
Abstract
The purpose of the present paper was to describe the circumstances and phenomenology of patients who remove or pierce their eyes or orbits during psychotic illness. In particular, the aim was to determine if patients in their first-episode psychosis (FEP) carry an increased risk of self-inflicted eye injury when compared to patients with previously treated psychosis (PTP). Data were extracted from all of the case reports published in English since 1960 and from two unpublished Australian cases. More than half of the cases of self-inflicted eye injury that resulted in permanent loss of vision occurred during FEP. Serious self-inflicted eye injuries are rare, but the risk appears to be greatest during FEP. Earlier treatment of emerging psychosis and close attention to patients who attempt to injure their eyes may occasionally prevent blindness.
Vision is our most important sense and the eye is the only external part of the body that has not been ritually mutilated by any recorded culture [1]. Although the eye can be extracted by hand [2], self-enucleation is rare and self-inflicted eye injuries always indicate severe psychological disturbance.
Serious ophthalmic injuries sometimes occur in the course of suicide attempts by shooting or stabbing at the brain [3], [4]. Less serious self-inflicted injuries have been reported in prisoners [5], among the intellectually disabled [6], and in people with disturbed personalities [7]. Self-enucleation is almost always associated with psychotic illness.
Fortunately most cases of self-enucleation involve only one eye, although unilateral enucleation may be complicated by hemianopia in the remaining eye from damage to the optic chiasm and complete blindness may theoretically result from sympathetic ophthalmia. There are also potentially fatal complications of serious eye injuries, including orbital cellulitis, meningitis, subarachnoid haemorrhage and pituitary failure [8].
Kraus et al. summarized 33 case reports of self-enucleation prior to the advent of antipsychotic medication [9]. The first recorded case was an acutely psychotic female inpatient who quoted the gospel of Matthew (chapter 5, verse 29; Box 1) and enucleated both eyes [10]. Half of the historical cases described by Kraus et al. were young women, two-thirds had religious delusions and six were reported to have cited the same biblical passage in the gospel of Matthew.
And if thy right eye offend thee, pluck it out, and cast it from thee: for it is profitable for thee that one of thy members should perish, and not that thy whole body should be cast into hell.
Davidson published the first case report of a patient to receive treatment with antipsychotic medication after self-enucleation [11]. The patient was a young Israeli in first-episode psychosis (FEP) who had delusional beliefs about his eyes. Although the author believed his actions were due to oedipal conflicts, he was treated with chlorpromazine and later had a lobotomy. Many more recent reports still focus on oedipal conflicts, the gospel of Matthew and cultural beliefs such as the ‘evil eye’ as explanations for self-enucleation while only a proportion emphasize the role of acute psychosis.
Several recent studies have reported that nearly half of the homicides during psychotic illness occur prior to initial treatment [12–14], usually in response to frightening symptoms [14]. The hypothesis for the present study was that serious self-inflicted eye injuries may be analogous to homicide in psychosis and hence more likely during FEP. In order to test this hypothesis we examined available case reports of self-inflicted eye injuries to determine what proportion of cases occur before effective treatment
Methods
Search strategies and inclusion criteria
The electronic databases Medline, Embase and PsychLit were searched from 1960 to February 2007 combining the terms psychosis OR schizophrenia OR mental disorder AND self-enucleation OR enucleation OR self-inflicted eye injuries OR eye injuries OR oedipism OR eye trauma. The references of relevant articles were hand searched for further articles. Case reports of self-inflicted eye injuries by patients with psychotic illness published in English were included.
Two reports of patients who had injured their corneas with disinfectant in response to the delusional belief that their eyes were infested and five cases of psychotic patients who enucleated another person's eyes were excluded. Of interest, the patients who injured another person's eyes were reported to have believed that the victim's eyes were a threat to them and three of the five subjects were in FEP [15], [16].
Definitions of prior treatment status and management of missing data points.
Cases were classified as FEP if it was stated that the patients had never received antipsychotic treatment or if they had received less than 1 month of antipsychotic treatment. Patients were classified as having previously treated psychosis (PTP) if prior treatment was described, if they had an established diagnosis of schizophrenia prior to the mutilation or if they were described as having chronic schizophrenia.
