
Abstract
Early psychosis (EP), in which the terms first-episode psychosis or first-break psychosis are also considered, is an area of developing research intensity. Although it is apparent that considerable progress has been made in establishing best practice criteria and protocols for EP in general, the particular issues pertaining to rural areas have not received the same attention. The purpose of the present study was to conduct a systematic review of the literature of early psychosis programmes, initiatives and research in rural areas in order to help establish the best available evidence. The authors conducted a systematic search of major electronic databases, based on the NHMRC hierarchy of evidence, an established scale, for identified early psychosis cross-referenced with multiple rural terms, between the years 1995 and 2005. A total of 637 articles met the initial search criteria; 206 were identified as having primary significance; three dealt specifically with rural areas. There is a paucity of research findings or published literature concerning the specific needs or characteristics of early psychosis practice or service delivery in rural areas. A number of inferences and suggestions for further research, investigations and policy directions are put forward for consideration.
Evidence-based practice does not rely on assertion or presumption, but on reliable, rigorous and repeated inquiry. The drive towards treatments, strategies and policies that are able to withstand the most clear-sighted interrogation has been a feature of the last decade of mental health research [1]. Furthermore, the identification and treatment of early psychosis (EP) has increased in significance and research activity since the early 1990s [2–5]. There have been substantial improvements in both areas and this has resulted in a number of best-practice clinical guidelines [2, 6–9]. Despite this, there is still work to be done to unpack the relevance of early intervention in psychosis fully [10]. A recent Cochrane review suggests that there have been two main themes in the research [11]. The first pertains to the early detection or identification of psychotic illnesses, especially in the prodromal stage. This refers particularly to the recognition of early symptoms as well as an improved response to manifest signs, with emphasis on this leading to recovery and rehabilitation from an initial episode and the minimization of relapse and secondary morbidity [12]. The second is concerned with phase-specific treatment; the consideration of the prodrome, the acute stage and the recovery. However, it has also become increasingly evident that although there has been significant research in the treatment and care of those with an early psychosis most of it has been in the context of urban settings [11].
There remains a paucity of research literature concerning services or interventions in rural areas [13–15]. The lack of research in mental health in rural areas generally has been recognized, and a review of rural health literature in Australia published in 2000 found nothing at all in the case of EP [16]. Healthy Horizons gave a framework for improving the health of rural, regional and remote Australia and although it highlighted early intervention in primary health care at the earliest possible stage (p.5) as a general strategy, identified Aboriginal health as a priority and gave youth suicide considerable attention, it did not mention early psychosis at all [17]. Integrated primary care programmes and early detection have been called for, but depression has been the rallying call, not psychosis [18–20].
The Canadian situation is similar and in many ways no better [15, 21–23]. By way of explanation, it has been suggested that the ‘metropolitan mindset’ extends to government decision-makers, the location of corporate headquarters and the distribution of universities and other centres of research [16].
Rural areas, which often have different demographic characteristics in age and family structure, often fewer and more thinly spread resources, less access to specialist services and personnel and large geographic areas and great distances to cover, may have to use other methods to deliver best practice [24–32]. What may be suited for a densely populated urban area may not be appropriate for rural areas that do not have a critical mass of incidence of EP [33–35].
Nevertheless, some authors suggest that rural areas may in fact have certain characteristics that enhance resilience and the development of a certain orientation to service delivery [33, 36–38]. In particular, social connectedness and a sense of social capacity may add to cohesion that links agents of intervention and build partnerships in care in a sustainable fashion; that is to say people know each other and work together [39–41]. The general practitioner (GP) or family physician knows the school counsellor who knows the local police officer who knows the minister at the church who knows the primary care nurse who knows the president of the Rotary Club who knows the probation officer who knows the head teacher who knows the football coach who knows the GP. Wainer and Chesters also suggest the valuing of diversity and economic participation as protective factors [36], but the specific impact of these is less clear. It is noteworthy that the first global priority for systematic reviews of health promotion and public health research was identified as “community building interventions (designed to build a sense community, connectedness, cultural revival, social capital to improve social and mental health” [42].
