
Abstract
Over the past few decades, quality of life (QOL) has been increasingly gaining attention as a valuable outcome measure to evaluate the impact of psychiatric illness on patients’ daily lives following de-institutionalization. QOL is defined as ‘an individual's perception of one's position in life in relation to goals, expectations, standards and concerns in the context of the culture and value systems in which one lives’ [1]. According to this definition, QOL is a wide concept consisting of four domains: physical health, psychological state, social relationships, and relationship to salient features of the environment.
During the past several decades, factors related to QOL in schizophrenia have been extensively reported. Browne et al. found that age, length of illness, and the cumulative duration of hospitalization significantly correlated with QOL [2]. Patterson et al. identified psychotic symptoms as the predominant determinants of QOL [3]. Bechdolf et al. investigated 66 patients with schizophrenia and found that the strongest determinants of QOL were depressive symptoms [4]. A survey that involved 227 inpatients with schizophrenia examined the relationship between QOL and suicide attempts and found that dissatisfaction with QOL was associated with repeated suicide attempts [5]. In addition, multicenter studies indicated that cross-cultural or ethnical differences also exist in schizophrenia with respect to QOL [6, 7]. However, there is still controversy about most factors that are associated with QOL due to differences in participants and settings, sample size, study design, and assessments and instruments.