Some histories were defined as ‘brief’, generally if they were only of one paragraph in length. Items that were not mentioned in brief reports were omitted (scored as missing data points). In cases described in more that paragraph, items that were not mentioned were regarded as not being present and were scored with a zero and thus appeared in the denominator. The exception to these rules were a small number of items that were actively reported as not being present in brief accounts that were ascribed a zero score and were also included in the denominator. The histories were examined independently by ML and NB.
Statistical analysis
Categorical differences between the FEP and PTP groups were analysed using χ2 tests. Fisher's exact test was used where frequencies were <5 in any cell. The denominator (n) varied for the 2×2 tables because some unreported items were scored as missing data, as described in the previous section. Patient age was analysed using unpaired two-tailed t-test. Statistics were performed using SPSS Release 15.0 (SPSS, Chicago, IL, USA).
Results
We found 87 unique case descriptions of serious self-inflicted eye injury by patients diagnosed as having a psychotic illness in 54 publications [9], [11], [17–68]. Most cases were recent: only two cases were reported in the 1960s, 18 in the 1970s, 20 in the 1980s and 47 since 1990. We included the clinical histories of two unpublished patients who were known to the authors to make a total of 89 cases.
Data quality and inter-rater reliability
Sixty-nine of the 87 published cases were described in some detail and 18 cases were classified as brief reports. The raters disagreed about the classification of two case histories, which were then classified as brief reports.
