
Abstract
Keywords
Abnormalities of thought and speech have long occupied a central place in clinical descriptions and psychopathological approaches of schizophrenia; Bleuler considered a deflection of associations to be a fundamental feature of the disorder [1], and the two most widely used modern classification systems include disturbances in the form of thought in the diagnostic criteria for schizophrenia [2], [3]. These are generally referred to as ‘formal thought disorder’ but this term includes disturbances that are quite diverse and do not always coexist in the same patient (e.g. ‘poverty of thought’ and ‘loose associations’) [4]. As a consequence, the assessment of formal thought disorder has often been problematic in the past.
Various standardized instruments for the assessment of formal thought disorder have been proposed in order to increase reliability of measurements [5]. One of the most widely used is the Scale for the Assessment of Thought, Language and Communication (TLC) [4]. This scale takes a strictly empirical approach to the assessment of formal thought disorder, based exclusively on the observation of language behaviours. It consists of 18 items, for which explicit definitions and clinical examples are provided; the severity of each item is rated using clearly specified anchor points based on a clinical interview, the conditions of which are also detailed by the author. The validity of the scale has been documented [6]; moreover, good interrater reliability [7–10] and test–retest reliability [11] have also been shown.
Thought, language and communication disorders were initially conceptualized as having only two underlying dimensions, a negative (consisting of poverty of thought, poverty of content and blocking) and a positive one (consisting of the 15 remaining items of the TLC) [12]. Although this conceptualization has proven useful in the discrimination of patients with schizophrenia from those with affective and schizoaffective disorders [6], [13], studies of the factorial structure of the TLC have not provided confirmation for the positive-versus-negative distinction. In most cases a three- to seven-factor structure has been described [6–8], [14]; even the simpler, two-factor models do not distinguish between positive and negative thought disorder, but rather between verbal productivity (reflected in poverty of speech and pressure of speech) and disconnection (consisting of the remaining 16 items) [10], [15].
The aim of the present study was to assess the psychometric properties and the factorial structure of the Greek translation of the TLC. Specific mention should be made to the patient sample: most of the studies on the TLC (with the exception of Bazin et al. 2002 [7]) have been conducted with acutely admitted patients, but thought disorder is known to improve with treatment [10], [16–18]. This improvement seems to be more prominent for some aspects of thought and language disturbances than for others [6], [19], raising the possibility that the interrelations among the various TLC items might be different in clinically stabilized patients. Thus, for the present study we chose to investigate a mixed sample of patients with psychotic disorders at various stages of their illness (acutely ill inpatients, stable outpatients and chronically hospitalized patients).
Method
Translation procedure
With permission of its author, the TLC was translated into Greek by one of the authors (CA). The ensuing proof was submitted to blind back-translation by a native speaker of English (MHK). Finally, the back-translation was compared to the original scale, revised accordingly and translated once again into Greek.
Participants
Subjects were 103 patients (69 male, 34 female) with psychotic disorders randomly recruited from two acute treatment units (n = 51, 49.5%), two outpatient clinics (n = 37, 35.9%) and one chronic hospitalization facility (n = 15, 14.6%). The mean age of patients was 38.8±12.0 years (range = 18–68 years), and their mean level of education was 10.6±3.6 years (range = 3–18 years). All patients were diagnosed according to DSM-IV criteria [2]. Diagnosis was confirmed with the Greek version (translation-adaptation to the Greek language by S. Berati) of the Mini International Neuropsychiatric Interview (4.4) (MINI) [20]. The majority of patients (n = 93, 89%) had a diagnosis of schizophrenia (paranoid: n = 70, 68.0% of the total sample; residual: n = 16, 15.5%; disorganized: n = 3, 2.9%; undifferentiated: n = 3, 2.9%; catatonic: n = 1, 1.0%); moreover, there were four patients (3.9%) with a diagnosis of brief psychotic disorder, and two patients (1.9%) each with schizophreniform disorder, schizoaffective disorder, and psychotic disorder not otherwise specified. The majority of patients (83.5%) were being treated with atypical antipsychotics, 6.8% with typical antipsychotics, while 8.7% of patients were receiving both typical and atypical antipsychotics. Moreover, 22.3% of patients were receiving anticholinergic agents (mainly biperiden), 29.1%, benzodiazepines and 15.5%, other agents (mostly antidepressants and anti-epileptics). All patients gave their informed consent to participate in the study, which was approved by the Department of Neuroscience and by the General Council of the Medical School of the Aristotle University of Thessaloniki.