It is noteworthy that all of the aforementioned studies were conducted in Western countries where the prevailing Judeo-Christian culture places high value on independence and self-realization [8]. In East Asia, particularly in those countries and regions that are influenced by traditional Chinese culture, traditional Confucian ideas still predominate, emphasizing interdependence and group harmony within the family [9]. Therefore, it is unlikely that findings of studies conducted with Caucasian patients would be applicable to a non-Western culture such as that of the Chinese. Behind its Westernized façade, traditional Cantonese cultural factors remain strongly influential in Hong Kong. For example, the traditional culture is well exemplified in public attitudes towards different psychotic symptoms. The general population in Hong Kong is more sensitive to positive symptoms, especially to aggressive or violent behaviour. Psychotic patients with these symptoms are usually more stigmatized and are committed to psychiatric hospitals because they are commonly regarded as threats to the social harmony even if they are clinically stable contrast, psychotic patients with negative symptoms are usually better accepted and supposed to ‘rest at home’ or receive psychological counselling rather than psychiatric care. While there are many publications on QOL in Western countries, few studies have focused on Chinese schizophrenia patients in this area [10].
Subject data (n = 200)
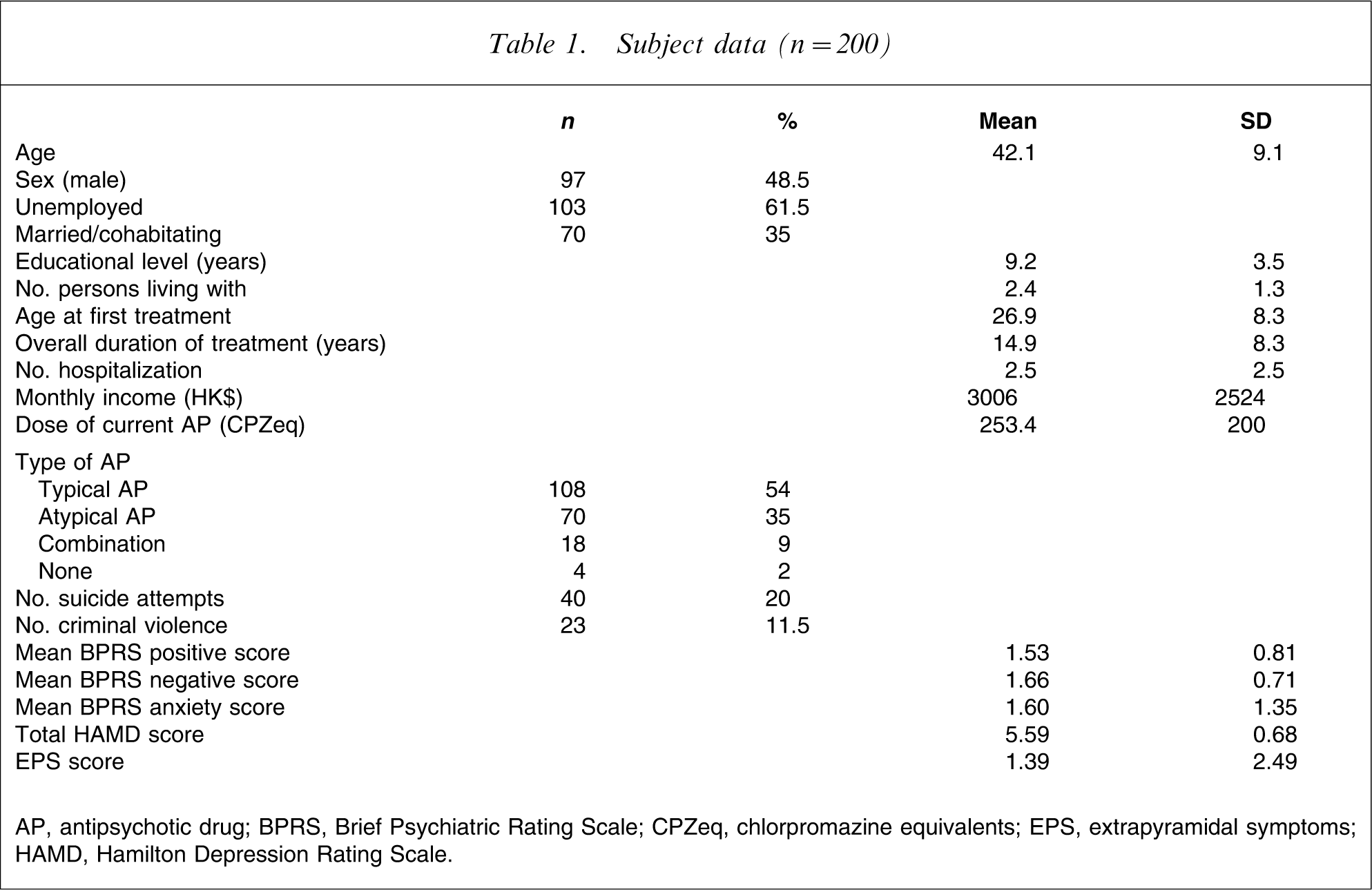
AP, antipsychotic drug; BPRS, Brief Psychiatric Rating Scale; CPZeq, chlorpromazine equivalents; EPS, extrapyramidal symptoms; HAMD, Hamilton Depression Rating Scale.
Comparison of QOL
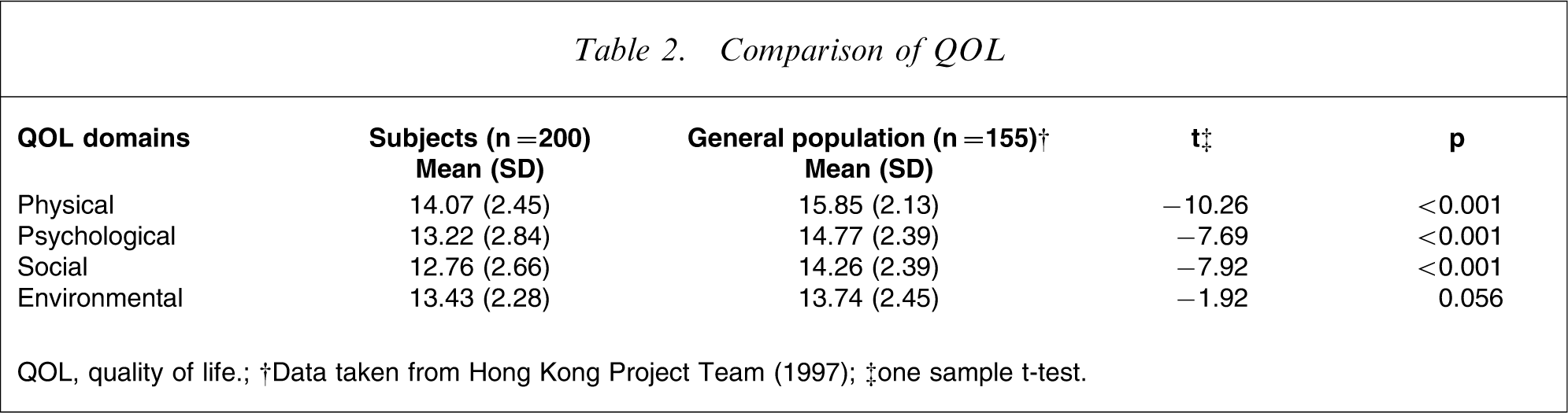
QOL, quality of life.