The clinical diagnoses reported by the treating doctors were used. Few authors provided a DSM or ICD diagnosis. There was no disagreement in the ratings of the diagnoses. In two cases histories the authors disagreed about FEP/PTP status. Both cases were finally classified as having undetermined treatment status by agreement between the raters. There was also disagreement about the total number of cases. Further examination of the place in which the injury was said to have occurred, the demographic details of the patient and the content of the case history indicated that two cases had been separately reported by different authors.
In addition to the diagnosis and treatment status there were 3026 data points considered with respect to the demographics, injuries, patient circumstances and symptoms. Disagreements in 20 further data points were resolved by consensus.
All 89 subjects were ascribed the diagnosis of a psychotic illness. Eighty-two of the 89 subjects were reported to have a symptom of psychotic illness, such as hallucinations or a delusional belief.
Treatment status and injuries
There were 89 available case reports of serious self-inflicted eye injury by patients diagnosed as having a psychotic illness (Tables 1 and 2.). Self-enucleation was more common than penetrating and other orbital injuries. Three patients blinded themselves with air guns and three patients sustained eye injuries in the course of attempting to stab their brains with a pen or pencil.
Reported clinical diagnosis in serious self-inflicted eye injury associated with psychotic illness (n = 89)
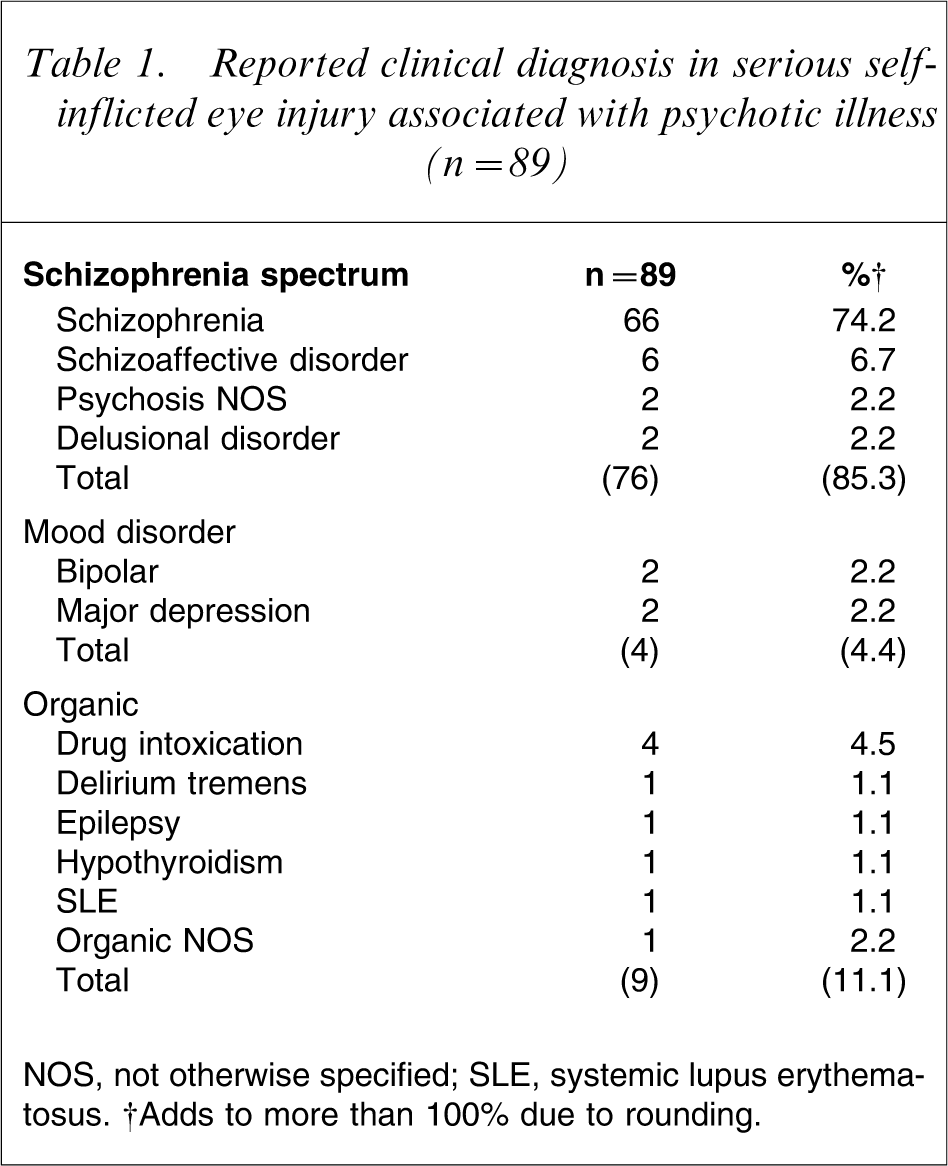
NOS, not otherwise specified; SLE, Systemic lupns erythematosus.
Self-inflicted eye injuries in FEP vs PTP
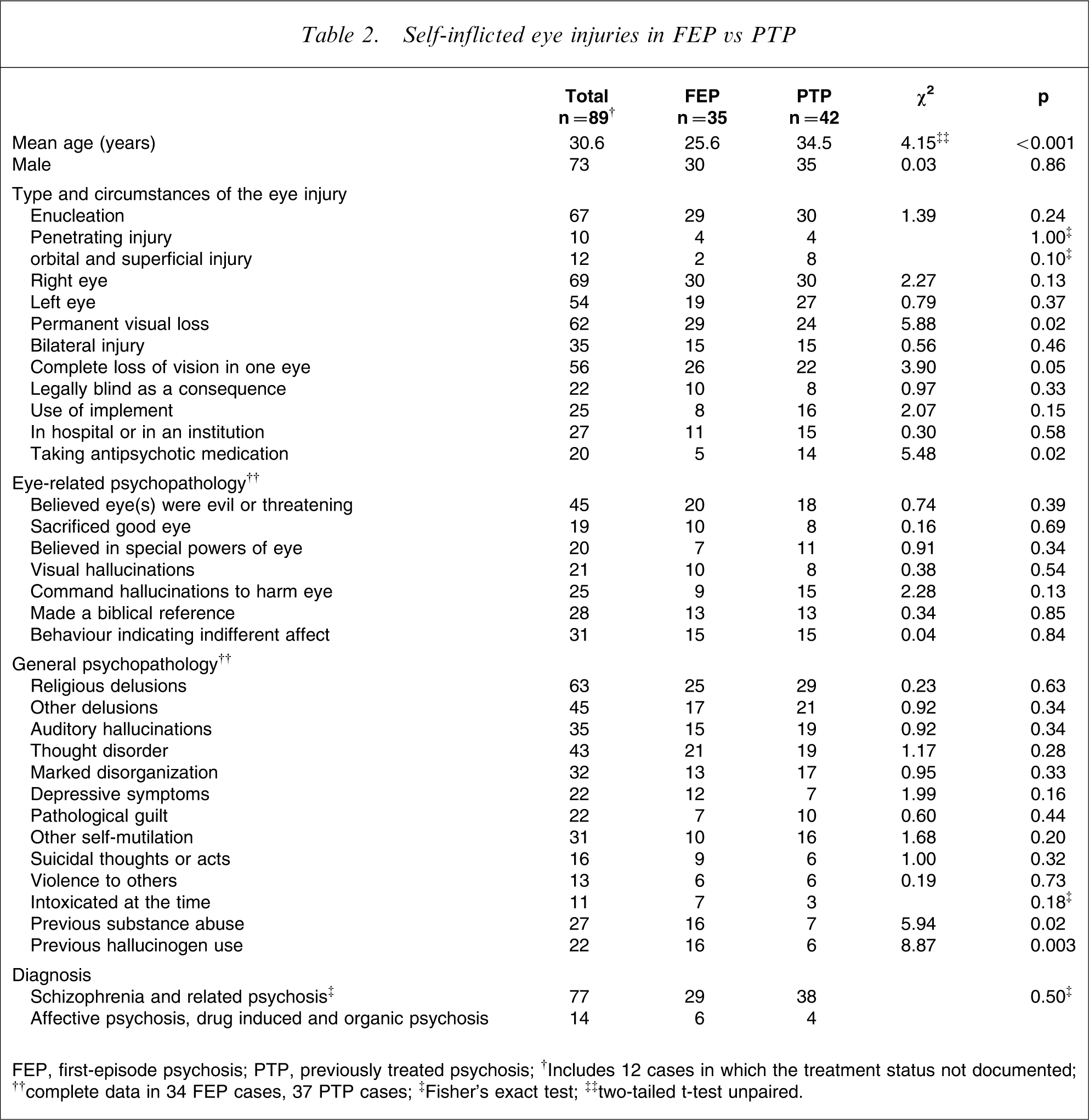
FEP, first-episode psychosis; PTP, previously treated psychosis.; † Includes 12 cases in which the treatment status not documented; †† complete data in 34 FEP cases, 37 PTP cases;‡ Fisher's exact test; ‡‡ two-tailed t-test unpaired.