The TLC was assessed by two of the authors (AC and IP) based on a 20 min clinical interview according to the instructions of the author of the scale [4], [12]. The interrater reliability (weighted κ) was measured in a subsample of 31 patients who were jointly interviewed by the two raters. The correlations of the TLC factors derived from the analyses with sex, age, education, age at onset and length of illness were explored using Pearson's correlation coefficient. Moreover, t-tests were conducted in order to investigate any differences between acutely hospitalized patients and outpatients in the TLC dimensions obtained.
Results
Frequency and severity of TLC items and interrater reliability
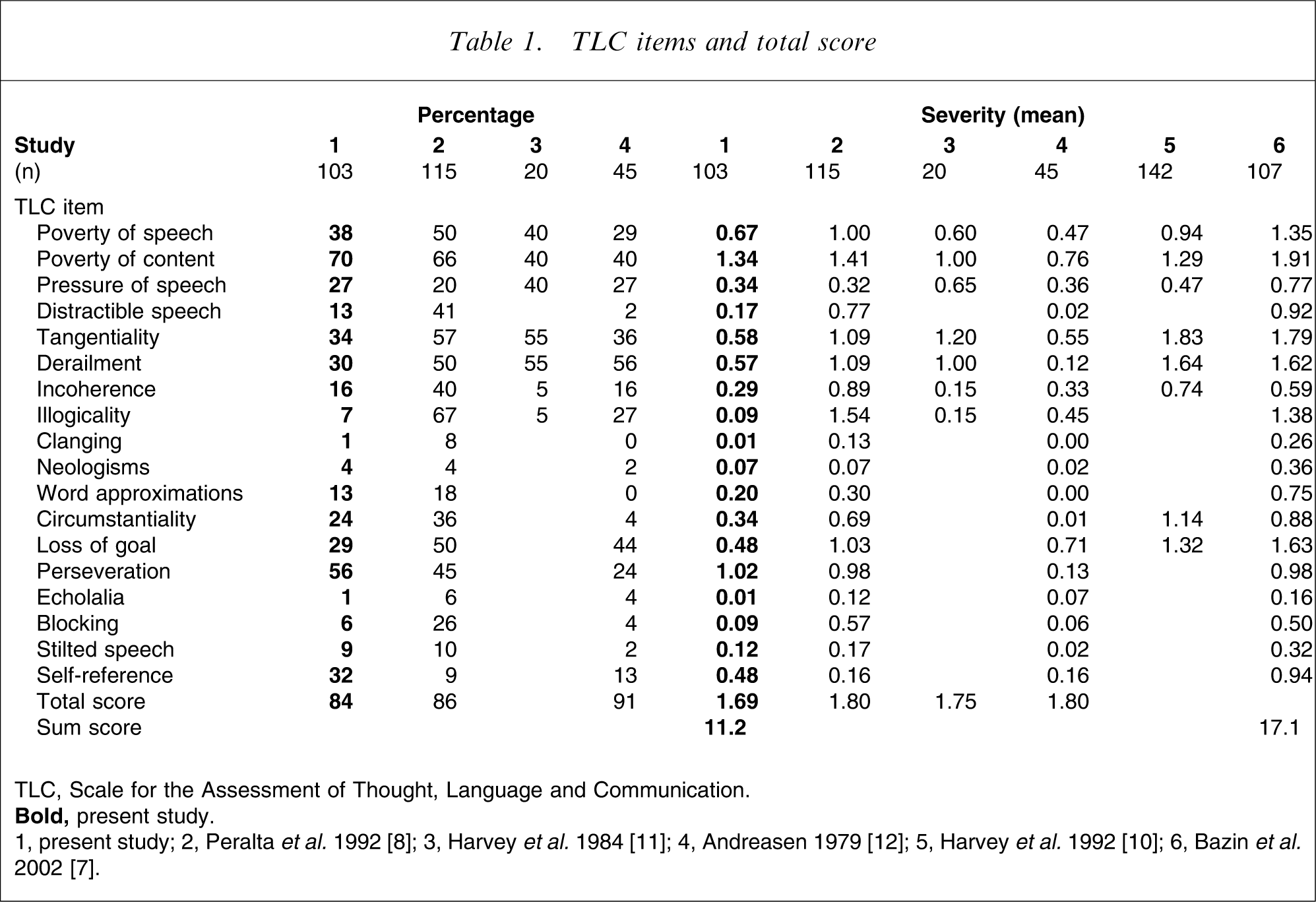