†Data taken from Hong Kong Project Team (1997); ‡one sample t-test.
The objective of the present study was to examine the association of sociodemographic and clinical characteristics and QOL. In view of the results of earlier studies [10, 11], the first hypothesis was that all aspects of QOL would be significantly lower in patients than in the general population of Hong Kong [12]. The second hypothesis was that one or more of the sociodemographic (e.g. age, sex, and educational level etc.) and clinical factors (e.g. depressive, anxiety, positive and negative symptoms etc.) would significantly correlate with QOL. The third hypothesis was that depressive and psychotic symptoms would significantly predict QOL.
Spearman correlations
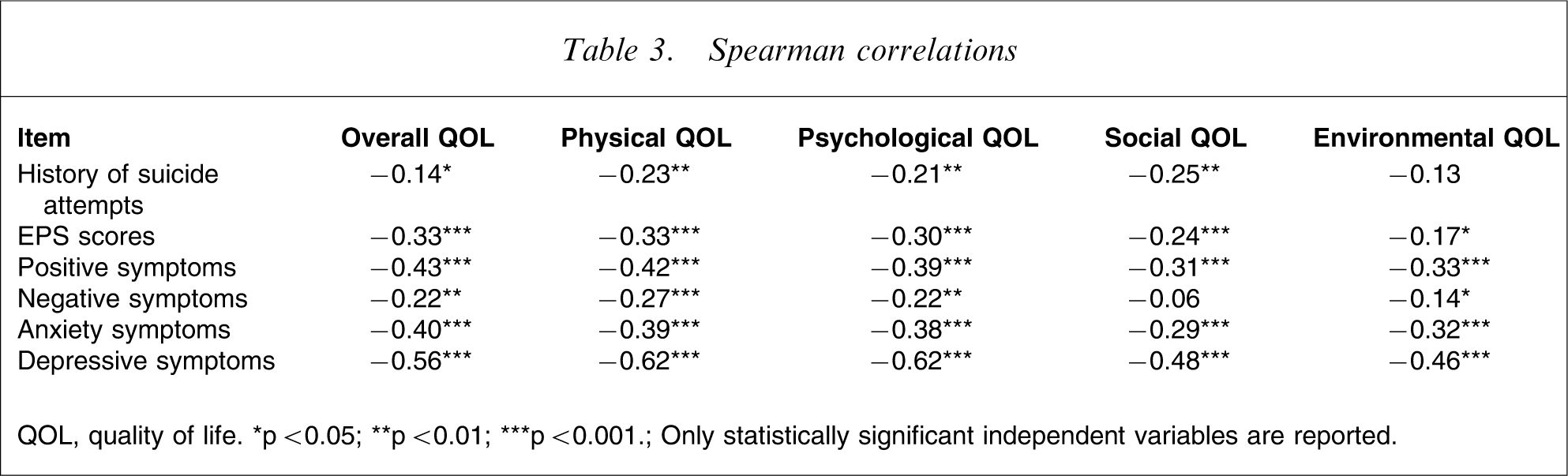
QOL, quality of life. ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Only statistically significant independent variables are reported.
Methods
Settings and subjects
The study was conducted between January 2005 and March 2006. The subjects were recruited from patients diagnosed with schizophrenia who were attending the Li Ka Shing Psychiatric Outpatient Clinic (LKSOPD) at the Prince of Wales Hospital. The catchment area of the LKSOPD covers a population of approximately 800 000.
Patients who met the following criteria were invited to participate in the study: (i) diagnosis of schizophrenia according to the DSM-IV [13]; (ii) age between 18 and 60 years; (iii) length of illness ≥5 years; (iv) being an outpatient living independently in the community (i.e. not in residential facilities); (v) being clinically stable for at least 3 months before recruitment (clinical stability was defined as no change in medication or other forms of treatment or an increase in the dose of drug(s) by ≤50% over the past 3 months [14] because no more accurate data, for example no change in Brief Psychiatric Rating Scale (BPRS) scores, could be used due to the cross-sectional nature of the study); (vi) having at least one family member cohabiting with the patient; and (vii) Chinese ethnicity with fluency in the Cantonese dialect. The exclusion criteria were: (i) history of or ongoing major chronic medical or neurological condition(s); and (ii) past or current significant drug/alcohol abuse other than nicotine abuse.
