
Abstract
Meta-analytic reviews have reported significant clinical benefits for persistent psychotic symptoms in individuals with a diagnosis of schizophrenia who participate in individual cognitive behaviour therapy (CBT) [1–4]. Accordingly, recent treatment guidelines suggest that CBT should be available for people with schizophrenia [5–8]. As the demand for CBT for psychosis outstrips the availability of trained therapists [2], evaluations of group, as opposed to individual, approaches have been the focus of increasing research attention [9–14]. In these research studies, group-based CBT was found to be effective in reducing rehospitalization rates, feelings of hopelessness or low self-esteem and to improve social functioning, but specific advantages for positive psychotic symptoms in CBT treatments compared to the respective control conditions were not observed in most trials.
Although subjective quality of life (QoL is widely considered as a relevant indicator of people's sense of well-being and satisfaction under current life circumstances [15], and there are consistent reports of patients with schizophrenia reporting lower QoL scores than healthy controls [16–18], only one study to date has explored the effects of CBT on subjective QoL in patients with schizophrenia [19]. Wiersma et al. reported significant advantages for CBT on QoL measures 9 months after treatment, when compared with treatment as usual [19]. The Atkinson et al. results, however, suggested that a group intervention educating patients about schizophrenia and antipsychotic treatment using standardized presentation of educational material and mainly didactic intervention strategies also improves QoL in comparison to standard treatment [20].
The aim of the present paper was to assess the differential efficacy of a brief group CBT intervention in comparison to a psychoeducation (PE) group programme in patients with acute schizophrenia on QoL at post-treatment and 6 month follow up.
Earlier analyses of data from the same trial indicated that CBT was superior to PE in terms of rehospitalization at 6 month follow up [12]. At 24 months there were no significant group differences regarding readmission, symptoms or compliance with medication. On a descriptive level, however, patients who received CBT on average experienced 21.8% fewer re-hospitalizations, 71 days fewer in hospital and higher compliance ratings at the 24 month follow up [13].
Method
This research project was approved by the local Ethics Committee of the Faculty of Medicine, University of Cologne, Germany.
Subjects
Patients were recruited from consecutive acute admissions to the inpatient unit of the Department of Psychiatry and Psychotherapy at the University of Cologne between July 1999 and December 2000. They were aged 18–64 years, met criteria for an episode of schizophrenia, schizoaffective or other psychotic disorder (ICD-10: F20, F23, F25) and were recommended antipsychotic medication. Any patient with a primary diagnosis of drug or alcohol dependence, organic brain disease, learning disability or hearing impairment was excluded from the study.
Study design
Within 14 days of hospital admission, treating psychiatrists were approached by the two therapists to seek permission for the inclusion of their patients in the study. When permission was given, the case notes were fully reviewed and the patients were approached to participate in the study. Patients were randomized to receive either CBT or PE treatment after they had provided full informed consent. Randomization was conducted by computer-generated random numbers for blocks of eight participants. The results were placed in sealed envelopes and opened at the time of treatment allocation.
Sessions of both interventions were delivered to groups of eight patients within a therapy envelope of 8 weeks. The interventions took place in the psychiatric hospital. Groups in both interventions were usually led by two therapists: an experienced and CBT-trained psychiatrist (A.B.) and a clinical psychologist (B.K.). A minority of the session were led only by one of the therapists. The sessions were carried out while the patients were inpatients and continued when they were discharged during the therapy envelope period. All interventions were an adjunct to routine hospital care and patients remained under the medical supervision of the responsible consultant psychiatrist who alone determined the pharmacological regimen, timing of discharge and readmission.
Assessments
A wide range of assessments was administered to participants at baseline, after treatment, at 6 month follow up and at 24 month follow up. The primary outcome measures were readmission, relapse, clinical symptoms as measured on the Positive And Negative Syndrome Scale [21] and compliance with medication [12,13]. The current paper presents results on the secondary outcome measure of subjective QoL as measured using the Modular System for Quality of Life (MSQoL) [22] after treatment and at 6 months follow up. Putative moderating variables of treatment effects (coping behaviour, locus of control and self-efficacy) were assessed on self-rating scales [23,24]. Results regarding moderating variables will be presented elsewhere.
Measures
Objective information was assessed on short demographic interview and was extracted from case notes.