Treatment status was known in 77 cases and 35 of these patients were in FEP. FEP was associated with more severe injuries involving blindness or the complete loss of an eye (Table 2). Permanent visual loss occurred in 53 of the 77 subjects for whom treatment status was known, of whom 29 (55%) were in FEP. Five of 35 FEP patients had very recently been admitted to a psychiatric hospital for the first time and several patients self-enucleated while being nursed one to one.
Many of the patients in this series attempted or performed other forms of self-mutilation or violence. Four patients stabbed themselves in the thorax or neck, three attempted to amputate their hands, two bit off their tongues, two attempted penile amputation and one castrated himself. Two of the patients had previously committed a homicide and there were several reports of serious assaults. Only one patient was reported to have later committed suicide.
Psychopathology
Psychotic symptoms specifically relating to the eye were reported in 77 of 82 cases (94%) in which any specific psychotic symptom was described. The most common beliefs were that the eye was evil (and a threat) or had special (usually threatening) powers. A smaller number believed that they had to sacrifice a normal eye in order to save themselves or other people, sometimes in response to instructions from hallucinated voices. Twenty-one patients reported visual hallucinations, seven of whom had previously used hallucinogenic drugs. Indifference or a surprising degree of calm was reported after the loss of one or both eyes in 25 cases.
Severe psychotic symptoms that were apparently unrelated to the eye such as agitation, disorganized thinking, hallucinations and other delusions were reported with equal frequency in FEP and PTP groups. Delusions with religious content were reported in 63 patients. None of the patients was reported to have subnormal intelligence and the presence of negative symptoms of schizophrenia was rarely mentioned.