Stepwise multiple regression analysis
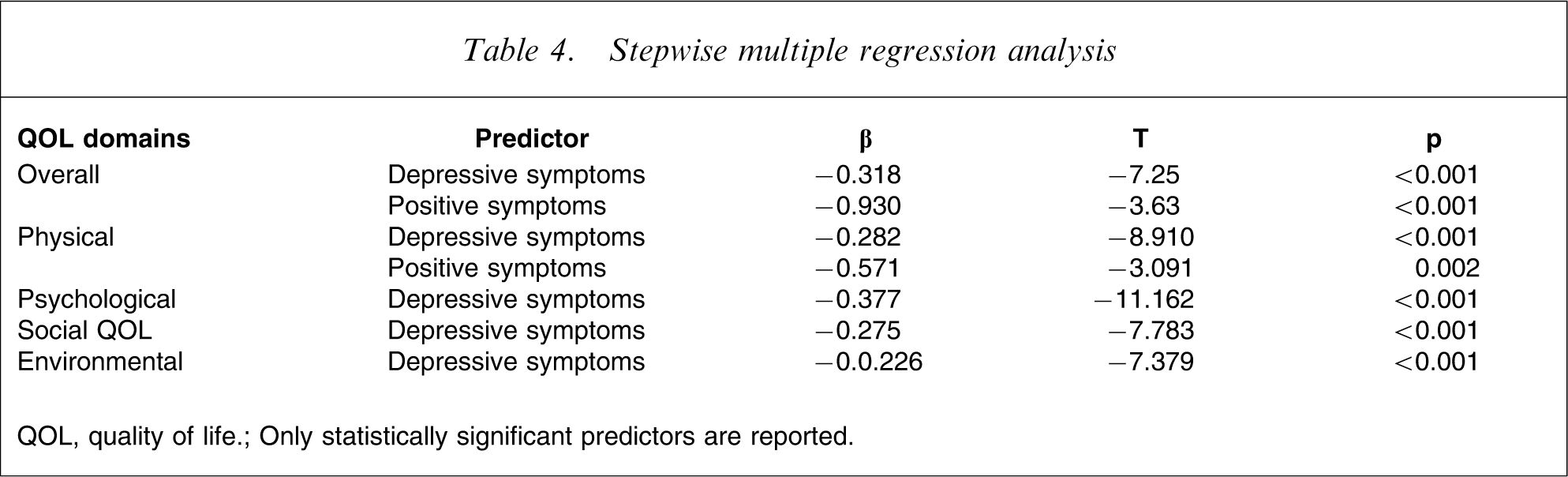
QOL, quality of life.
Only statistically significant predictors are reported.
The family is viewed as the root of humankind in Chinese culture [15], and it remains one of the major providers of care for psychiatric patients in Hong Kong even though community-based residential facilities have been relatively well developed over recent decades [16]. Therefore, schizophrenia outpatients living with their family members were expected to be better adjusted and to have higher QOL than hospitalized patients and those living independently or in supported community facilities. In addition, there are at least two advantages of investigating chronic schizophrenia patients instead of acute ones. First, their diagnosis was more likely to be firmly established. Second, they were more likely to be on stable doses of maintenance medication that can influence QOL. These arguments explain why patients with chronic schizophrenia in this particular locality were chosen as targets for the study.
The reported effect size (correlation coefficient; r) between one of potential predictors, the depressive item in BPRS, and QOL outcome measures of physical health, psychological, social relationships and environment were −0.31, −0.39, −0.27 and −0.29, respectively, in a previous study [8]. Based on these values, using power calculation [17] the minimum number of patients needed to achieve 80% power would be 65, 40, 93, and 66, respectively, at α
The study was designed and conducted according to the Declaration of Helsinki [18]. The study protocol was approved by the Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee in Hong Kong. Written consent was obtained from all participants.
Data collection
A questionnaire was designed to collect sociodemographic data including age, sex, marital and employment status, educational level, number of persons living with, age at first treatment, overall duration of treatment, number of hospitalizations, and monthly income.