QoL was assessed using the MSQoL, a self-report instrument consisting of a demographic module and four subjective QoL modules (core module, partnership module, family module and professional occupation module) [22]. The MSQoL was derived from eight internationally well established generic QoL instruments, and demonstrated good reliability and validity comparable to that of the Shortform 36 [22,25]. Recently the measure has been used for the assessment of QoL in a big international research effort in people at risk of psychosis [26]. Median values for internal consistencies were 0.88 (range = 0.73–0.92) in the general population and 0.83 (range = 0.78–0.92) in patients with schizophrenia. In the present study we focused only on the core module, which consists of seven areas of QoL (47 items each rated on a 7 point scale): Physical Health (e.g. limitations to perform moderate–vigorous activities), Vitality (e.g. feeling full of life; feeling relaxed and comfortable; amount of time feeling tired), Psychosocial QoL (e.g. satisfaction with relationships with others; feeling self-confident), Affective QoL (e.g. feeling under strain, stress or pressure; getting easily hurt), Material QoL (e.g. satisfaction with financial situation or living conditions), Spare Time QoL (e.g. interest in hobbies at home or outdoor), and General QoL (e.g. having problems in general; enjoying life). Raw scores were rescaled to a range from 0 to 100 so that a higher score indicated higher QoL.
Treatment groups
Group CBT treatment
The group CBT treatment was based on the approach by Tarrier et al., who used coping strategy enhancement, problem solving and relapse prevention in patients with psychosis [27,28]. This treatment has been found to be effective in short-term follow ups in patients with chronic [27–31] and recent onset psychosis [32,33]. It has been combined with motivational interviewing and family interventions in dually diagnosed patients in individual therapy settings [34,35]. The group CBT intervention focused on the treatment of auditory hallucinations and delusions, associated symptoms and problems (e.g. anxiety, depression), relapse prevention and associated problems and enhancing medication compliance. Because it was our clinical experience that psychotic symptoms are recognized by most patients as a kind of personal dysfunction (especially during recovery), which is likely to be associated with negative self-evaluations, we integrated the component ‘improving self-esteem’ [34] into the intervention in order to foster feelings of hope and engagement with therapy. The intervention included 16 sessions in 8 weeks. Sessions followed a semi-structured format and lasted between 60 and 90 min, interrupted by a 5–10 min break.
Treatment consisted of the following elements: (i) assessment and engagement (sharing information about voices and delusions, models of psychosis); (ii) improving self-esteem; (iii) formulation of key problems; (iv) interventions directed at reducing the severity and the occurrence of key problems; and (v) relapse prevention/keeping well. The following specific CBT strategies were used: formulation, guided recovery, symptom monitoring, exposure/focusing strategies for managing voices, hypothesis/reality testing, re-framing attributions, rational responding, coping strategy enhancement, distraction techniques, role play, anxiety management, depression and self-esteem work, medication compliance/motivational interviewing, schema work, relapse prevention and keeping well strategies.
Group psychoeducational programme
The PE programme was similar to the PE group training for patients developed by Hornung et al., which demonstrated improvement in medication compliance and re-hospitalization rates in patients with schizophrenia [36,37]. The programme included eight sessions in 8 weeks. Sessions followed a semi-structured format and lasted between 60 and 90 min, occasionally interrupted by a 5–10 min break. It covered the following topics: symptoms of psychosis, models of psychosis, effects and side-effects of medication, maintenance medication, early symptoms of relapse, relapse prevention. The approach was primarily didactic and included the following strategies: formulation, guided discovery and motivational interviewing.
Data analysis
Sample characteristics were analysed using t-test or χ2 test to check the randomization. The lost-to-follow up mechanism was analysed using t-test or χ2 test by comparing sociodemographic data at the pre-treatment stage between the initial sample and the remaining participants at 6 month follow up as well as between the CBT group and the PE group in the remaining participants. The effects of treatment on QoL were checked using the t-test for dependent samples. All analyses of treatment effects were calculated by intention to treat. For pre–post-treatment and pre-follow-up analysis, a Wilcoxon signed–rank test was used. Within-group effect sizes (ES) were calculated in accordance with Rector and Beck [5] by using the mean difference divided by the pooled standard deviation. To test the differential effects of CBT and PE on QoL, an ANCOVA was carried out using pre-treatment scores as covariants. Two-tailed tests of significance were used in all analyses with p set at .05.