FEP patients were more likely to be described as depressed and were more likely to have used drugs, especially the hallucinogenic drugs lysergic acid diethylamide (LSD) and phencyclidine (PCP).
A schizophrenia-related diagnosis was made in 76/89 cases (85%) and two patients diagnosed as having drug-induced psychosis were reported to have persisting psychotic symptoms, which suggested that the correct diagnosis may have been schizophrenia in those cases as well. There were five cases of organic psychosis and only four cases of affective psychosis (Table 1).
Ophthalmic and neurological complications
Although physical complications of self-enucleation have previously been reported to be rare [38], in four of 30 cases (13%) in which a single eye was enucleated, contralateral hemianopia developed; two patients (2.5% of enucleations) developed a subarachnoid haemorrhage and one patient developed a cerebrospinal fluid leak. There were no cases of orbital infection or meningitis in this series, although meningitis was the presenting complaint of a depressed patient excluded from the present study who attempted suicide by inserting a ballpoint pen into the brain while intoxicated [4]. No patients developed sympathetic ophthalmia. One patient may have experienced an exacerbation of their psychotic symptoms from prophylactic treatment with corticosteroids.
Discussion
In contrast to the findings of previous reviews of self-inflicted eye injuries, we found that most of the serious injuries occurred prior to initial treatment rather than later in the illness, and delusional beliefs about the injured eye were the main reason for the injuries [49]. The study also showed that self-inflicted eye injuries are not restricted to Christians of European background, as stated in a recent review [53], and that psychoanalytic theories are of little assistance in explaining the injuries [11], [44].
After consideration of the methodological limitations of this review, an estimate was made of relative risk of catastrophic self-inflicted eye injuries in FEP and after treatment. Causative factors and management were also considered.
Methodological limitations
There are no population-based studies showing the incidence of serious self-inflicted eye injuries. The authors are aware of five cases of self-inflicted blindness due to psychosis in New South Wales (two in FEP, two in PTP, one unknown) over a period of 15 years suggesting a risk of approximately one case per 20m population per year. This estimate should be viewed with caution because of the small number of known cases and the likelihood that there were other cases.
Not all patients who have self-enucleated will have been the subject of a published case report. Hence this series should be considered to be a semi-random sample of a larger group of psychotic patients who have injured their eyes.
We classified 45% of our sample as FEP (95% confidence interval (CI) = 34–57%). The real degree of uncertainty is greater than the confidence intervals would suggest, because the treatment status of 13% of cases could not be ascertained and there may have been publication and reporting bias regarding previous treatment.
The nature of the injuries in FEP patients were more serious because the proportion of FEP cases among those who had visual loss was 55%.
There may have been a bias against submitting a case report of self-enucleation by a PTP patient if the patient's psychiatrist was not completely surprised by the event. This was examined by comparison of the proportion of FEP patients in single case reports and in small series, on the assumption that the authors of reports of small series would have included all the cases known to them. When the patients with some loss of vision in this series were considered, 61% of the cases that were reported as a single case and 50% of patients reported in small case series were in FEP (χ2=0.32, p = 0.67).
There may have been some errors in the classification of previous treatment status in this retrospective review of case histories, which may have biased the study towards an overestimate of the number of patients in FEP if the authors of some of the reports were unaware of previous treatment. Our assumption that patient with a diagnosis of chronic schizophrenia had received treatment may have created bias in the opposite direction. Some of these patients may have been first-episode patients with a long duration of untreated psychosis.
The 12 subjects with undetermined treatment status were unlikely to have altered the reported proportion of FEP patients because the mean age of this group (31.3 years) was only slightly greater than the whole group (30.4 years) and five of the 12 patients were in their late teens or early 20s. Even when all the cases in which the patient's treatment status was not known were assumed to be PTP, the proportion of cases of self-inflicted eye injuries in FEP was 47%.
A conservative estimate of the proportion of patients in FEP was reached after the exclusion of patients who (i) had not lost an eye; (ii) reported substance use and hence may have self-enucleated as a direct effect of intoxication or withdrawal, or who had another organic diagnosis; and (iii) were reported in single case histories. Of the remaining patients, nine of 22 (43%, 95%CI = 35–50%) were in FEP.