Only 16.5% of patients exhibited no formal thought disorder; mean frequency and severity for the TLC items and the total score appear in Table 1, along with corresponding values from other studies using the TLC. Patients with schizophrenia did not significantly differ from patients with other psychotic disorders in TLC total score (U = 323.000, p = 0.75), sum score (U = 343.500, p = 0.97) or separate item scores (all ps > 0.1).
TLC items and total score
Interrater reliability was good to excellent (≥0.60) for 15 items of the scale and moderate for distractible speech (0.47), illogicality (0.42) and perseveration (0.50). The total TLC score achieved excellent interrater reliability (0.87; Table 2).
Interrater reliability for TLC items and total score
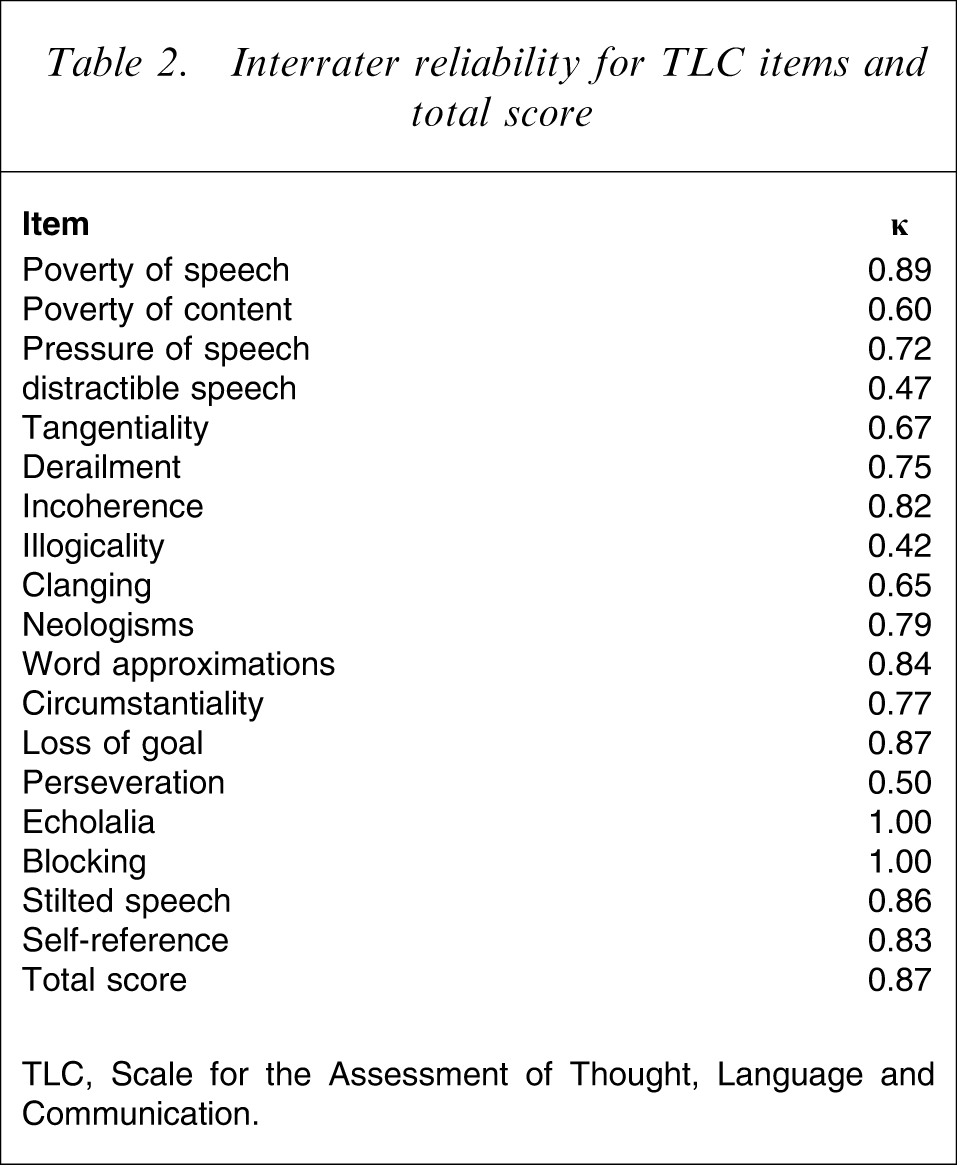
