
Abstract
The unruly heterogeneity of psychopathology within the clinical diagnoses of psychoses, especially schizophrenia, has driven the continuing search for alternative clinical descriptions of these conditions. Some researchers and clinicians have returned to the symptoms and signs which are building blocks of psychotic syndromes and from these have constructed different diagnostic schemata using a fundamentally different approach for characterising psychoses.
To date, atomising diagnoses into numerous diagnostic subclasses has not been successful because the symptoms and signs are too unstable over time. The recent epoch has favoured factor analytic approaches, looking for the dimensions of disturbed psychological function. Crow [1] and Andreasen and Olsen [2] described two factors, positive and negative symptoms, in patients with a diagnosis of schizophrenia. Liddle [3] later showed that three factors: positive, negative and disorganised better fitted the data. These factors or ‘domains of psychopathology’ have also been demonstrated in psychotic diagnoses other than schizophrenia [4] indicating that disturbances in particular domains are not peculiar to particular diagnostic categories. This strengthened the claim that measuring domains of psychopathology can characterise psychosis more accurately than does classifying into diagnoses and can take us closer to the mental states and processes disturbed in psychotic disorders [5].
However, while a number of studies have confirmed positive, negative and disorganised psycho-pathological factors [5], other studies have found different factorial structures [6–10]. These alternative factorial structures undermine the claim that three factors represent the natural underlying structure of the psychopathology. There are several reasons that factor structures will differ between studies. The factors that researchers find will vary with the selection of subjects, with the implicit structure of the instruments and with choices made in analysis. When hospitalised patients are selected as subjects, they are selected not only by illness but also by disability or social behaviour. Second, many interview instruments have embedded factorial structures. Schedules such as the Scales for Assessment of Positive and Negative Symptoms (SAPS [11] and SANS [12]), which are popular in these studies, have been designed with an explicit factorial structure. As different instruments explore psychopathology differently, it is likely that the nature and content of the domains will change [4]. Third, choices always obtrude in statistical analysis. The number of factors extracted from the analysis is chosen by the researcher whose choice may, tautologically, confirm pre-existing ideas. Despite these weaknesses, studies of factors or ‘domains of psychopathology’ persist in psychosis research, probably because of dissatisfaction with the heterogeneity and incoherence of higher level diagnostic classification. For example, it is theoretically possible for two patients with DSM-III-R schizophrenia not to share a single cardinal symptom, or for six dissimilar patients to share an ICD-10 diagnosis of schizophrenia.
An alternative to diagnostic classification is to reach behind the diagnostic categories toward their constituent symptoms and signs. These symptoms and signs can be built into scales of ‘domains of psychological function’. The measures may better fit or predict those features or outcomes that, traditionally, have been used to validate diagnosis. Domains of psychopathology may better explain variance in family history, illness course and treatment response than do categorical diagnoses [9,10,13]. In a study of 706 patients with chronic psychosis, van Os et al. [14] found that factorial scores on psychopathology scales predicted clinical measures better than did diagnosis. That is, the higher the summed score across the factors, the greater the defect or disability. They concluded that much more clinically relevant information came from a dimensional representation of psychopathology than from diagnostic categories which are limited both by their heterogeneity and their mutual exclusiveness [14]. Hence the ‘domains of psychopathology’ approach resolves some of the ‘comorbidity’ contradictions raised by the categorical approach. Categorical diagnoses require ‘comorbid’ diagnoses to explain symptoms which fit other categorical diagnoses [15]. (For instance, depressive symptoms in schizophrenia require a diagnosis of comorbid depression.) This complicates teaching, communication, research and treatment, which are the very justifications for categorical diagnosis.
The Australian National Survey of Mental Health and Wellbeing offered an opportunity to examine the factorial structure in the psychopathology of psychosis without some of the constraints of past studies. A study of people with psychotic illnesses [16] was conducted at the same time as a large community survey of mental health. The sample in the psychotic illnesses study included people in contact with specialist services as well as those in the community not receiving services, and was examined with an instrument (the Schedule for Clinical Assessment in Neuropsychiatry or SCAN [17] items used in the Operational Criteria for Psychosis, or OPCRIT, [18] system) which was designed without explicit factorial structure.
