
Abstract
In 1982 a poorly managed schizophrenia patient killed six children and injured 38 others in a public housing estate in Hong Kong [1]. Following the subsequent public outcry, a priority follow-up (PFU) system was set up in which psychiatric patients with a history of violence or violent dispositions were registered and closely followed [2]. There are detailed criteria for PFU and subsequent care [3]. Briefly, patients are included in PFU if they have a history of violence or a well-established disposition to violence that requires special attention to their assessment and extra care in management. PFU patients receive additional discharge assessment and are closely monitored by aftercare services. According to the guidelines [3], the status of PFU patients should be reviewed at least annually by a multidisciplinary team. A PFU patient may be changed to non-PFU status if s/he fulfils all of the following criteria: (i) no physical violence for 3 years; (ii) significant improvement in clinical condition; (iii) satisfactory social environment; and (iv) good adherence to treatment [3]. But it should be noted that PFU is not formally legislated and does not equal a community treatment order or any form of compulsory treatment. It is only a reminder for mental health professionals to pay extra attention to potentially dangerous patients.
Experience in Western settings suggests that PFU or similar systems can help to control psychotic symptoms and reduce relapse/re-hospitalization rates and the risk of violence [2], [4–6]. To date, the impact of PFU on patient quality of life (QOL) is unknown although QOL, especially its subjective aspects, has been gaining attention as an important outcome measure in psychiatric practice [7]. Integrating subjective QOL in the traditional outcome measures could give a more complete picture of the effectiveness of mental health care [8].
The aim of the present study was to investigate the impact of the PFU system on QOL in Chinese schizophrenia patients in Hong Kong. We hypothesized that (i) the severity of positive symptoms would significantly correlate with PFU status because most violent acts are the consequence of delusions and hallucinations [9], [10]; and (ii) PFU patients (the PFU group) would have a better QOL than patients without PFU status (non-PFU group) because PFU patients usually receive more intensive mental health care that has proved to be successful in controlling their psychotic symptoms, decreasing relapse and re-hospitalization rates and reducing the risk of violence [4], [5]. All of these factors could lead to a better QOL [11], [12].
Methods
Settings and subjects
The present study was part of a project on QOL in schizophrenia outpatients in China conducted between January 2005 and June 2006 [12]. Subjects were selected by computer-generated random numbers from patients diagnosed with schizophrenia attending the Psychiatric Outpatient Clinic of the Prince of Wales Hospital, which has a catchment population of approximately 800 000.
Patients who met the following inclusion criteria were invited to participate in the study: (i) diagnosis of DSM-IV schizophrenia [13]; (ii) age between 18 and 60 years; (iii) length of illness ≥5 years; and (iv) being an outpatient who had been clinically stable for at least 3 months before recruitment [14]. The exclusion criteria were (i) history of or ongoing major chronic medical or neurological condition(s); and (ii) past or current significant drug/alcohol abuse other than nicotine.
The study protocol was approved by the Joint CUHK-NTEC Clinical Research Ethics Committee in Hong Kong. All participants signed a consent form.
Data collection
Basic sociodemographic and clinical data including PFU status were collected during a diagnostic interview. Psychotic symptoms were measured with the Brief Psychiatric Rating Scale (BPRS) [15]. The following three mean symptom scores of the scale were used: (i) positive (conceptual disorganization, suspiciousness, hallucinatory behavior, and unusual thought content); (ii) negative (emotional withdrawal, motor retardation, blunted affect, and disorientation) [16]; and (iii) anxiety and tension [17]. The 17-item Hamilton Depression Rating Scale (HAMD) [18] was used to assess the severity of depressive symptoms.
Extrapyramidal side-effects (EPS) were evaluated with the Simpson–Angus Scale of Extrapyramidal Symptoms (SAS) [19] and the Barnes Akathisia Rating Scale (BARS) [20]. The sum scores of these scales were entered in the statistical analysis [12].
The Hong Kong version of the World Health Organization Quality of Life Schedule–Brief (WHOQOL-BREF-HK) [21] was used to assess the patients’ subjective, self-reported QOL. WHOQOL-BREF-HK is a generic QOL rating instrument that covers four domains: physical and psychological health, social relationships and environmental factors. Patients assess their satisfaction of each item during the past 2 weeks on a 5-point scale (from 1 = very dissatisfied to 5 = very satisfied).
Doses of antipsychotic drugs were converted to chlorpromazine equivalent milligrams [22].