This study should be considered within this context. It has endeavoured to review the known literature, identify the strengths as well as the gaps and suggest future directions for investigation, research and development.
Objectives
The governing criteria were clearly defined in order to maintain a transparency of process, and to maximize the reproducibility of the study. Of course, there is always room for debate over such items, but in an effort to be as inclusive as reasonably possible the following parameters were adopted.
Criteria for selecting studies
There are still some areas of inconsistency in terminology used in the literature to describe the conditions of interest. EP, first-episode psychosis and first-break psychosis, as well as the more specific schizophrenia, are terms that are all commonly found in the literature, and sometimes they are used interchangeably. However, in the present review no particular distinction is made between them. In the report ‘early psychosis’ will be used as the preferred term and will be assumed to cover all of the aforementioned unless otherwise specified. Where appropriate, or where the distinctions are necessary or informative, other terminology may be used, but this will be highlighted.
The geographic terms of interest are also interpreted inconsistently in the literature. Although rural areas were the principal concern of the study, very few reports attempted to identify the criteria for the term, outside of self-definition. It also means different things in different countries and contexts. The size of countries such as Australia or Canada may give quite a different nuance to the term, than the UK. The use of the term ‘remote’ further complicates the issue [43]. However, as Wakerman suggests in a review of terminology from Australia, Canada, the USA, the UK and New Zealand, to be more than 60 km from a primary care facility to one of a higher level may be considered to be rural to remote; to be 400 km away may be considered remote. The imprecision of these definitions is compounded by the use of terms such as ‘driving time’ or ‘transport’ or even ‘transport in good conditions’ [43]. Nevertheless, for the purposes of the present review ‘rural’ will essentially be recognized as being self-defined and, in the absence of actual distances or measures, accepted as such. Some terms, such as ‘northern health’, which has been applied to Canadian studies [13], emerged through the literature search itself. When that occurred the term was added to the search strategy and combined with previous terms and searches.
The use of evidence terms in the search strategy was guided by the Cochrane Database terms [44], textbooks [45] and by terms that came to light through the search itself. Again, when a new term was uncovered, it was entered into the search strategy and combined with previous results.
Only articles written in English were considered. While this is a clear limitation, it is governed entirely by the restricted resources of the researchers and for no other reason.
Although it is recognized that the issue of psychiatric services in rural areas is not new, the search was limited to publications after 1995 (10 year span). This meant that some seminal articles on the rural matters may have been excluded [46, 47], but the subsequent literature fully compensates for their absence.
Types of studies
The study adopted a hierarchy of evidence that recognizes a meta-analysis or systematic review of multiple randomized controlled trials (RCTs) as the most reliable form of evidence (level 1), and expert opinion or single case studies as of lesser certainty [48]. Other levels of evidence in between include single RCTs, controlled, but not randomized studies, uncontrolled studies and descriptive studies. This hierarchy does not preclude expert opinion from being insightful, informative or of as great a utility as an RCT; it may only be a question of reliability, reproducibility and rigor.
Types of participants
Other than being defined within the parameters of early psychosis and rural, no further distinctions were made regarding the participants. Men and women, young and old, all ethnic backgrounds were considered equally. In some cases studies overlapped an age range that may in other circumstances be considered adult or adolescent. For example, some programmes included individuals as young as 13 years old, others drew a line at 18 and some had no age distinctions at all. It was not relevant to the present study whether programmes were considered an adolescent mental health initiative, an adult one, both or neither. The key factor for inclusion was the suspicion, diagnosis or treatment of an EP.
Types of interventions
No intervention was discounted per se. The search included any and all descriptions as well as evaluated programmes. The scarcity of precisely relevant material led to this decision. In cases in which interventions and measures from non-rural studies were reported, the NHMRC hierarchy of evidence was implemented.