Method
Procedure and subjects
Detail of study procedure and subjects have been described in previous publications [16,19]. Briefly, in four geographically delimited areas (parts of Brisbane, Melbourne and Perth as well as all of the Australian Capital Territory), a 1-month screening census was made of all people aged between 18 and 65 years contacting clinical services and social agencies which might serve people suffering from major psychiatric illness. These included inpatient and outpatient mental health services, private psychiatrists, general practitioners, social welfare agencies and accommodation services for the homeless. A Psychosis Screen of six questions (including a question about known diagnosis) was asked of potential subjects or an informant. Random samples were drawn from the 3493 people which the Psychosis Screen had identified as having a probable psychotic illness. Subjects were approached to consent to interview with a comprehensive diagnostic interview, the Diagnostic Interview for Psychosis (DIP). Interviews were conducted by research assistants with mental health background (most were psychiatric nurses) who had been trained by SCAN-trained psychiatrists at each centre and at intercentre workshops where their ratings were calibrated and interrater reliability found satisfactory [16,19].
From 2002 attempted contacts, 480 refused interview and a further 542 could not be traced or were too unwell for interview. Nine hundred and eighty subjects completed the DIP of whom 978 responded with sufficient data for analysis. Table 1 shows some characteristics of the sample.
Characteristics of sample
Sampling for interview was random within each centre, however, inpatients were overrepresented and outpatients underrepresented in the interviewed sample, due to refusals, unsuccessful attempts to contact, unfitness for interview, or other reasons. The non-interviewed subjects did not differ significantly from the interviewed sample by age or sex, but we cannot exclude differences in symptom patterns associated with their psychotic illness. The over-representation of inpatients weights the interviewed sample towards the more severely ill which needs to be taken into account in interpreting the results.
Instruments
The DIP is a composite instrument composed of established international instruments. It included the complete OPCRIT [18], a diagnostic instrument of established reliability [20] and performance [21] which is designed to detect all items required for diagnosis according to a number of different diagnostic systems. The present factor analysis study used the SCAN [17] questions and probes relevant to OPCRIT items, selecting only those pertinent to symptoms and signs experienced at the time of interview or in the preceding month. Diagnoses, where used, came from the OPCRIT diagnostic system which makes diagnoses by its proprietary algorithms using the OPCRIT questionnaire data.
Analysis
A principal factor analysis was carried out with NOVAX computer program [22] on a tetrachoric correlation matrix of 64 items from the OPCRIT which represented current symptoms and signs of psychosis present at the time of interview or in the previous month. Four interviewer ratings of the nature of delusional experience refer to delusions at any time. The factors were Varimax rotated.
