among immigrants (Alegria et al., 2017; Arévalo et al., 2015; George et al., 2015). For immigrants from diverse cultural and linguistic backgrounds, this experience can be even harder (Donath et al., 2016).
In addition to higher risk of mental health problems, immigrants are also less likely to access or use primary mental health services compared with non-immigrants (Durbin et al., 2015b; Minas et al., 2013). This may relate, at least in part, to communication difficulties due to linguistic and cultural differences, cultural shaping of symptoms and illnesses and fear of negative impact on employment (Kirmayer et al., 2011). Regardless of the reason, lower access to mental health services may further increase their vulnerability to mental health issues.
To the best of our knowledge, this is the first study to investigate the association between area- and individual-level characteristics and psychological distress in immigrants compared with non-immigrants in Australia. Using a quantitative scale for indexing social cohesion and deprivation on a large sample is a key strength of this study. However, the interpretation of the results should be viewed with caution because of a number of limitations. Our sample consisted of middle- and older-aged adults, and thus the findings cannot be generalised to immigrants from other age groups. Furthermore, even in this age group, the sample is from a population-based cohort (with an 18% response rate), with over-sampling of those in higher income groups, people aged over 80 years and those live in rural/regional. Therefore, the extent to which the present results can be generalised to other populations is unclear. Additionally, information on important immigration-related factors impacting immigrants’ mental health after migration were not available in this study. This includes factors such as being a refugee, reason(s) for migration, mental health condition before migration, the timeline and process of migration and experiences of prejudice. These factors and their associations with psychological distress require further investigation.
Conclusion
Although living in socially fragmented neighbourhoods and areas of higher socioeconomic disadvantage is associated with higher psychological distress, regardless of immigration status, being immigrant is additionally associated with higher distress. Furthermore, speaking English as a second language or having lower incomes are determinants of higher psychological distress in immigrants. Helping people to settle into well-integrated and economically advantaged areas after migration and assist them to deal better with acculturation stressors may decrease the possibility of mental health issues. This will not only reduce the demands on health systems but may also help immigrants to participate actively in the new society and develop a cohesive community. However, building socially cohesive neighbourhoods with less socioeconomic disadvantage will ultimately reduce the area-level risk factors and will benefit all vulnerable members of the society, including immigrants.
Footnotes
Acknowledgements
We would like to thank the ANU Research School of Population Health’s support for funding Population Health Excellence Research Award. This research was completed using data collected through the 45 and Up Study (![]() ). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW and partners: the National Heart Foundation of Australia (NSW Division); NSW Ministry of Health; NSW Government Family & Community Services – Ageing, Carers and the Disability Council NSW; and the Australian Red Cross Blood Service. We thank the many thousands of people participating in the 45 and Up Study.
). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW and partners: the National Heart Foundation of Australia (NSW Division); NSW Ministry of Health; NSW Government Family & Community Services – Ageing, Carers and the Disability Council NSW; and the Australian Red Cross Blood Service. We thank the many thousands of people participating in the 45 and Up Study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.