Relative risk of serious eye injuries in FEP
Assuming a null hypothesis that the risk of serious self-inflicted eye injuries is the same in FEP and PTP and that the duration of untreated psychosis (DUP) is on average 1 year and the illness lasts for another 24 years, we would expect to find one FEP case for every 24 PTP cases. After excluding cases that may have been unrepresentative we found that nine of the 23 subjects were FEP, and that 29 of the 53 subjects who sustained visual loss were in FEP.
The estimated ratio of FEP to PTP patients of 1:25 is supported by published studies of the incidence and prevalence of schizophrenia-related disorders. The incidence of new cases of psychotic illness is usually reported to be approximately 20 per 100 000 per annum [69], [70], whereas the prevalence of schizophrenia is approximately 500 per 100 000 population [70]. Thus in any given year there is approximately 25-fold more patients who have previously received treatment than new first-episode patients. Hence if 40% of the patients who self-enucleate are in FEP, the risk of self-enucleation prior to treatment is 20-fold higher than the annual risk after treatment.
The high risk of self-inflicted eye injuries in FEP was not simply due to the smaller proportion of this group of patients receiving antipsychotic treatment. The proportion of chronic patients who are adherent to treatment with antipsychotic medication has been estimated to be 50% [71]. Hence there are many more untreated PTP patients than FEP patients in the community and, based on our previous estimates, at least 12-fold more. This result does not mean that non-adherence by PTP patients is not a risk factor for self-enucleation. In this series 14 of 42 PTP subjects (33%) were reported to be taking medication, suggesting that non-adherence to treatment may confer a small increased risk.
Causative factors
Self-enucleation and self-inflicted eye injuries are not limited to Christians of European origin, as recently asserted by Shiwach [53], because published case histories of Japanese patients [59], [72–74] and Chinese patients [19], [39], as well as patients of Jewish [44] and Muslim [17], [68] faith were found. Although some authors seem to suggest that biblical knowledge is a causative factor, a literal interpretation of the Gospel of Matthew may actually have prevented blindness, because the Bible refers to the benefits of removing only the right eye. Patients who quoted the gospel of Matthew were less likely to damage their left eye (Fisher's exact test, p < 0.0001), both eyes (Fisher's exact test, p < 0.01) or experience blindness (Fisher's exact test, p < 0.012).
Although a significant proportion of the authors of the case reports referred to oedipal theory in their discussion, the effects of symptoms arising from the patient's psychosis was a more obvious and straightforward explanation in all of the cases. None of the patients was reported to have self-enucleated for reasons that could be reasonably compared to the story of Oedipus. Nor did any patient report experiences consistent with the usual oedipal explanation for self-enucleation in which feelings of guilt or desire are attributed to the testes and then ‘upwardly projected’ from the testicles to the eyes [56], [75], [76]. In fact, 11 enucleating patients were women and only 21 patients were reported to have pathological guilt, not all of which was sexual in nature. Some authors discounted the role of psychosis with the argument that most schizophrenia patients did not injure themselves, but did not apply the same reasoning when considering psychodynamic explanations.
Cultural beliefs regarding the ‘evil eye’, abnormal religious experiences and concepts of good and evil were also frequently mentioned in the discussions of individual cases, although in only a very small number of cases was it reported that self-enucleation was performed in order to prevent adverse consequences arising from looking at other people. In these cases it was clearly due to symptoms of psychotic illness rather than a cultural belief that a person could be cursed with a glance. In most instances the evil stemming from the eye was perceived as a direct threat to the patient. The common factor in all of the cases of self-inflicted eye injury, irrespective of treatment status, was the presence of severe psychotic symptoms, especially delusional beliefs involving the eye.