Statistical analysis
Data were analysed using SPSS version 13.0 (SPSS, Chicago, IL, USA). Comparisons between the PFU and non-PFU groups with regard to sociodemographic and clinical characteristics and QOL were performed using independent samples t-test, Mann–Whitney U-test, χ2 and Fisher's exact tests as appropriate. To control the potential confounding influence of background variables when comparing the QOL between the PFU and non-PFU cohorts, analysis of covariance (ANCOVA) was carried out. Stepwise multiple logistic regressions was used to adjust for relevant covariates and to determine the correlates of PFU status. PFU status was the dependent variable, and the independent variables included age, sex, educational level, marital and employment status, monthly income, length of illness, number of admissions, dose of antipsychotic drugs, history of suicide and violence, positive, negative, depressive and anxiety symptoms, and EPS. The one-sample Kolmogorov–Smirnov test was used to check the normality of distributions for continuous variables. The level of significance was set at 0.05 (two-tailed).
Results
Forty-three of the 310 patients who were approached to take part in the study refused to participate. There was no significant difference between the study subjects and those who refused to participate in terms of age, sex, age at onset, and length of illness.
Table 1 shows the basic sociodemographic and clinical characteristics of the subjects. Twenty-two (8.2%) of the 267 subjects were given PFU status. Table 2 compares the sociodemographic and clinical characteristics, and QOL of the PFU and non-PFU groups.
Subject data (n = 267)
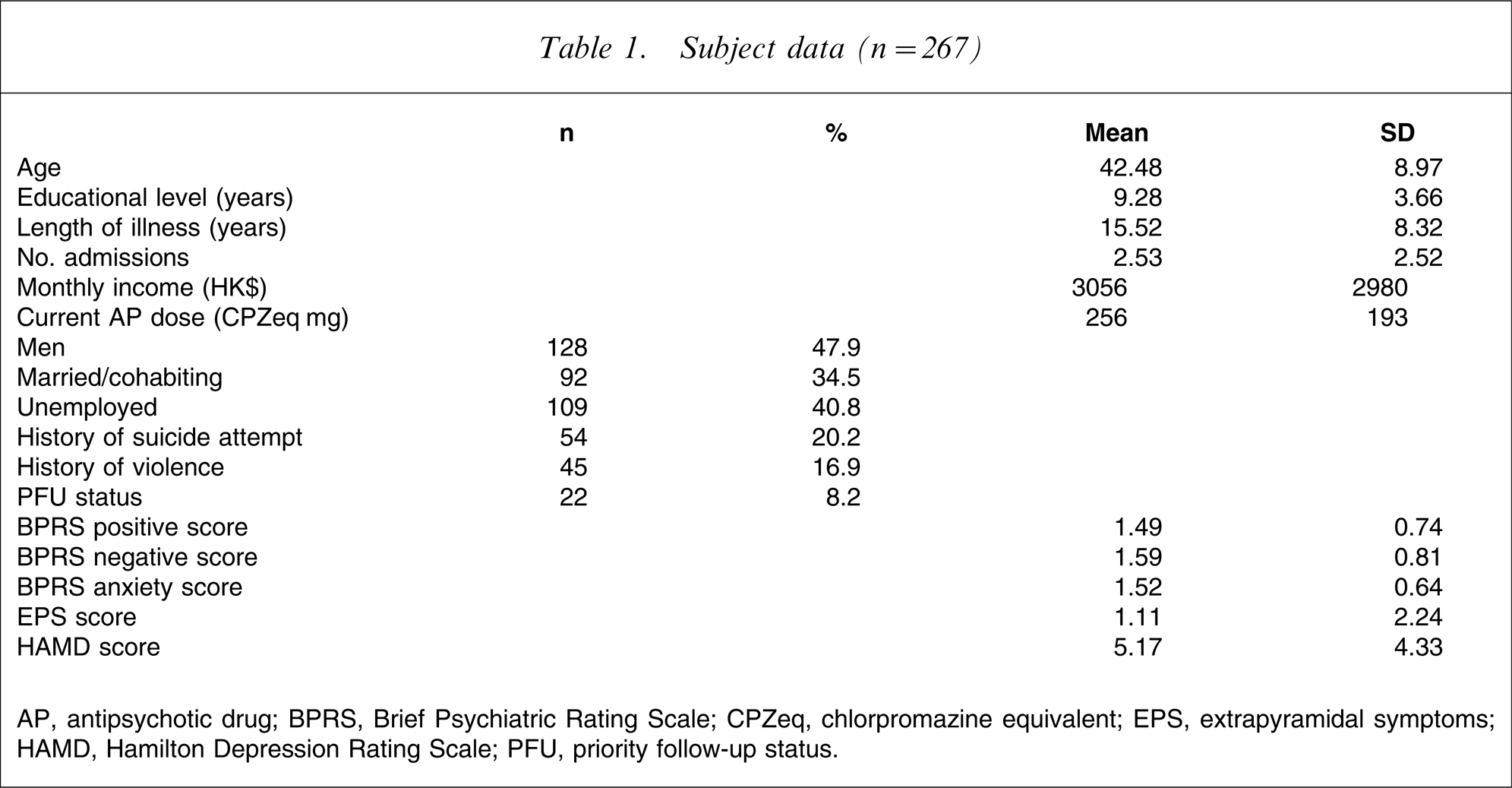
AP, antipsychotic drug; BPRS, Brief Psychiatric Rating Scale; CPZeq, chlorpromazine equivalent; EPS, extrapyramidal symptoms; HAMD, Hamilton Depression Rating Scale; PFU, priority follow-up status.