Factor-based rating scales were constructed by summing the responses of items whose factor loadings were greater than 0.4 on any factor. The sum was divided by the number of items so that each scale lay between 0 and 1.
Results
After inspection of the scree plot (Fig. 1) three, four, five, six and seven-factor solutions were examined. These explained 42.7%, 50.0%, 55.4%, 58.9% and 62.2% of the variance respectively.
Scree plot of factorial solution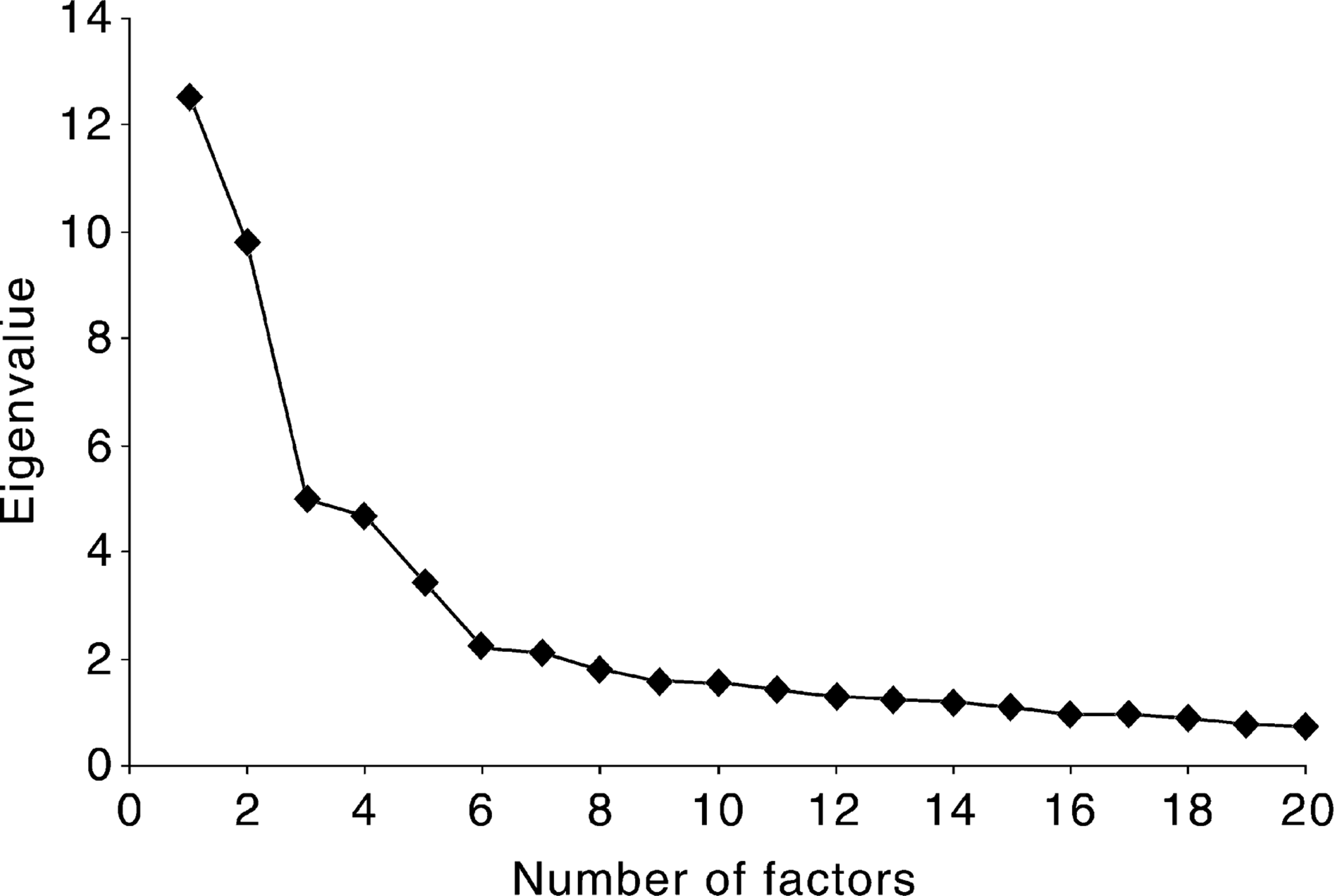
A five-factor solution provided the most satisfactory fit to the data. In the five-factor solution most symptoms loaded on one and only one factor, and only two symptoms were not represented in some factor.
A six-factor solution produced almost identical factors, but added another on which only a single item (increased sociability/disinhibition) had a substantial loading. A seven-factor solution retained the previous structure, but added a further factor with low loadings on a wide range of items which had loaded more strongly on other factors. The seventh factor was unintelligible.
Three- and four-factor solutions combined positive and negative symptoms into a single factor and otherwise created a model which was too condensed to illuminate any psychopathological relationships.
The five factors and their loadings are presented in Table 2. The first factor is substantially loaded with the 19 items which specify dysphoria and depression with subjective anergia and dysphoria as leading symptoms (dysphoria factor).
Factor loadings for five-factor solution for OPCRIT items
The second factor ties clearly the seven positive symptoms of hallucinations, delusions (other than nihilistic and poverty delusions) and abnormalities of thought possession (positive symptoms factor).
The third factor holds all items indicating substance abuse and dependence (substance abuse factor).
The fourth factor holds the primary signs of psycho-motor acceleration and mania, a total of eight items (mania factor). Two items which clinical intuition would bracket with the mania factor, increased sociability/disinhibition and self-esteem, do not load on this or any other factor.
The fifth factor contains 10 items which are classically associated with negative symptoms; incoherence and restricted affect (negative symptom/incoherence factor). However, this factor also loads with both positive and negative formal thought disorder and agitated activity. Positive thought disorder was defined as ‘speech fluent but communicates extremely poorly due to neologisms, bizarre use of words, derailments, loosening of associations’, negative thought disorder was defined as ‘severe blocking, poverty of speech, restricted quantity of speech’, and agitated activity was defined as ‘excessive repetitive activity, fidgety restlessness, hand-wringing, pacing, accompanied by mental anguish’. Six and seven factor solutions did not cleave positive from negative thought disorder or agitation.