TLC, Scale for the Assessment of Thought, Language and Communication.
Factor analysis
The dimensionality of the 18 items of the TLC was analysed using principal component analysis with varimax rotation. Seven factors had an eigenvalue greater than 1, but after rotation only four of them were interpretable and sufficiently consistent (data available on request); moreover, inspection of the scree plot (Figure 1) indicated that eigenvalues started to level off for factors after the third or fourth. Because no underlying assumptions had been made about the number of factors, both a three- and a four-factor solution were rotated, yielding the structures presented in Tables 3 and 4, respectively.
Scree plot of Scale for the Assessment of Thought, Language and Communication factor eigenvalues.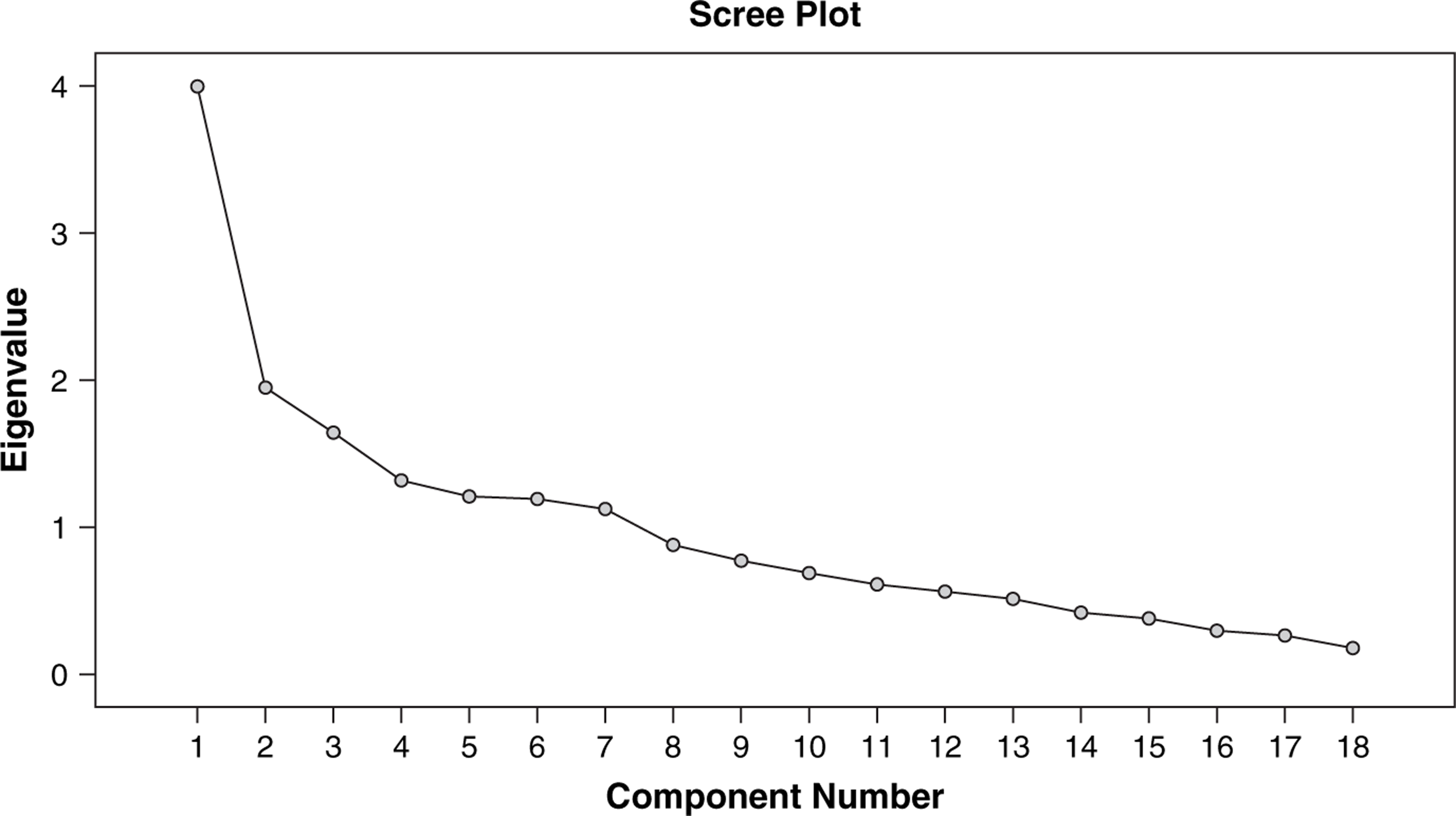
Three-factor solution for the TLC and internal consistency of factors
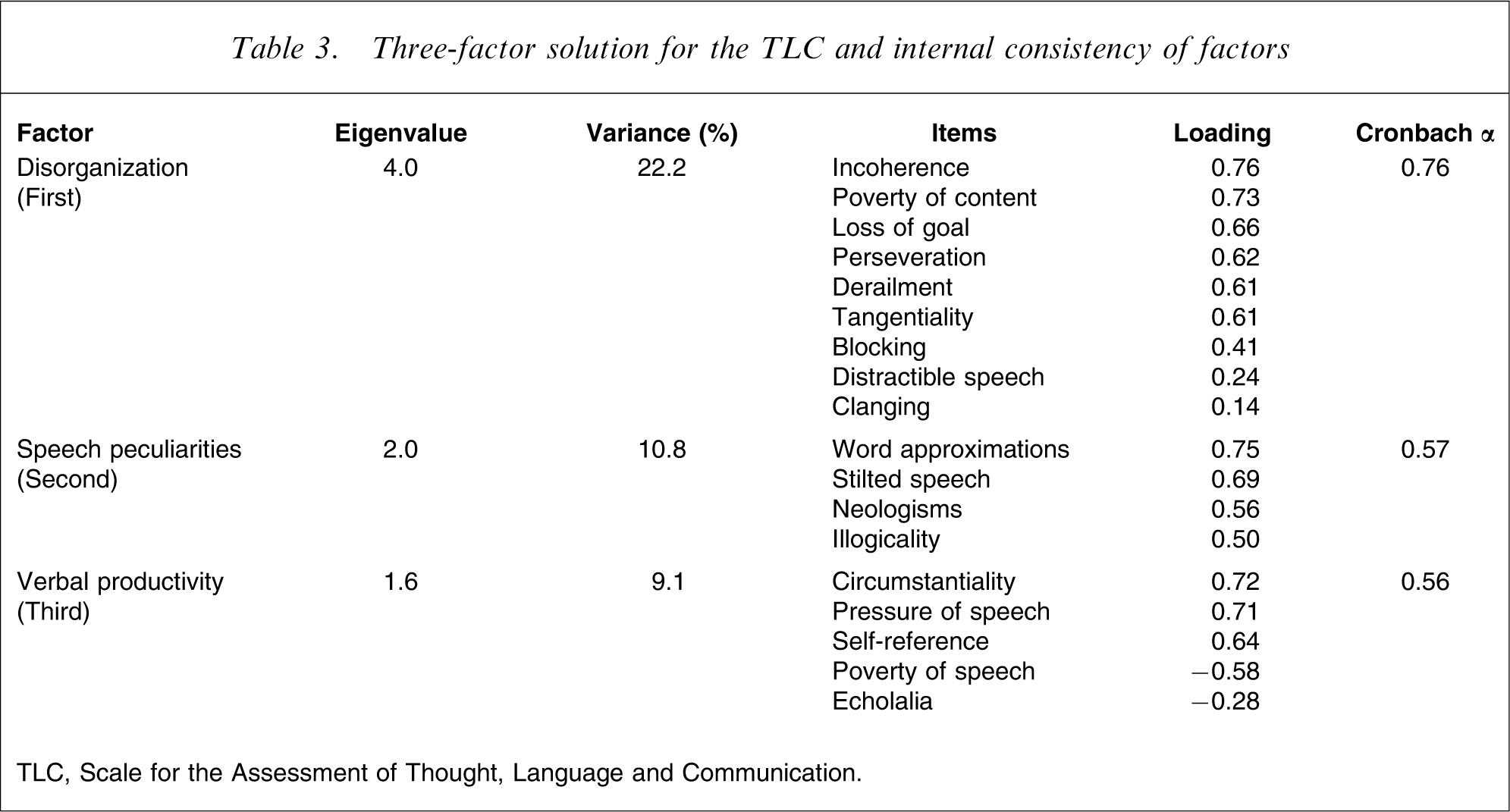
TLC, Scale for the Assessment of Thought, Language and Communication.
Four-factor solution for the TLC and internal consistency of factors
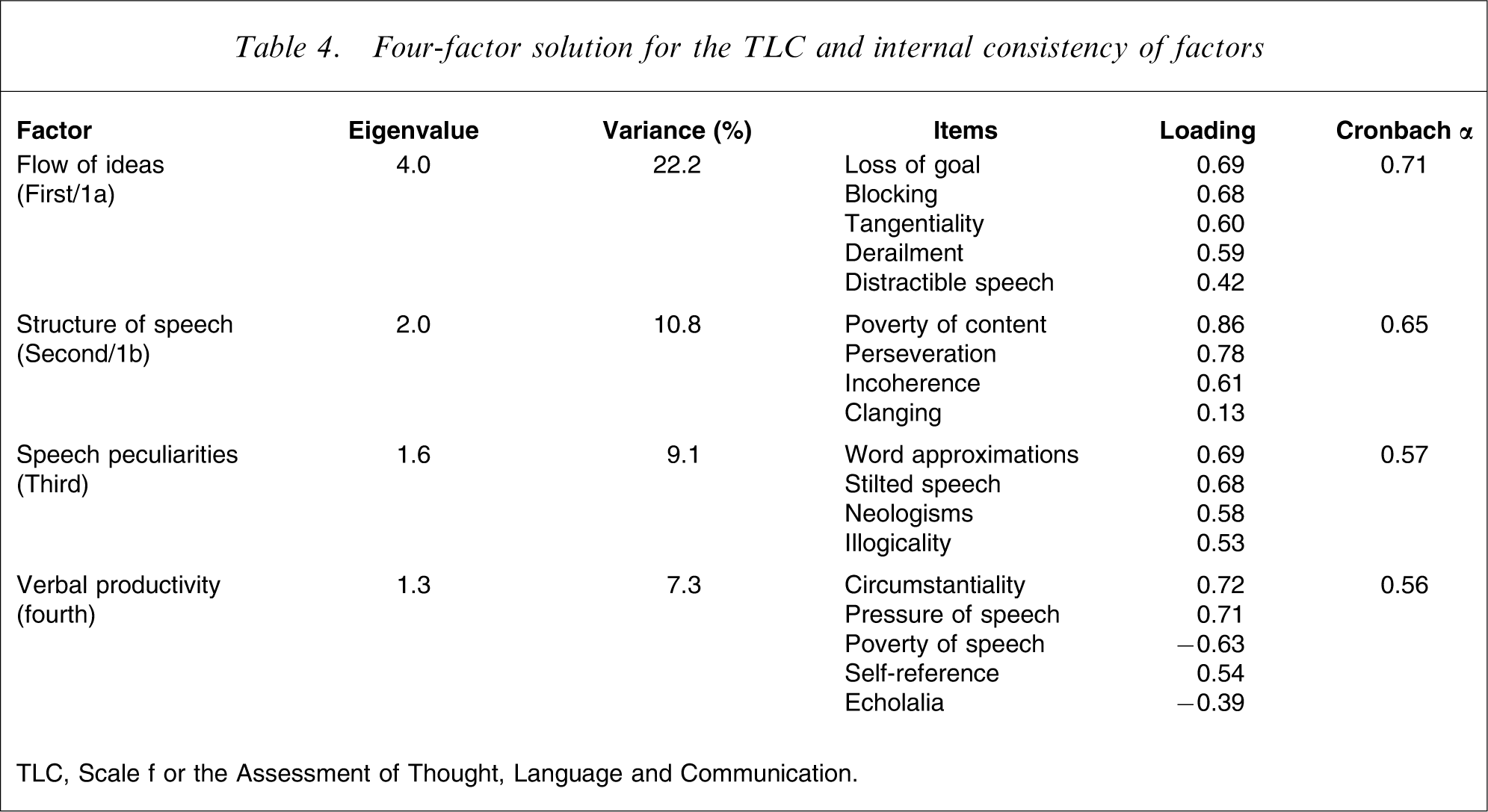
TLC, Scale f or the Assessment of Thought, Language and Communication.
The two solutions are very similar; in fact, the only difference is that the same nine items constitute a single factor in the former, while they are distributed between two factors in the latter. These items comprise derailment, tangentiality, loss of goal, distractible speech, blocking, incoherence, poverty of content, perseveration, and clanging, and could thus be considered to reflect the characteristic disorganization of psychotic speech; in the four-factor solution this factor is further split into two factors, reflecting disturbances in the flow (factor 1a) of ideas and in the structure (factor 1b) of speech. The remaining two factors consisted of the same items in both solutions: one factor comprised neologisms, word approximations, stilted speech and illogicality, and possibly reflected an idiosyncratic use of language, and another was mostly composed of items relating to verbal productivity. It is noted here that the classifications of clanging and echolalia (under the first and last factor, respectively) could be an artefact because these items exhibited very low loadings and were not especially correlated with any of the other items of the scale (possibly due to their very low prevalence in the present patient sample). The internal consistencies of the factors are presented in Tables 3 and 4.
Hospitalized patients and outpatients
Sex, age, age at onset and length of illness were not significantly correlated with any of the TLC factors. The only significant correlation obtained was a negative one between the structural factor (1b) and education (r = −0.27, p = 0.004). Acutely admitted patients significantly differed from outpatients only in the amount of verbal productivity (factor 4) disorders (t = 2.99, p = 0.004, all other ps > 0.1); inpatients had greater mean scores on this factor (2.4±1.8) than outpatients (1.4±1.2).