Types of outcome measures
The study did not exclude any form of outcome measure, and accepted reports that had process or output measures, rather than outcomes. Again, the lack of any substantial body of literature for rural services was felt to justify this choice.
Search strategies for identification of studies
A systematic review of the literature was undertaken. Searches were made of major electronic databases: Medline, PubMed, CINAHL, Ovid Health Star, PsychINFO, EmBase, the Cochrane Library consisting of all EBM Reviews (Cochrane Database of Systematic Reviews; ACP Journal Club; DARE; Cochrane Central Registry of Controlled Trials) for the years 1995 to September 2005, inclusive. In addition, hand searches of two journals of particular interest and relevance (Australian Journal of Rural Health and Canadian Journal of Rural Medicine) were conducted. The search targeted EP interventions, programmes and programme evaluation with special consideration for rural criteria.
The specific terms used in searching the data bases are given in Table 1. All databases, excluding the Cochrane Library consisting of all EBM Reviews, were searched according to these terms. All Cochrane Library searches were according to the clinical terms only.
Database search strategies
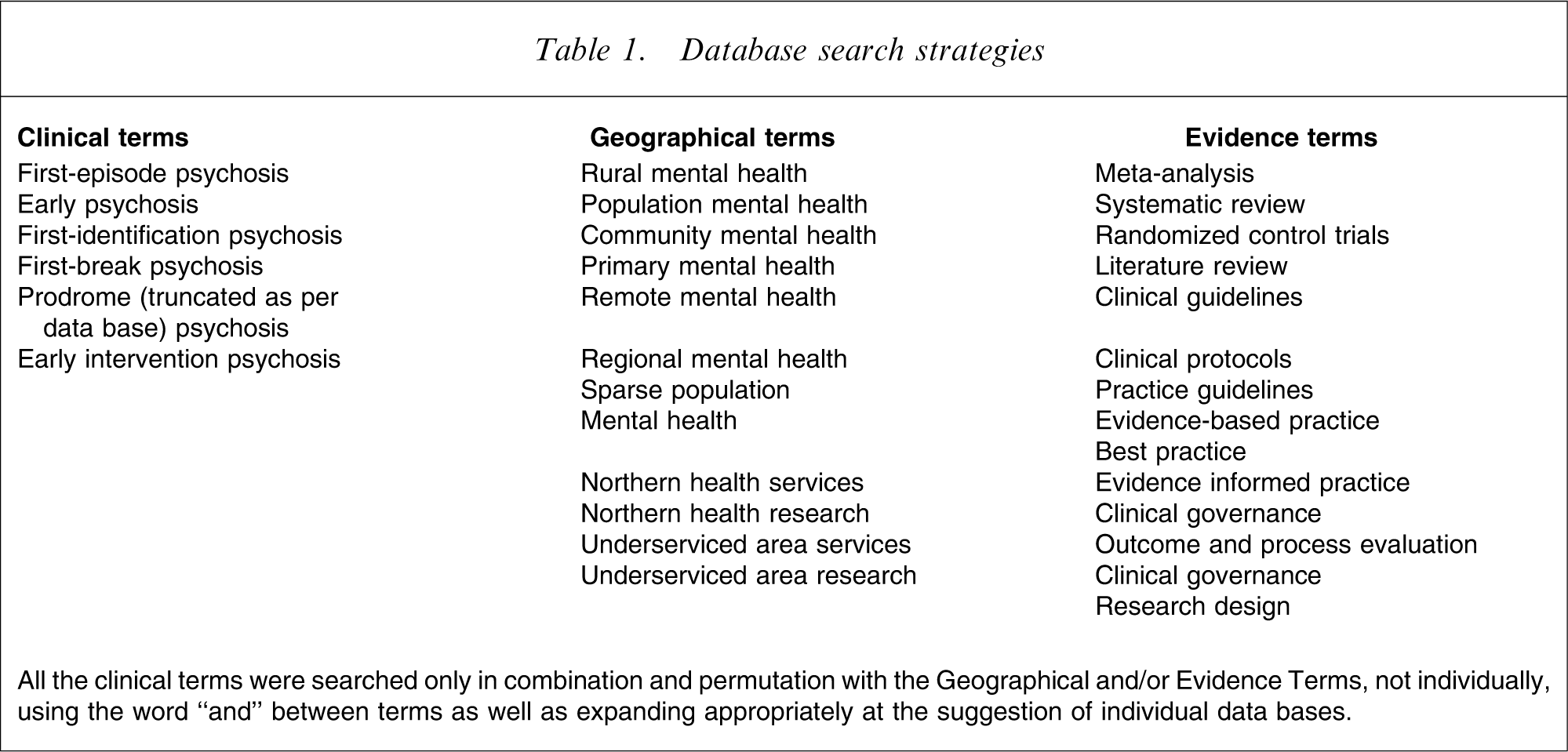
All the clinical terms were searched only in combination and permutation with the Geographical and/or Evidence Terms, not individually, using the word “and” between terms as well as expanding appropriately at the suggestion of individual data bases.
Methods
Articles not written in English, conference papers and other grey literature were excluded from those finally considered. All other studies that conformed to one or more of the EP search criteria and one or more of the geographic criteria were individually and independently reviewed by two researchers. These first-line reviews were compared. All studies identified by both reviewers were included. All studies identified by one, but not the other were re-reviewed individually and then together. The identified studies were then prioritized according to their relevance to the primary criteria.
Results