Factor-based rating scales
As would be anticipated for scales derived from factor analysis, the five rating scales had satisfactory reliability. Cronbach's alpha for the scales were dysphoria factor, α = 0.91; positive symptoms factor, α = 0.86; substance abuse factor, α = 0.84; mania factor, α = 0.88; negative/incoherence factor, α = 0.62.
Table 3 shows the correlations between factor-based rating scales. There are significant correlations between positive symptoms and substance abuse, mania and negative/incoherence symptoms. There is a positive correlation between mania symptoms and negative/incoherence symptoms. Notably, there is no negative correlation between mania and dysphoria.
Factor scale intercorrelations
The relation of factor-scale scores to categorical diagnosis
Figure 2 shows the mean scale scores across ICD-10 and DSM-III-R diagnoses. Scores are all scaled to fall between 0 and + 1. These show that the activity of psychopathological factors follows an expected pattern with predominant symptoms concurring with the diagnostic category. However, all factors are active in all the diagnostic categories. Notable is the prominence of depressive symptoms throughout, whether or not they are anticipated in the criteria for these diagnoses.
Distribution of scales by ICD-10 (a) and DSM-III-R (b) diagnoses. ─, Dysphoria scale; □, positive symptom scale; ⊡, substance abuse scale; ▒, mania scale; ▪, negative symptom/incoherence scale.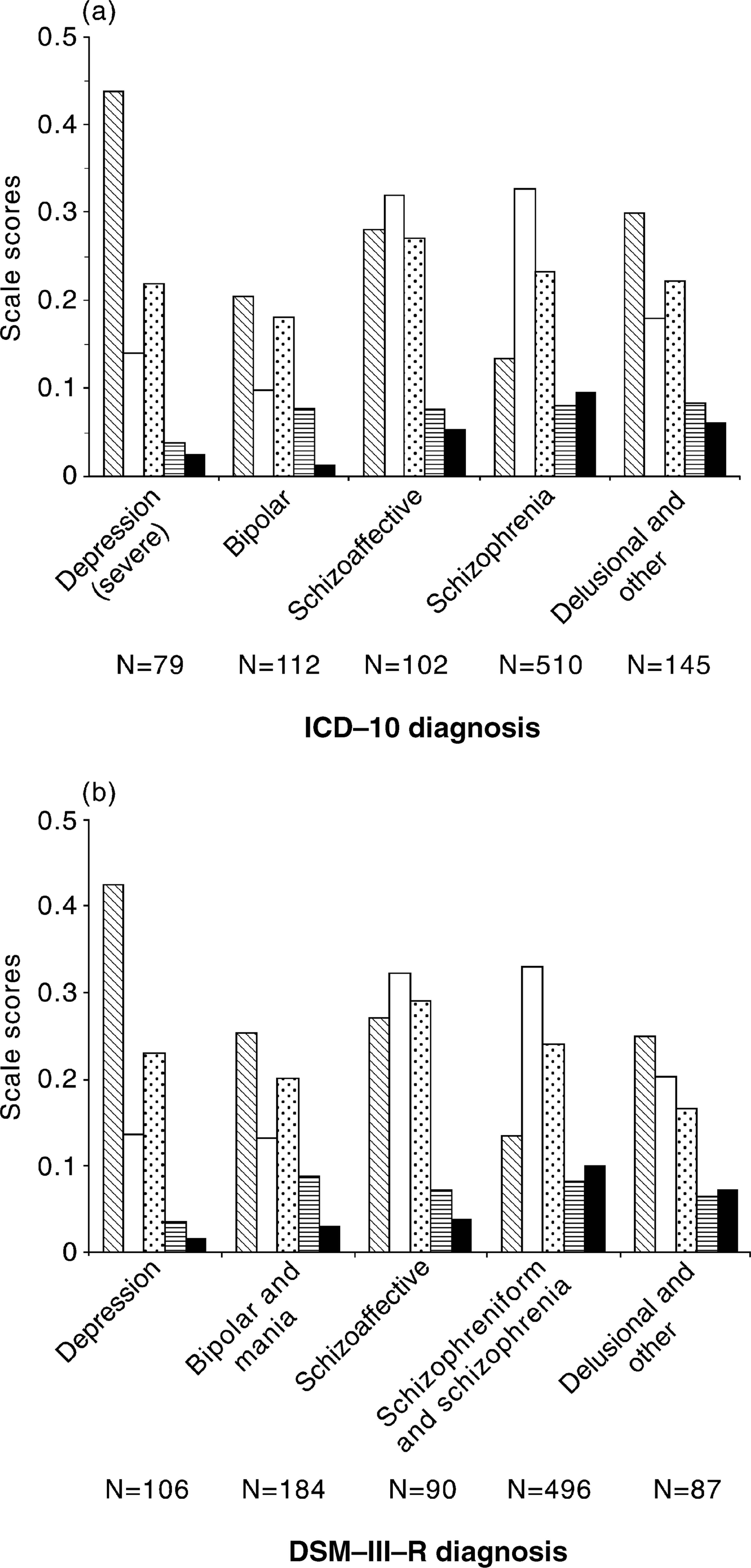
The symptom pattern is very similar between ICD and the DSM diagnoses. Analyses of variance showed that, between diagnoses, scores on depression, positive symptom and negative symptom/incoherence scales were significantly different, but scores on the elevation and negative symptom/incoherence scales were similar. Post-hoc multiple comparisons, using Tamhane's T2 statistic (which does not assume equal variances) [23], indicates that there is no significant difference on the positive symptom and negative symptom/incoherence scales between schizophrenia, schizoaffective and delusional disorders. Schizo-affective and depressive disorders score similarly on the dysphoria scale.