Outcome measures
World Health Organization Quality of life schedule–brief version (Hong Kong translation)
The World Health Organization Quality of Life Schedule (WHOQOL)-Brief version [1] is a 26-item, self-administered generic questionnaire that covers four domains: physical health, psychological health, social relationships, and environmental factors. Patients assess their satisfaction with each item during the past 2 weeks on a 5-point scale (from 1, very dissatisfied, to 5, very satisfied). The WHOQOL-BREF (HK) included two additional questions on ‘the availability of food’ and ‘acceptance by others’ in the psychological domain because food and respect and acceptability are both very important issues in Confucian culture. The WHOQOL-BREF (HK) showed acceptable psychometric properties in the Hong Kong Chinese population. The Cronbach alphas for internal consistency ranged from 0.67 to 0.79 in the four domains; the intra-class correlation coefficient (ICC) for test–retest reliability ranged from 0.64 to 0.90; and the overall goodness of fit of the four domains for construct validity ranged from 0.86 to 0.99 [19].
Brief psychiatric rating scale
Psychiatric symptoms were assessed by BPRS [20]. For this study, the following three mean scores were used: 1, positive symptoms of conceptual disorganization, suspiciousness, hallucinatory behaviour, and unusual thought content; 2, negative symptoms of emotional withdrawal, motor retardation, blunted affect, and disorientation; and 3, symptoms of anxiety and tension.
Simpson and angus scale of extrapyramidal symptoms and barnes akathisia rating scale
For the sake of convenience, the sum scores of the Simpson and Angus Scale of Extrapyramidal Symptoms (SAS) [21] and Barnes Akathisia Rating Scale (BARS) [22] were used to measure drug-induced extrapyramidal side-effects (EPS).
17-item Hamilton depression rating scale]
The 17-item Hamilton Depression Rating Scale (HAM-D) [23] is an observer-rated scale that was used to assess the presence and severity of depressive symptoms.
Course of assessment
Participants were selected by a computer-generated random number from patients who met the study criteria on the day of their attendance. Those who signed the consent form were interviewed before or following their consultation in the LKSOPD. The principal author assessed all of the subjects throughout the study. Psychotic and depressive symptoms and EPS were measured by BPRS, HAM-D, SAS, and BARS, respectively, supplemented by a review of the case notes. The WHOQOL-BREF (HK) was given to the participants who were asked to respond to each item; items were read aloud if it was deemed necessary. To check the consistency of the principal author's ratings, before the study an interrater reliability exercise of all clinical rating instruments was conducted with another research psychiatrist on 20 randomly selected patients with schizophrenia. The ICC for BPRS overall and positive, negative, and anxiety symptom scores, SAS, BARS, and HAM-D were 0.867, 0.927, 0.92, 0.763, 0.927, 0.835, and 0.935, respectively. All ICC were satisfactory.
Statistical analysis
One-sample t-test was carried out to compare the QOL ratings in the present study with normative data obtained for the Hong Kong general population. The relationships between sociodemographic and clinical factors and QOL domains were measured by Pearson correlation analysis given that the data followed normal distribution: otherwise, Spearman rank correlation analysis was used. To explore the relative association between each of the sociodemographic and clinical factors that had significant correlations with each QOL domain, partial correlation analysis was used to control for possible confounding variables, namely, remaining variables that had significant correlations with QOL. Multiple regression analysis using the stepwise method was used to identify factors that affected each of the QOL domains. Hierarchical (sequential) multiple regression analysis was used to explore the individual contribution of depressive symptoms to each QOL domain after the effects of other sociodemographic and clinical factors were controlled, because depressive symptoms have been reported to be one of the strongest predictors of QOL in Western countries [2, 24, 25]. Categorical variables were included as dummy variables. To attempt to avoid multicolinearity, tolerance was used to measure the strength of the linear relationships between the independent variables. In this case, a cut-off of ≥0.4 was regarded as acceptable. The use of two-tailed tests and the setting of the level of statistical significance at p < 0.01 reduced the potential of inflated Type I error due to multiple tests. Furthermore, a re-calculation of power based on the results was made using Cohen's criteria [17].
Results
A total of 227 eligible patients were approached, of whom 200 agreed to participate in the study. Table 1 shows the sociodemographic data of the whole sample. There was no significant difference between the study subjects and those patients who refused to participate with regard to age, sex, age at onset, and length of illness. Table 2 compares QOL between the study subjects and normative data obtained for the general population in Hong Kong.
Correlation analysis
Table 3 shows the statistically significant correlations between clinical factors and all QOL domains. For the history of suicide attempts, EPS scores, positive, negative, and depressive symptoms that had significant correlations with QOL, the relative association between each of them and all QOL domains was explored by using partial correlation analysis. Finally, only depressive symptoms had a significant negative relationship with each QOL domain, while positive symptoms were inversely correlated with overall QOL and the physical QOL domain, and negative symptoms were positively correlated with the social QOL domain.