Role of the funding source
The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
Characteristics of the sample
During the study period 189 patients fulfilled inclusion criteria. Of these, 57 patients were not approached, either because they were involuntary admissions, formally detained under the Mental Health Act and could therefore not be included in randomized trials or because during their inpatient stay the patient flow was too small to form a group of eight patients to start a group intervention. Of the remaining 132 subjects who were approached to be included in the trial, there was a 33.4% non-participation rate (n = 44) due to refusal, lack of German, inability to complete assessment or rapid discharge. Table 1 shows the characteristics of the 88 patients included in the study. Participants had, on average, been hospitalized between two and three times because of psychosis in their lifetime and had a mean time since diagnosis of > 4 years. Most patients were single and lived alone or with their families. Only a minority was employed on a regular basis. There were no significant differences between the CBT and the PE group at baseline with regard to age, gender, time since diagnosis, or number of admissions.
Subject characteristics (n = 88)
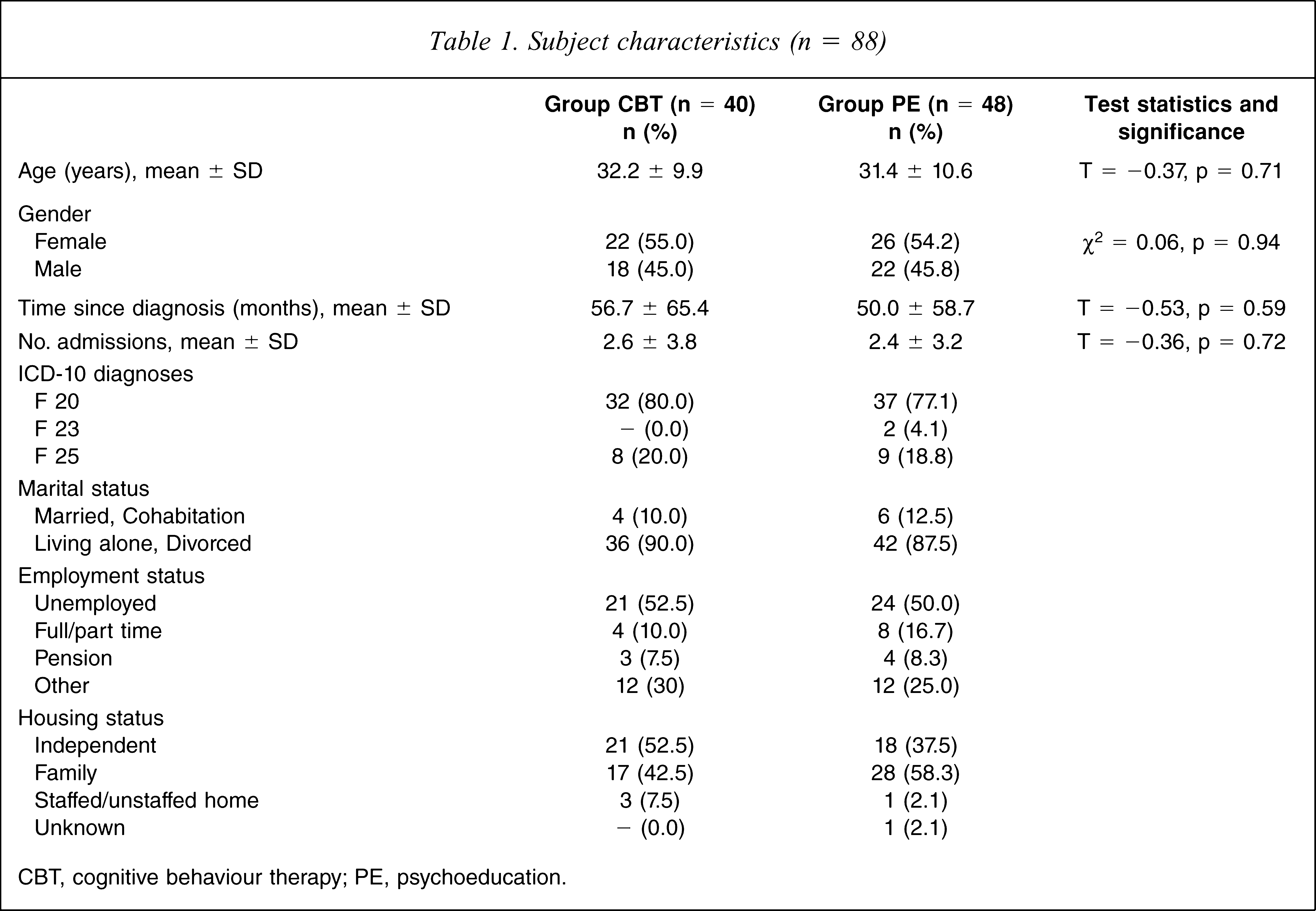
CBT, cognitive behaviour therapy; PE, psychoeducation.