Discussion
This study reports the principal factor analysis of data from the Low Prevalence Disorders Study, part of the Australian National Mental Health Survey. The 978 subjects, who satisfied screen criteria for a psychotic illness, were sampled from a large number of people with psychotic illness detected in a month-long census of services and agencies. The number of subjects and the range of psychotic conditions and settings were larger than is usual for this sort of study.
The principal factor analysis was performed on OPCRIT data extracted from a comprehensive interview instrument composed for the survey. The OPCRIT items used in the analysis related to psycho-pathology present at the time of the interview or reported in the month preceding interview.
Principal factor analysis yielded five principal factors which explained 55% of variance. The five factors, in order of the variance explained, can be characterised as dysphoria (or depression); positive symptoms (hallucinations, delusions and abnormalities of thought possession); substance abuse; mania (psychomotor acceleration); and negative symptoms/incoherence (incoherence, thought disorder, restricted affect).
Rather than supporting the repeatedly confirmed three-factor solution for schizophrenia (positive, negative, disorganised), this factor analysis appears to confirm the factor structure found in other studies which have taken less-highly selected populations or used less committed instruments [7,8,10]. In particular, the findings tend to confirm those of McGorry et al. [8] whose factors included depression and mania, but also ‘Schneiderian’ and ‘Bleulerian’ factors named in homage to the clear psychopathological descriptions provided by these historical figures. Their ‘Schneiderian’ and ‘Bleulerian’ factors appear reasonably congruent with our positive and negative/incoherence factors, respectively. The negative symptom/incoherence factor represents impoverishment and both positive and negative thought disorder, which is more complex than is generally subsumed in ‘negative symptoms’. Moreover, unlike Andreasen et al's findings [5], negative symptoms such as blunted affect do not clearly segregate from positive thought disorder.
We have treated substance abuse equivalently with other symptoms and signs rather than assuming it to be a cause or a comorbidity. Its salience and ubiquity in the sample deserves its importance as a feature of these illnesses without prejudgement of its role.
Importantly, the examination of the derived scale scores showed that symptoms are active across the diagnoses and the presence of even dysphoria did not exclude symptoms of elevation.
Methodological issues
Most of the methodological issues of this study are shared by all such factorial studies. The size of the factors or the variance they explain depends on the number and choice of items devoted to them. The OPCRIT has 19 dysphoria items and nine mania items. Clearly, questions not asked can never yield a factor or factorial loading. Moreover, where an item was a factor of its own, a single-item factor, the relative weight it exerted on the analysis and its prominence in the model was small.
Extracting only five factors reflects the judgement of the investigators. More than 12 factors could have been reported by a common convention which retains all factors with Eigen values exceeding 1.0. However, the scree plot, which indicates how much variation each successive factor explains in the data, confirms the clinical intuition which rejected the solutions with more factors. Not only did the extra factors not make clinical sense, they explained little of the variance and their component items loaded more heavily on factors already identified.
The results of factor analysis are sensitive to the method of extraction. In this study, all item ratings were made binary, that is, present or absent. For these binary data, the tetrachoric correlation matrix was the appropriate object of the factor analysis. Other techniques using continuous variables and bivariate correlations may yield subtly different results.