A total of 637 finds that met both one EP term and one or more of the geographic or program criteria were located. Of these, 206 were identified as having primary importance in that they focused directly on the areas of interest, described or evaluated either EP programmes or specific elements thereof, or were seminal to EP best practice rather than being of tangential interest. Of these 206, only three, Welch and Garland; O'Kearney et al. and Tee et al., were specific to first-episode psychosis in rural areas [26–28] and only one had any program evaluation [27]. The other two were only descriptive. Rural issues or perspectives did not figure to any significant degree in any of the meta-analyses, systematic reviews, guidelines or protocols.
Welch and Garland described the beginning of implementation of an EP service in a rural area in NSW, Australia with a population of approximately 185 000 [26]. The Southern Area First Episode (SAFE) Programme adopted a mainstreamed approach to EP intervention in the light of the guiding principles of promotion, prevention and partnerships from the 2nd National Mental Health Plan [49]. It describes how locally based mental health clinicians developed expertise in EP and built liaisons with primary care, community and education services in order to maximize the early identification of people at risk of, or developing an early psychosis. The programme concentrated on issues of identification, referral, coordination of services, engagement of families and clients, assessment and treatment protocols. It was actively involved in the development of continuing medical education (CME) modules and workshops for all levels of mental health and other health workers. The report did not include any clinical data, and was primarily a description of service provision and orientation.
Tee et al. reported on a Canadian project from South Fraser Area Health in British Columbia [28]. Like the Welch and Garland study, it was descriptive rather than evaluative, but was a mix of rural and urban settings. However, it was particularly concerned with bridging youth and adult mental health services and consisted of a central team (a 0.4 psychiatrist, a programme manager, an education coordinator, am intake clinician, a group therapist and two part-time psychologists for research, programme development and cognitive assessment) and a set of specialist community clinicians who provide core case management and treatment services. In its first year of operation the programme accepted 93 referrals from a total population of 590 000.