Discussion
The frequency and severity of most TLC items in the present study were generally in the range of previously reported values, although comparisons are complicated by the large variation among studies (Table 1), possibly due to differences in diagnostic criteria and sample composition [7], [8]. The only consistent difference in the present study in comparison to other studies was the decreased frequency and severity of the derailment and loss of goal items. This finding could be attributed to the fact that a significant proportion of patients included in the present study were stable outpatients. But it could also reflect the substantial overrepresentation of the paranoid subtype of schizophrenia in the present study. Unfortunately, data regarding differences in thought disorder patterns among diagnostic subtypes are scarce: although earlier studies have looked separately into thought disorder profiles of different subtypes of schizophrenia [6], [21], in these studies emphasis is usually placed on the (more prominent) differences between schizophrenia and other disorders; moreover, study differences in diagnostic criteria and subtype categorizations preclude the drawing of any secure conclusions in relation to the present study. Nevertheless, some thought disorder symptoms have been reported to be differentially affected by specific subtypes of schizophrenia [21]; furthermore, because specific speech disorders (such as disorganized speech or echolalia), or absence thereof, are included in the diagnostic criteria for schizophrenia subtypes according to DSM-IV [2], it is reasonable to assume that the frequency and severity of some TLC items might have been affected by the analogy of the various subtypes in the patient sample.
Factor analysis of the scale yielded a three- to four-factor structure. The first factor corresponded to what Bleuler referred to as ‘loss of associations’ [1], and is found in almost all studies assessing the dimensionality of the TLC with only minor variations. This factor could be further divided into two dimensions reflecting disturbances in the flow of ideas and in the structure of speech; this distinction seems to have some validity because only the latter is negatively correlated with education. Two more factors were also extracted; one that consisted of items reflecting peculiarities of speech, and another that consisted of items relating to verbosity. Thus, the present results have many similarities to those of the Bazin et al. (2002) study [7], the only other study that included both inpatients and outpatients, and to those obtained by Andreasen and Grove (1986) [6], who assessed a mixed sample of manic, schizoaffective and schizophrenic patients. In contrast, the present findings do not support the separate existence of a ‘negative’ dimension in the TLC, as studies of acutely ill patients with schizophrenia have proposed [8], [14]. Moreover, although previous studies have found five or more factors underlying the structure of the TLC [7], [8], [14], all of these studies report at least one factor with low internal consistency and/or consisting of one single item; thus, the assumption of a simpler, three-dimensional, structure is probably more reasonable for practical purposes.
Interestingly, acutely hospitalized patients significantly differed from outpatients only in the dimension of verbal productivity. This could suggest that changes in the amount of produced speech are a more sensitive marker of clinical state than disorganization or speech peculiarities, which represent more stable features of psychotic disorders; further studies are warranted to confirm this finding.
Certain methodological limitations of the present study need to be addressed. First, the patient sample was dominated by patients with schizophrenia. Because it has been shown that patients with schizophrenia might differ from those with non-schizophrenic psychotic disorders, such as schizoaffective and schizophreniform disorders, with respect to the profile [6], [21], [22] and course [6], [23] of thought disorder, it is conceivable that the specific sample composition may have affected the frequency and severity of specific TLC items in the present study. In contrast, this does not necessarily affect interrelations between items and the factorial structure of the scale; in fact, the factor structure obtained in the present study is very close to the dimensions of thought disorder described by previous studies that have included more balanced (in terms of composition) mixed samples of patients [6], [21]. Another limitation of the present study may be that most patients were receiving antipsychotic treatment. Medication (at least neuroleptic medication) has been shown to improve some, but not all, aspects of thought disorder [24], [25], and thus may have affected the findings. Unfortunately, the number of patients in each drug status group (medicated, unmedicated) was too small to permit separate analyses within each group; further research is warranted in order to evaluate the effects of antipsychotic medication on the various TLC dimensions.
Conclusions
The investigation of the factorial structure of the TLC in a mixed sample of inpatients and outpatients with psychotic disorders found no support for the positive-versus-negative distinction of thought, language and communication disorders. Three factors (disorganization, speech peculiarities, and verbal productivity) were found to underlie the variance of the scale, although some evidence indicated that the disorganization factor could be further divided into disturbances in the flow of thought and in the structure of speech. Acutely ill inpatients scored higher than outpatients only in the verbal productivity subscale, raising the possibility that the other two dimensions of the scale, disorganization and speech peculiarities, are stable, long-term features of psychotic disorders.