Multiple regression analysis
Results of multiple regression analyses with the stepwise method to explore the predictors of QOL are shown in Table 4. All variables that had a significant correlation with QOL at the α=0.05 level and those that were described as predictors of QOL in the literature [3, 8, 26–30], including education level, marital status, antipsychotic medication, illness duration, poor living situation, number of hospitalization, and history of crime/violence, were entered as independent variables and each QOL domain was entered as a dependent variable. All QOL domains were significantly predicted by one or more clinical characteristics. Specifically, overall QOL was significantly predicted by depressive and positive symptoms (F(2,196)=55.3, p < 0.001), which accounted for 35.4% of the variance in overall QOL. Physical QOL was significantly predicted by depressive and positive symptoms (F(2,196)=70.2, p < 0.001), which accounted for 41.2% of the variance. Psychological QOL was significantly predicted by depressive symptoms (F(1,197)=124.58, p < 0.001), which accounted for 38.4% of the variance. Social QOL was significantly predicted by depressive symptoms (F(1,197)=60.58, p < 0.001) which accounted for 23.1% of the variance. Environmental QOL was significantly predicted by depressive symptoms (F(1,197)=54.44, p < 0.001), which accounted for 21.3% of the variance. The results of hierarchical multiple regression analysis showed that depressive symptoms accounted for 7.1%, 9.8%, 12.2%, 8.5%, and 7.4% of the variances in overall QOL and the physical, psychological, social, and environmental domains of QOL, respectively, after the effects of other sociodemographic and clinical factors were controlled.
Re-calculation of power
The correlation coefficient (r) between one of the potential predictors, the depression item in the BPRS and QOL outcome measures of physical health, psychological, social relationships, and environment were −0.44, −0.50, −0.34, and −0.42, respectively. Using Cohen's method [17], the power was >0.99 in all cases at α=0.05 (one-tailed).
Discussion
To the best of our knowledge, this is the first study aimed at exploring QOL and its correlates in Chinese outpatients with schizophrenia living with their families.
The results partly supported our first hypothesis, in accordance with results of previous studies [31, 32]. Contrary to our expectation, no statistically significant differences between the two groups in environmental QOL were found, probably because the subjects lived in their family homes. The distress/protection model suggests that QOL is the outcome of an interaction between several protective factors (e.g. self-esteem, social support, and avoidance) and a number of distressing factors (e.g. psychopathology and drug side-effects) [31]. QOL increases if protective factors, such as the possible social support derived from families in the present study, predominate over distress factors, which may explain the patients’ good environmental QOL. This finding requires replication.
As for the second hypothesis, no sociodemographic characteristics but a host of clinical factors were significantly correlated with the QOL domains. Similar findings have been reported [33, 34]. However, in partial correlation analysis, depressive symptoms had a strong mediating role over other QOL correlates, thus confirming the widely held view that depression is one of the strongest predictors of QOL in schizophrenia patients [2, 24, 25]. This finding could be best interpreted by the distress/protection QOL model [31]. According to this model, one or more QOL domains could decrease if distressing factors such as depressive symptoms predominate over protective factors. This model may also apply to the inverse association between positive symptoms and the physical QOL domain. Surprisingly, more severe negative symptoms were associated with a higher social QOL domain, a finding that is opposite to most but not all [35] earlier conclusions [2, 11, 26]. This striking result could be partly explained by the assumption made by Jenkins et al. [36] that negative symptoms are not part of the primary process of schizophrenia, but constitute a secondary adjustment to both external and internal overstimulation. Therefore, the effect of negative symptoms would be to exert some degree of control over environmental stimulation, and the more effective they are, the better the patient perceives his or her QOL, particularly in its social domain. Again, these are speculations and need further studies to replicate.