O'Kearney et al. presented an evaluation of the SAFE program [27] previously described in its developmental stage [26]. The study attempted to identify the factors that influenced the fidelity of programme delivery. A retrospective audit of all clients aged between 15 and 25 years seen by the entire mental health service in the first 2 years of SAFE's operation was conducted. A total of 225 new files were audited and 43 of these met sufficient criteria to be included in the SAFE programme. However, only one-quarter of these were actually identified as early intervention clients on initial assessment. There was considerable variation in the delivery of best-practice protocols. Some, like the medical aspects of care, ranged between 61% and 81% fidelity, but others, such as psychoeducation for clients and families, cognitive behavioural interventions or outcome measures, had only 20–33% fidelity. Much of this discrepancy was accounted for by inconsistent application of the programme in different sectors of the service. Where the programme was implemented according to its protocols the specificity and sensitivity of the assessment was high, the drop-out rate low and process evaluation encouraging. Overall, a provisional assessment diagnosis of psychosis, or suspected psychosis, was predictive of best-practice intervention, and registration in the SAFE programme was the strongest predictor of all.
The South Fraser Area [28] has a population more than threefold that of Southern Area (SAFE) [26, 27] and also has a greater urban component, but it may be concluded that the referral rates are approximately similar. It therefore appears possible for rural EP services to capture those most at risk, but treatment fidelity and outcome measurement is less researched.
It may also be noted that although EP does not figure specifically, a significant number of national policy and strategic documents recognize some of the particular needs and characteristics of rural areas [17].
The lack of any large-scale studies makes assertions difficult. However, the three studies that do concentrate on rural services have a number of common factors that have been identified elsewhere in other literature: (i) well-developed GP of family physician liaison and primary care structures [50–56]; (ii) integration of services [51, 57, 58]; (iii) single point of entry and open referral systems [50, 51, 59, 60]; (iv) partnerships with other agencies [58, 61–64]; (v) continuous programme of CME and clinical development activity [51, 65–67]; (vi) engagement of community and educational agencies, especially in raising awareness and collaboration in early identification of mental disorders generally and psychosis in particular [52, 68–71]; (vii) accessible expert consultation, including using innovative technology such as telepsychiatry [72–75]; (viii) well-distributed clinical guidelines and protocols, medication recommendations [6, 7, 76, 77]; (iv) standardized intake, assessment, rating and evaluation forms, scales and measures [78–80]; (x) process as well as outcome evaluation [80, 81]; (xi) coordination and ease of transition between youth and adult services [62, 82–86]; and (xii) working within existing structures and budgets; reorganizing staffing duties and roles rather than adding more [55, 87].
These factors may be compared to the evaluation of the best available evidence in EP generally [11]. Although Marshall and Lockwood conclude that the number of rigorous trials is small, and that only family interventions can claim to be validated by the clinical evidence [11], there is still both a compelling theoretical case and an ethical justification for early intervention. The problem is not so much a preponderance of contrary evidence as a lack of persuasive studies.
If the idea of early intervention makes sense, and the benefits to clients, families and services have a sound hypothesis, then carefully crafted research design and evaluation may begin to indicate where practice is, or where practice needs to become, evidence based [11].
Discussion
It is clear from the paucity of results from rural search criteria that the particular and specific aspects of providing EP care in rural areas have received little consideration in the published literature. Australia and Canada appear to have given the issue most prominence, not altogether surprising considering their geography and population characteristics. Others, such as the UK and New Zealand also appear to recognize rural mental health as having particular needs, although it must be recognized that the use of the terms and the issues of distance and population density in particular may not be comparable in all cases. Nevertheless, it may be asserted that overall rural mental health, and EP in particular, is underserved and underresearched [88, 89]. This parlous situation seems to be well-recognized in the wider literature, but still not yet fully addressed.
Nevertheless, the evidential landscape is not entirely barren. It may be possible to infer a number of significant aspects of research, service delivery and evaluation that require and may benefit from further and more rigorous investigation.
Although it is a small study, and lacks controls, O'Kearney et al. suggest that it is possible to develop rural programmes that have comparable specificity and sensitivity to metropolitan ones [27]. It is also arguable that better outcomes are associated with best-practice measures, and the best predictor for receiving best-practice care is to be registered with an EP programme.