Subject data according to PFU status
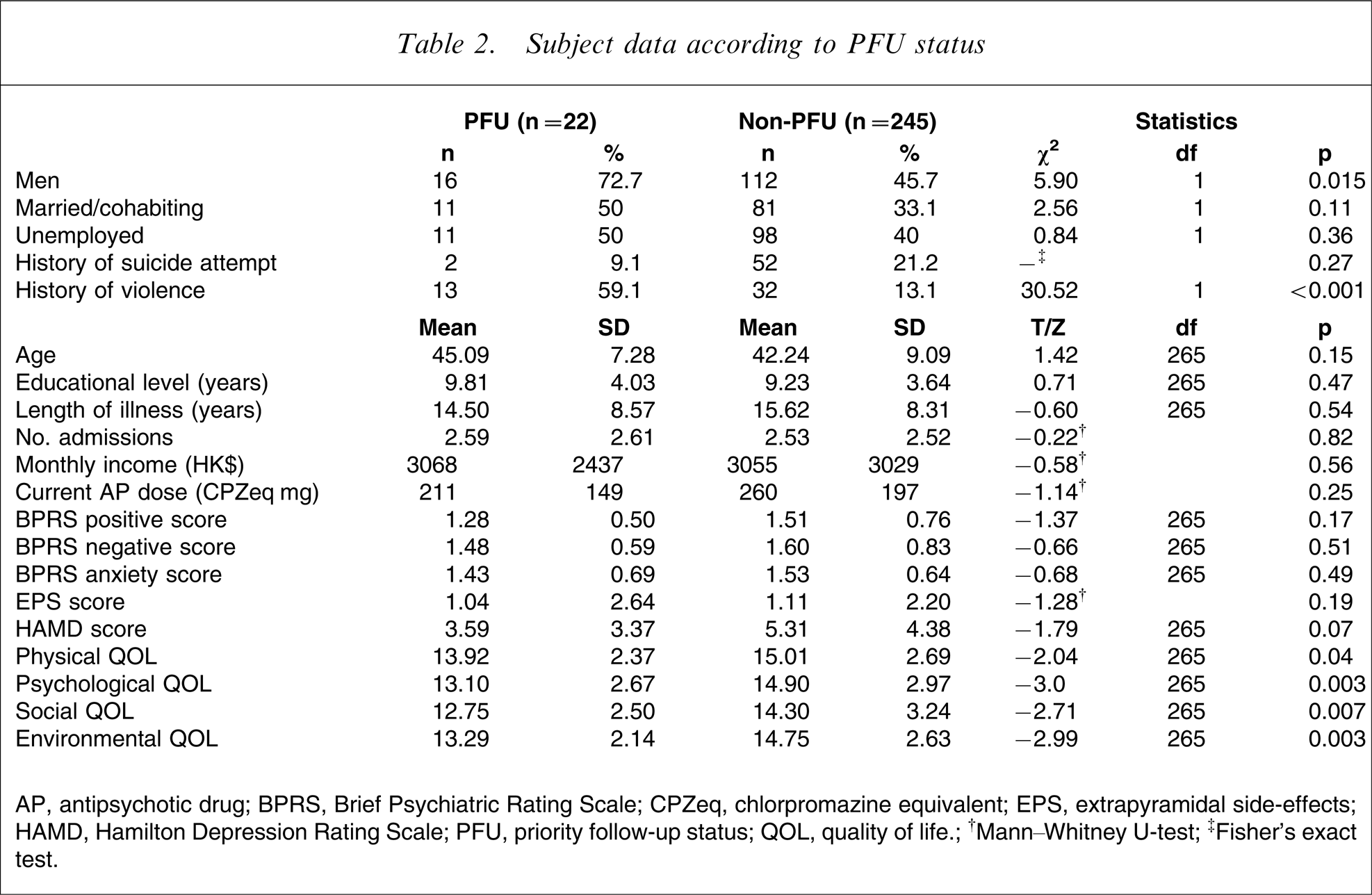
AP, antipsychotic drug; BPRS, Brief Psychiatric Rating Scale; CPZeq, chlorpromazine equivalent; EPS, extrapyramidal side-effects; HAMD, Hamilton Depression Rating Scale; PFU, priority follow-up status; QOL, quality of life.