The third hypothesis that depressive and psychotic symptoms would significantly predict QOL was also confirmed. Depressive symptoms were found to significantly negatively predict each QOL domain, thus underscoring the important role that depressive symptoms play in contributing to QOL in clinically stable outpatients with schizophrenia. This finding is also consistent with that of previous reports [11, 35, 37]. At the same time, severe positive symptoms were found to predict poor overall and physical domains of QOL. Surprisingly, this finding was contrary to the widely held conclusion that QOL is more related to negative symptoms and only weakly related to, or independent of, positive symptoms [2, 11, 26]. The discrepancy between the literature and our findings might be mainly due to traditional Cantonese cultural factors, namely the influence of traditional Confucian ideas that champion modesty or golden mean (zhong yong zhi dao) and oppose polarity or extremes, which lead to dramatic attitudes of the general population toward different psychotic symptoms: namely, negative symptoms are relatively more acceptable while positive symptoms are more stigmatized. A vivid example of the diverse attitudes toward positive and negative symptoms is the nickname for schizophrenia, which is loaded with stigma. In China, schizophrenia patients are generally divided into two types by the lay public. ‘Psychotic patients with guns (wu feng)’ refers to patients with predominantly positive symptoms. This metaphor suggests that patients with positive symptoms are more likely to behave aggressively and are potential threats to public safety and harmony. Consequently, they should be strictly monitored and controlled in restricted settings. ‘Psychotic patients with pens (wen feng)’ applies to patients presenting mainly with negative symptoms indicating that they are gentle and quiet persons and should be more acceptable in the community although they suffer from psychotic disorders. These different attitudes would have an impact on patients’ self-esteem and coping mechanisms, which has also been reported to influence QOL [11]. However, to date no study has specifically focused on the impact of Confucian culture on QOL. Studies examining QOL in psychotic patients in different sociocultural contexts are warranted.
The discrepancy between the present study and the literature [8, 26] with regard to the relationship between sociodemographic factors and QOL could be partly due to differences in sample size, study design and entry criteria, assessment methods, and the choice of variables. Our findings replicated earlier findings concerning the lack of association between sociodemographic factors and QOL domains [38–40]. Anxiety and drug-induced side-effects were highly correlated with most QOL domains in the present study, which is broadly consistent with previous reports [2, 41]. However, this correlation lost statistical significance after the effect of other correlates of QOL were controlled for, and it also failed to significantly predict QOL possibly because of the relatively low level of anxiety and side-effects observed in the present study. Therefore, the conclusion should be interpreted with caution, and requires replication.
Strengths and limitations of the study
The major strength of the present study is the fairly large, randomly selected, ethnically homogenous sample. However, the results should be interpreted with caution with several methodological limitations in mind. The first limitation is the relatively limited scope of variables examined; it is widely believed that in addition to sociodemographic and clinical data, a complex interaction of other factors, for example patients’ ways of coping with symptoms and associated distress, self-esteem, premorbid adjustment, and social support network, could play a substantial role in the determination of QOL [11]. Second, the results are applicable only to clinically stable schizophrenia outpatients living with families in the community, thus precluding generalization to patients with different clinical status or those living in residential facilities. Third, patients with concomitant and/or substance abuse were excluded from the study. Because in Hong Kong only approximately 10% of schizophrenia patients abuse alcohol and/or illicit substances [42], their exclusion may not have led to significant sampling bias. Fourth, the study was cross-sectional therefore the exploration of causal relationship was tentative. The fifth limitation concerns the assessment; all ratings were made by the same investigator. The optimal solution would have been to assess QOL and the clinical and demographic aspects independently. Sixth, the choice of QOL measures is limiting; the WHOQOL-Brief version is a generic QOL instrument and it may not be sensitive enough to identify small changes in QOL. At this point, no Cantonese version of schizophrenia-specific QOL rating instrument is available in Hong Kong. Finally, there was no control group in the study; comparisons were made with the normative data obtained for the general population in Hong Kong.
Clinical implications
The results underline the deleterious effect of depressive, positive and negative symptoms on QOL in Chinese schizophrenia patients living with their family, thus suggesting that effective therapeutic interventions that alleviate the aforementioned symptoms might be of considerable benefit in improving QOL. The positive association between QOL and EPS found in the study warrants the more widespread application of second-generation antipsychotic drugs that have no, or minimal, such side-effects to improve patient QOL. Because of its significant correlation with the physical, psychological, and social domains of QOL, more attention should be paid to schizophrenia in patients with a history of suicide attempts.
Footnotes
Acknowledgements
The authors would like to thank the staff in the Day Hospital at Shatin Hospital, and the Li Ka Shing Psychiatric Outpatient Clinic at the Prince of Wales Hospital for their assistance in the project. The authors also express their gratitude to the two anonymous reviewers for their several constructive comments and recommendations.