From the initial sample of 88 participants, QoL data were available for 68 participants (77.3%). There were no significant differences on demographic data between the total initial sample and those who completed the MSQoL. A total of 80.7% of the total sample (n = 71) were assessed at 6 month follow up. In the CBT group 9/40 subjects (22.5%) and in the PE group 8/48 patients (16.7%) were lost to follow up. There was no significant difference in attrition rates between the intervention groups. Of the remaining participants 64 patients (90.1%) completed the QoL measure. Four patients (5.9%) of those who initially completed the MSQoL were lost to follow up at 6 months. There were no significant differences in demographic data between the total initial sample (n = 88), the total follow-up sample (n = 71) and those who completed the MSQoL at follow up (n = 64).
Adherence to treatment
After randomization one CBT patient and two PE patients failed to attend any treatment sessions. The maximum number of sessions (CBT maximum 16 sessions; PE maximum eight sessions) were delivered to eight of 40 patients in the CBT group and 13 of 48 in the PE group. On average, in the CBT group patients attended 11.9 ± 4.1 sessions and in the PE group patients attended 6.4 ± 1.8 sessions.
QoL
The QoL data from baseline, after treatment and 6 month follow up are presented in Table 2. In general, QoL improved over time in both treatment groups. From pre-treatment to post-treatment assessment no significant within-group improvements were found in the CBT group, but in the PE group improvements were observed for Physical Health (F = 8.618, p = 0.006) and Affective QoL (F = 5.213, p = 0.029). Within-group pre–post-treatment ES for general QoL were 0.06 for CBT and 0.07 for PE. At 6 month follow up significant within-group improvements were found in both groups. In the CBT group significant improvements were present for Vitality (F = 5.898, p = 0.024), Material QoL (F = 4.733, p = 0.042), Spare time QoL (F = 4.412, p = 0.049) and in the PE group for Physical Health (F = 15.587, p < 0.001; ES = 0.38), Vitality (F = 25.093, p < 0.001; ES = 0.35), Psychosocial QoL (F = 13.882, p < 0.001; ES = 0.33), Material QoL (F = 5.981, p = 0.020; ES = 0.15), Affective QoL (F = 10.919, p = 0.002) and General QoL (F = 13.693, p < 0.001). Within-group pre-treatment follow-up ES for general QoL was 0.25 for CBT and 0.29 for PE. No significant differences between CBT and PE were found at pre-treatment or post-treatment assessments, or at 6 month follow up.