†Mann–Whitney U-test; ‡Fisher's exact test.
There were significant differences between the two groups in all QOL domains. Having controlled for the effect of sex and history of violence (the variables that significantly differed between the two groups), significant differences remained in the physical (F(1,263)=4.77, p = 0.03), psychological (F(1,263)=7.56, p = 0.006), social (F(1,263)=5.34, p = 0.02), and environmental (F(1,263)=7.27, p = 0.007) QOL domains.
In stepwise multiple logistic regression analysis, only history of violence was significantly associated with PFU status.
Discussion
To the best of our knowledge this was the first study to investigate the impact of a PFU system on QOL in schizophrenia patients.
The first hypothesis that the severity of positive symptoms would significantly correlate with PFU status was not supported. In general, Chinese public opinion is more sensitive to positive symptoms because they are more likely to lead to aggressive or violent behavior [9]. Patients who present with positive symptoms are regarded as threats to social harmony even if they are clinically stable [10], [12]. Therefore the severity of positive symptoms was expected to correlate with PFU status. We assume that because only clinically stable patients were involved in the present study, minor differences between PFU and non-PFU patients with regard to positive symptoms could not be detected using the BPRS.
It has been argued that male schizophrenia patients are more likely to commit violent acts [9], and that position was supported by the present results. In the present study not all PFU patients had a history of violence because patients with proneness to violent acts (e.g. making frequent verbal threats) also receive PFU status [3].
The second hypothesis that PFU patients would have a higher QOL compared to their non-PFU counterparts was also not supported by the results. PFU patients receive more intensive mental health care, which has been be successful in engaging patients, controlling their psychotic symptoms, decreasing relapse and re-hospitalization rates and reducing risk of violence [2], [4–6]. For these reasons, patients with PFU status were expected to have a higher QOL [11], [12], [23]. Contrary to the expectations, however, PFU patients had poorer QOL in comparison with their non-PFU counterparts. Even controlling for the effect of sex and history of violence, significant differences between the PFU and non-PFU groups remained in all QOL domains. We speculate that the discrepancy between the present results and expectations might be partly accounted for by the stigma and related discrimination that have long been fundamental problems in psychiatric rehabilitation [24], [25]. PFU patients are required to regularly attend psychiatric clinics and keep in contact with mental health professionals. Although these measures could control their psychotic symptoms and decrease relapse/re-hospitalization rates, they could not alleviate the public's fear of formerly violent psychiatric patients or reduce discrimination and stigmatization. PFU status could even lead to further social isolation and stereotyping of psychiatric patients [26]. All of these factors would inversely affect QOL [23]. Because of the cross-sectional design, the possible influence of pre-existing factors cannot be ruled out; that is, patients with poor QOL were more likely to be prone to violence and selected for PFU. Longitudinal studies will probably shed light on this issue.
It has been argued that poor QOL in psychiatric patients might arise from their dissatisfaction with their inner experiences of self-fulfilment, self-reliance, harmony, freedom, joy, and love [27]. Current mental health policy and most psychiatric rehabilitative interventions in Hong Kong pay the most attention to effective symptom control, relapse prevention, and improvement of living standards regardless of the patients’ expectations and subjective experiences. The present findings support the need for a paradigm shift [27], [28]: psychiatric treatment and rehabilitation would fail to improve patients QOL if all rehabilitative measures focus on the outer world, that is, only the illness-related aspects and patients’ material well-being, and ignore the patients’ inner world. Patient views should be considered by community mental health services including the PFU system.
The major strength of the present study is the large, randomly selected, ethnically homogenous sample. But the results should be interpreted with several methodological limitations in mind. First, the results are applicable only to community-dwelling, clinically stable schizophrenia outpatients, precluding generalization to patients with different clinical status or those living in residential facilities. Second, the study was cross-sectional, and the causality of relationship between PFU status and its potential predictors could not be explored, thereby warranting prospective studies with a more appropriate control group: patients meeting PFU criteria who receive only standard care. Third, the sample size of the study group was relatively small; only 22 PFU patients were involved, which would have led to inadequate power to make a comparison. Finally, the present findings may reflect only the nature of the service model used in Hong Kong and could not be applied to other types of mental health services in other localities.
Footnotes
Acknowledgements
The authors would like to thank the staff at the Day Hospital at Shatin Hospital and the Li Ka Shing Psychiatric Outpatient Clinic at the Prince of Wales Hospital for their assistance in the project.