There were also some characteristics specific to this study. Interviews were conducted by clinicians trained in administration of the instrument, but the diversity of the interviewers' clinical background might increase the variability of item endorsement. Second, the rate of non-response means the sample was skewed to those well enough and willing to be interviewed. Last, course and disability were left out of the analysis, even though some may argue that they must be intrinsic to the description of illness.
However, the study was strong in its large sample size and the breadth of the sample from inpatient, outpatient and community sources in different cities. Selection was by known diagnosis and symptom screening rather than only by prior diagnosis. The study instrument used a large number of items and had no implicit structure.
Implications
Approaching psychological illness by the ‘domains of psychopathology’ or factorial approach provides an alternative to the characterisation by categorical diagnosis which has dominated analysis for more than half a century. The present study shows that the factorial approach can be applied and used to explain a large part of the symptom variance. Is this alternative to categorical diagnosis of any greater use?
Ideally in medicine, categorical diagnoses would be exhaustive (i.e. accommodate all cases), but also mutually exclusive if they are to tie phenomena of illness to a particular underlying disease process [15]. In psychiatry, diagnostic categories have been made exhaustive by multiplying categories, by creating large atypical or residual categories [24] or by loosening category boundaries to accommodate variation. They have been made mutually exclusive by arbitrary exclusion criteria. On the other hand, the ‘domains of psychopathology’ scores are dimensional, flexible and unbounded. These measures allow all patients to be represented on a smaller number of domains in the same way that colour may be characterised by the quantities of a small number of constituent pigments rather than a large number of named colours seen on a colour card.
Change over the course of an episode of illness can be accommodated by revising the balance of the domains without overturning a category. Similarly, domain scores can do away with the need for comorbid diagnoses to represent symptoms that are not core symptoms of the diagnostic category. They may also better adapt to the secular change in the phenomena of illness which has certainly occurred since the existing classifications of illness were described at the beginning of the twentieth century.
Description in terms of domains retains much of the information discarded in categorical diagnosis and this can improve the clinician's grip on or comprehension of the symptoms that bother the patient. This is a counterbalance to categories based on predominant symptoms which promote the notion that the predominant symptom is the pathognomonic symptom or is the only symptom that matters.
Whether the factorial approach actually provides a better guide for practice is a matter for experiment. Symptoms ignored in categorical diagnosis can be shown to prejudice outcomes [25,26]. There is evidence that dimensions of psychopathology are better than categories for predicting disability as well as needs for treatment and service [14]; such predictions are central to health planning. Extensive literature shows that, within a category, information captured by the domain approach explains much of the variability in history, treatment response and outcome [9,13,14,27,28]. The domains of psycho-pathology can be targets for the present enthusiastic biological research in genetics, neurochemistry and functional imaging [29] in the same way that diagnostic categories are currently used. The neuro-imaging of high scorers on negative symptom/ incoherence scales may be more informative than examining the group of ‘schizophrenia’.
Categorical diagnosis is profoundly entrenched in clinical practice and is unlikely to be replaced by dimensional measures of domains of psychopathology, however well domains are substantiated. Historically, medicine has refined descriptive categorical diagnosis until each diagnosis corresponds to a unique underlying pathology or aetiology. This has served medicine well for generations and will not be derailed by its lack of success for the psychotic disorders to this time. Nonetheless, knowledge of alternative dimensional representations of psychopathology may usefully complement our use of categories, enhance awareness of symptoms and ensure that important psychopathology is heeded in practice and research.
Footnotes
Acknowledgements
The present report is based on data collected in the framework of the collaborative Study on Low Prevalence Disorders, an epidemiological and clinical investigation which is part of the National Survey of Mental Health and Wellbeing, Australia 1997–1998. The chief investigators in this study are: A. Jablensky (Project Director, Perth, Western Australia), M. Evans (Canberra, Australian Capital Territory), H. Herrman (Melbourne, Victoria), and J. McGrath (Brisbane, Queensland). A complete list of the investigators is available in Jablensky A. et al. [![]() ]. The study was funded by the Commonwealth Department of Health and Aged Care (Brisbane, Melbourne and Perth) and by local sources (Canberra).
]. The study was funded by the Commonwealth Department of Health and Aged Care (Brisbane, Melbourne and Perth) and by local sources (Canberra).