MSQoL scores
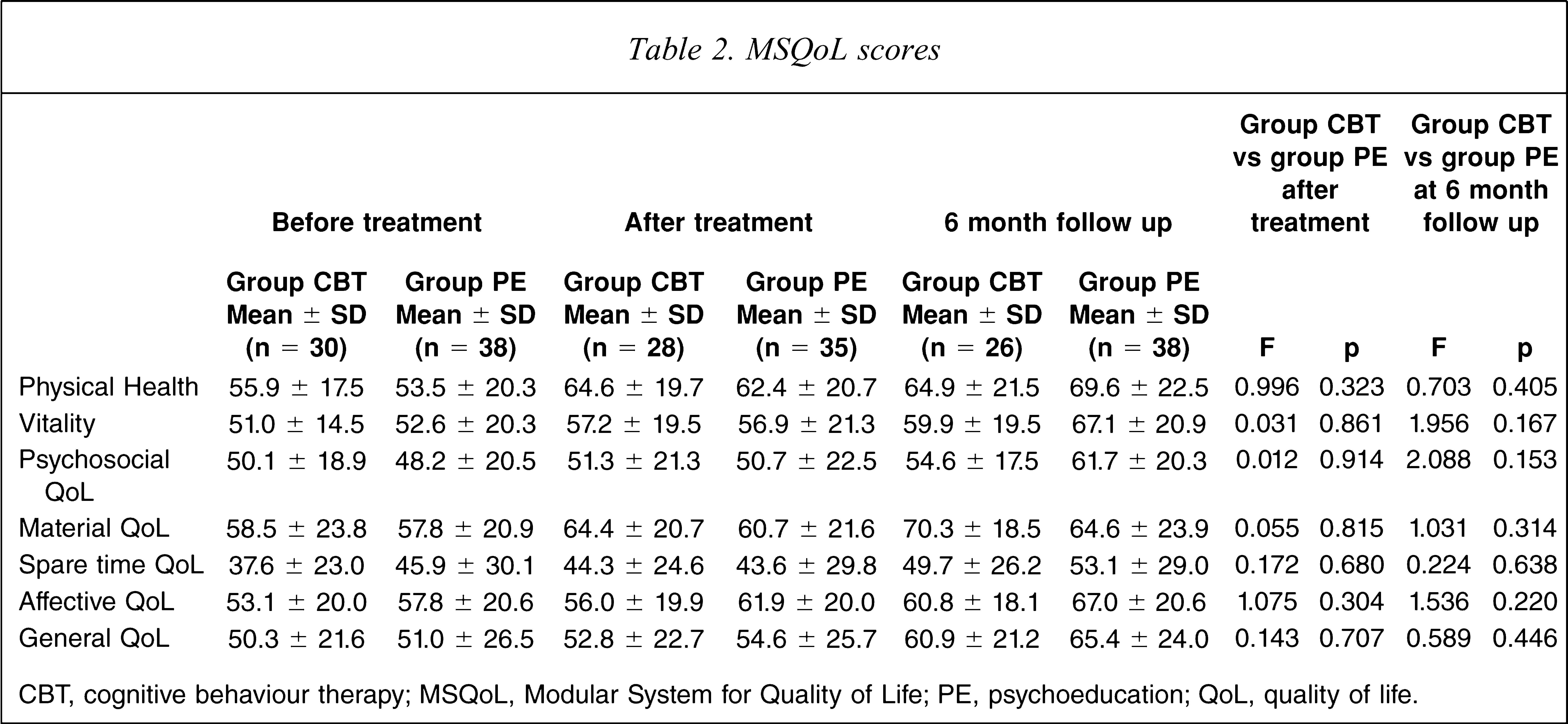
CBT, cognitive behaviour therapy; MSQoL, Modular System for Quality of Life; PE, psychoeducation; QoL, quality of life.
Medication use
The mean dosage of typical antipsychotics converted to chlorpromazine equivalents [38] was nearly the same at baseline and follow-up evaluations, although there was a wide range of dosage within the treatment groups (before treatment: CBT = 431.7 ± 201.0 mg, PE = 375.0 ± 349.5 mg; after treatment: CBT = 158.8 ± 73.3 mg, PE = 520.0 ± 413.3 mg; follow up: CBT = 358.3 ± 340.4 mg, PE = 361.4 ± 340.9 mg). All patients were treated with antipsychotics, most with atypicals (before treatment: CBT = 80%, PE = 85%; after treatment: CBT = 93.5%, PE = 87.8%; follow up: CBT = 88.9%, PE = 89.2%). Approximately one-third of participants also received antidepressant medication (before treatment: CBT = 26.3%, PE = 25.0%; after treatment: CBT = 25.8%, PE = 38.9%; follow up: CBT = 31.0%, PE = 28.9%). No significant differences emerged between treatment groups at pre- or post-treatment assessment or at follow up.
Discussion
This was the first study that compared a brief group CBT with a group PE programme as an adjunct to routine care in acute inpatients with schizophrenia in terms of effect on QoL at post-treatment assessment and at 6 month follow up. Earlier analyses of the trial indicated superiority of CBT on rehospitalization rates at 6 months follow up, which were maintained on a descriptive level at 24 months follow up [12,13]. With regards to QoL outcomes, both groups improved significantly in most domains 6 months after treatment. There were no significant between-group differences at post-treatment assessment and at 6 months follow up. Moreover, on a descriptive level the within-group improvements seemed to be more pronounced in the PE group rather than in the CBT group. Results suggest that strategies that include cognitive, affective and psychomotor components such as the group CBT intervention are more likely to change complex behaviour patterns influencing rehospitalization, relapse and compliance than didactic interventions that focus on knowledge and concepts of illness such as the PE programme. These changes of complex behaviour by CBT might be associated with a slightly unfavourable subjective well-being during the post-acute recovering phase when compared with PE.