Substance abuse appeared to have a causative role in a small number of cases. There were four cases in which there appeared to be a close relationship between hallucinogen or amphetamine intoxication and self-enucleation. In two of these cases the patients remained psychotic for some time after the injury, suggesting that the correct diagnosis was schizophrenia and that the role of substance abuse was probably to precipitate or exacerbate underlying psychosis. Drugs that induce visual hallucinations may predispose the user to later delusions about the eye because, visual hallucinations at the time of the enucleation were only slightly more common in hallucinogen users, and most of the self-enucleations by those who had used hallucinogens occurred months or years afterwards.
The presence of five subjects with a diagnosis of an organic psychosis, a further five patients who attacked the eyes of other people in response to threatening delusions about the victim's eyes, and a patient who enucleated his already blind eye support the conclusion that the main reason for self-inflicted eye injury is the effect of psychosis.
In almost all of the case reports the most simple and logical cause for the catastrophic self-injury was the bizarre belief that there was a threat that could be reduced by removing one or both eyes. In this respect the phenomenology of severe self-mutilation is similar to that of serious assault committed during acute psychosis, which is often performed in response to a delusional belief in the existence of threat [77]. This is also consistent with Favazza's conclusion that self-mutilation is a purposeful, if norbid, act of self-help [78].
Delusions of a religious nature were reported in the majority of these patients, indicating that religious delusions may add to the risk of self-mutilation, although of course only a tiny minority of patients with religious delusions go on to self-enucleate. It is possible that eye-related delusions may be more common in FEP, but no published studies were found that mentioned the incidence of eye-related delusions before and after treatment of psychotic illness.
Management
Completed or attempted self-enucleation is a medical and a psychiatric emergency. An urgent consultation with an ophthalmic surgeon should always be sought, even if there is minimal bleeding, because the extent of the injury may not always be apparent. Prophylactic antibiotics are generally indicated to prevent orbital infection and corticosteroids may be needed to prevent sympathetic ophthalmia after injuries in which the orbit is contaminated with intraocular contents. Intracerebral bleeding, cerebrospinal fluid leakage and pituitary failure should also be considered. Patients with a unilateral injury need to be assessed for contralateral visual loss. The patient's capacity to consent to corneal donation may also be relevant.
Urgent psychiatric care is also required. It should be assumed that any patient who attempts or completes enucleation is acutely psychotic, even if they appear calm. In the case of unilateral or incomplete self-enucleation the risk of further eye injury remains high. Some patients make determined efforts to enucleate that may be prevented only by physical restraint, close supervision or even electroconvulsive therapy (ECT) [36]. The case reports show that one-to-one nursing has not been sufficient to prevent threatened enucleation. Although we hesitate to recommend limb and finger restraint for any patient, in the situation of attempted enucleation the only way to prevent blindness may be to bind fingerless mittens to the patient's hands and restrain their arms to their sides or to the bed until treatment has had time to take effect. Although the use of ECT has been reported only in a small number of cases, in this situation it may be considered to be a safer and less restrictive form of treatment.
Antipsychotic medication is always indicated even if psychotic symptoms are not immediately elicited. Moreover, a longer period of treatment in hospital may also be indicated to ensure that the patient has had as full a remission as possible and has developed some awareness of the presence of illness and the need for continued treatment.
Communication within the treating team is important and any signs of eye gouging should be reported promptly. After a catastrophic event the reactions of staff to psychotic patients who have blinded themselves may influence the patient's subsequent care. Our experience has been that even some professionals assume that enucleation is in some way connected with incestuous feelings, and relatives and friends who read existing publications on the topic may develop similar unfounded beliefs.
Conclusions
The risk of serious ocular self-mutilation is highest in FEP. This finding did not appear to be due to methodological limitations of the study, the lack of treatment at the time of the injury, a particular pattern of symptoms or drug use in this period.
Very rare events such as self-enucleation cannot be reliably predicted. Sometimes it may be possible to reduce the seriousness of some events if clinicians are aware of the danger arising from a failed attempt and the increased risk in patients with delusions about the eye, especially in FEP. Measures to reduce the duration of untreated psychosis may also reduce the incidence of self-enucleation in the same way that they have been shown to reduce suicidal thoughts and behaviour [79].
Footnotes
Acknowledgements
We would like to thank Ilona Harsanyi and Fang Fang of the Winston Library, Sydney Eye Hospital.