Some aspects of best practice, clinical protocols or clinical guidelines may be applicable irrespective of the geographical location. A recommended medication regimen, the dosages and algorithms may be a prime example of what may be achieved. The implication for rural services is that because of the centrality of the GP as both initial assessor and continuing clinician [37, 90–93], in addition to the mental health worker relationship, clear guidelines, education and monitoring protocols are essential. Individual and family psychoeducation may similarly be possible in rural areas, whereas group activities may be less feasible due to a critical mass of clients, relatively few clients at the same appropriate stage of illness or treatment, distance between clients, therapists and clinical centres and the comparative lack of specialist clinicians [18]. The Initiative to Reduce the Impact of Schizophrenia (IRIS) Programme may be cited as a case of a primary care initiative [94], albeit in an urban area and this interface requires further investigation.
The demographic and service characteristics of rural areas may require a reorientation of approach. A more systematic approach to research and evaluation may be required. Recommendations for issues that may be specifically addressed include the following.
Early identification: unless there is a fundamental awareness of those at risk of an EP there cannot be a timely intervention. Early identification of signs, symptoms and at risk states may be a key factor in reducing the duration of untreated psychosis (DUP). The ease and reliability of these processes seems to be of the highest importance. Access: isolation, distance and thinly distributed services may make access to specialist services more problematic. Partnerships: rural services are often centered around the pivotal role of GPs. Programmes to develop awareness, assessment skills, early identification and referral mechanisms, best-practice support and protocols for the delivery of care may need to be encouraged and systematically evaluated. The community: the recognition and facilitation of social capital in rural areas, involving programmes of mental health literacy, collaboration with schools and other social services, may optimize the strengths of rural communities. It may be possible to incorporate early identification strategies into public, school and GP education initiatives. The critical mass: the lack of a critical mass in the population to sustain specialist services may require different funding mechanisms such as the pooling of resources across several programmes. Best practice: there is no rigorous body of evidence to indicate best practice in the delivery of early psychosis services in rural areas, their needs and characteristics. Clinical guidelines and protocols may need to address this shortcoming in future revisions and editions.
In addition some specific initiatives may be suggested to build on this study. In particular to: (i) identify in a vigorous and thorough manner the issues facing rural areas as they attempt to implement early psychosis programmes; (ii) develop multi-site projects involving a number of rural areas that may be able to work with populations and samples large enough and methodologies with sufficient rigor to give greater statistical reliability than is currently available (pertinent measures may include referral rates, length of DUP, hospitalization rates, lengths of stay in service and clinical outcomes); (iii) review the grey literature concerning EP in rural areas; (iv) conduct a review of studies in languages other than English; (v) recognize the heterogeneity of rural populations, and interrogate the distinctiveness of hard-to-reach groups that may include transient, traveling and seasonal workers; (vi) compare and contrast the level of mental health literacy and awareness, particularly concerning EP in programmes incorporating a social capacity model for early identification (target populations may include GPs, school counsellors, community services, other primary health care providers); and (vii) consider the implications of significant indigenous populations in countries such as Australia, Canada, New Zealand, South Africa and the USA (not to mention the non-English speaking world).
The are significant design challenges for teams and programs in rural areas, and the dilemma of providing expert services for low-prevalence disorders is acute (although not entirely confined to EP) [46, 95, 96]. Some of these are concerned with stretched resources, especially time, money and the recruitment and retention of trained personnel [97]. This can result in programmes operating within programmes, within programmes with a consequent dilution of therapeutic focus and intensity at each stage. It can also adversely affect the staffing of rural services: fewer resources put more pressure on staff, more pressure on staff makes retention and recruitment more difficult, retention and recruitment difficulties make for fewer resources and so the vicious cycle continues [98]. Small urban services, operating on a hub-and-spoke model in which an urban centre can offer a support service to a rural hinterland, may also face similar problems, but with systematically applied and evaluated programmes can deliver services with outcomes comparable to larger centres [99]. Sometimes it appears that the size of the service is no indicator of its efficient or effective implementation of an EP service and better measures may be its focus, process evaluation, retention of clients within a service and social capacity [97].