Although only 77% of the randomized sample completed the QoL measure at intake, <10% of the patients for whom data were available at the initial assessment were lost to follow up at 6 months. This is a very low follow-up loss rate compared to other trials of CBT and PE in patients with schizophrenia [2,3]. There were no significant differences between the subsample and the total sample at intake and the reasons for this relatively high number of missing data at intake were more of a logistical nature than due to patient decisions.
The QoL outcomes in the current study compare well with earlier studies. The observed within-group ES of 0.25 in the CBT condition at 6 months follow up are in line with the ES reported by Wiersma et al. (ES = 0.28) 9 months after CBT treatment [19]. The ES of the QoL improvement in the PE condition (0.29) was higher than the ES described by Atkinson et al. (ES = 0.15) [20]. This difference might be due to the fact that Atkinson et al. primarily studied a chronic population with stable symptoms, whereas the present trial addressed acute psychotic patients with fewer hospitalizations, who might be more responsive to treatment. All ES observed, however, were small when applying Cohen's definition [39]. Because the significant advantages for the CBT and PE conditions with regard to QoL in the two earlier studies were primarily based on non-improving or worsening of the patients in the respective control conditions [19,20], the significant advantages were lost when comparing CBT with a valid comparator such as PE. Because in the present study the patients of the CBT as well as of the PE condition improved, we did not find significant differences between the conditions. The pattern, that the specific intervention was not superior to the control condition, was also found in other studies, which used enriched packages of care as the control condition. Röhricht and Priebe did not find significant differences between a body-oriented therapy and matched supportive counselling on QoL in patients with schizophrenia [40]. Moreover, individual CBT studies using befriending or supportive counselling as control conditions also failed to show significant benefits for CBT on schizophrenia symptoms at some assessment occasions [29, 35, 41].
Methodological issues
To our knowledge this is the first study that compared a CBT intervention with a PE programme in patients with schizophrenia. Therefore it is also the first time that conclusions regarding the differential efficacy of CBT and PE on QoL in patients with schizophrenia can be drawn. There were several methodological limitations, however. First, due to logistic reasons we could deliver the interventions only to inpatients with acute schizophrenia. Although we doubt that this is a significant source of bias, one might not be able to generalize the results to other clinical settings without further considerations. Second, the conclusions about treatment specificity could be limited by the fact that we did not control for contact time. Although both interventions were an adjunct to treatment as usual (including pharmacological treatment, daily clinical assessments, supportive therapy, group meetings, occupational therapy, counselling by social workers) and therefore the difference of attention between the two interventions was small compared to the overall attention, the face-to-face contact with therapists within the trial was twice as much for patients in the CBT group than for patients receiving PE. Moreover, no formal measures of therapist adherence to the manual were used nor did we use any formal assessments of therapist competence. Although the conceptual framework differed relevantly between CBT and PE, we cannot be sure that the treatment that was actually delivered, differed between the treatment conditions and that CBT standard was adequate. Third, moreover, due to problems of statistical power with regards to the primary outcome measures (readmission, relapse, clinical symptoms and compliance with medication) we did not introduce a non-specific control condition, which again limits conclusions regarding treatment specificity. Thus, we cannot rule out that QoL of the patients would have improved independently from the psychological interventions during recovery from the acute phase. But, because almost no effects on QoL for waiting list and treatment as usual control conditions were observed in earlier studies [19,20], this is unlikely to be the case. Fourth, Wiersma et al. reported increasing improvements in some QoL dimensions over time [19], therefore longer follow up might be needed to detect significant differences between groups.
Clinical implications
Despite the methodological limitations mentioned here, the present results suggest that CBT in a brief group format and group PE as an adjunct to routine care both have an impact on QoL in patients with schizophrenia. Although the effects are small in terms of ES, we believe that, given the relative disability of the sample, the improvements are clinically relevant. Thus, in addition to reducing rehospitalization rates in people with schizophrenia [12,13], brief group CBT as well as group PE may contribute to patient well-being by improving their subjective QoL.
Footnotes
Acknowledgements
This work was supported by grant from the Koln Fortune Program (191/1998)/Faculty of Medicine, University of Cologne, Germany.