It has been noted that there is considerable variation in the types, levels and intensity of the services delivered in rural areas [97]. However, evidence-based principles seem equally applicable, no matter what the circumstance. Jensen and Boyden [33] detail a series of 15 interdisciplinary health training programmes all informed by concepts of social capacity, with none relying on extensive infrastructure.
Furthermore, while the education of practitioners or the widespread distribution of clinical guidelines or protocols is necessary, it is not sufficient [100]. Sometimes this may simply add to the burden of an already overstretched service [101]. Knowledge itself may inform better practice, but an alternative view of service provision, a conceptual reorientation, may be required.
There are qualitative as well as quantitative factors that affect the implementation of services [102]. Aspects of leadership, staff attitudes and most importantly an understanding of local culture and context are cited as being the practitioners’ own priorities. The levels of trust and intimacy arising from these relationships significantly effect the care provided [103]. The effectiveness of local practitioners compared with visiting experts is argued following a study in rural Tasmania [96]. The active utilization of local resources seems to have therapeutic advantages over the intermittent expert.
Although the evidence is sparse, and this is reflected throughout the literature concerning mental health in rural areas, there does seem to be good reason for hope that a reorientation of service provision towards an integrated primary health approach that utilizes the strengths of the social capacity of rural areas and embeds an early identification ethos within all its partners, may produce effective and efficient care.
Limitations of the study
The review of the literature, while attempting to be comprehensive, has a number of shortcomings that should be acknowledged. It considered only the literature published in peer-reviewed journals. This excludes any significant studies or reports that may be found in the grey literature, such as unpublished theses, health service reports and audits, unpublished conference presentations or studies that were not peer reviewed. While this is a limitation of the present study, it is also a criticism that may be levelled at the methodology per se. However, the inclusion of lower levels of evidence in the report may offset this to some extent. Second, no studies in languages other than English were considered. This decision may have excluded significant studies from countries with considerable rural populations or where pertinent work may be being conducted. Countries in Central and South America such as Mexico, Brazil and Argentina come to mind, as do several European countries, including France, Germany, Spain and Denmark. Some, for example France, may be somewhat in advance of the English-speaking world in advocating for ‘breaking the compartmentalization in the delivery of psychiatric and mental health care’ and involving primary care systems [104]. However, without further research this question cannot be answered at this point.
It is not within the scope of the present review to discuss in detail all of the 206 articles that were identified as having some relevance to the study questions. Space alone dictates this. However, a full bibliography and search term results are available on request.
Conclusion
In conclusion, it must be noted that, as Marshall and Lockwood caution [11], EP is a very rapidly expanding topic of research, and there are constantly new reports and studies. There have been many great strides and substantial gains in the design, implementation and evaluation of early intervention programmes in the last decade. A significant number of national plans or guides have been very supportive, for example The Third National Mental Health Plan from Australia [105] and National Service Framework Policy Implementation Guide from the UK [106]. However, there remains a discrepancy and shortfall in the quantity, quality and intensity of research pertaining to rural areas. There are design challenges inherent in providing services in rural areas that are not solely concerned with EP, but which are exemplified by it. Nevertheless, some areas of inquiry do provide encouragement and hope, in particular: the primary care approach, the early identification of those at risk through community partners, developed community capacity-building and the utilization of the hub-and-spoke model for interventions. Despite the disappointing return the systematic search of the published literature provides significant evidence of absence rather than relying on any unsubstantiated assertion, and this may serve as a point of departure for the next stage of focused research and service development.
Footnotes
Acknowledgements
The present study was made possible through funding from a grant from the Faculty of Nursing, University of Alberta, Edmonton, Alberta, Canada.