
Abstract
Professionals tend to favour a relatively brief set of therapeutic options in managing depressive disorders, including drugs, psychotherapy and counselling. Many reports inform us, however, that patients and those in the community do not necessarily share such prioritizing, with self-help and complementary therapies both commonly used and highly rated. In one representative regional study, patients routinely attending their general practitioner were asked to consider two depressogenic stimuli and then complete a checklist of 51 coping responses [1]. When ranked by perceived effectiveness, distraction strategies were perceived as most effective, engaging in physical exercise or sport rated 19th, visiting a doctor or other professional person rated 42nd, and taking medication rated as the third least effective strategy. In essence, subjects rated personal coping and self-help strategies as more effective than seeking professional help or accepting professionally recommended antidepressant drugs. In another regional study, Jorm et al. undertook a postal survey of more than 6000 individuals, quantified state depression levels and asked individuals to rate ‘treatments and activities’ used to cope with any depression [2]. Although seeking professional help was uncommon for those experiencing low distress levels, it increased linearly as distress levels increased. However, self-help strategies were commonly used, irrespective of the level of distress.
We report a study of a large sample of Australian individuals, with selection designed to ensure a high probability of those who had both experienced clinical depression and sought professional help. The aim was to determine – in a sample with substantive depressive experience-the judged comparative effectiveness of a range of professionally recommended strategies (i.e. antidepressant drugs and psychotherapy) and other self-help, complementary and less orthodox strategies previously suggested as commonly used by those with depression.
Method
Strategy
People accessing the Black Dog Institute website were invited (if they had received treatment for a lifetime episode of depression) to participate in an anonymous online survey. Participants were informed that the principal purpose of the study was to examine the relationship between personality styles and treatment response (to be reported independently), with informed consent addressed by checking a box.
Those who elected to participate were asked to respond to demographic questions, provide details of their depressive episodes and complete a personality questionnaire. They were asked whether they had consulted differing professionals for a depressive episode (e.g. general practitioner, psychiatrist, psychologist), and whether they had ever received any of a set of different treatments for depression, including antidepressants, psychological therapies, electroconvulsive therapy, and whether they had trialled other more alternative strategies. For each strategy trialled, they were required to rate its effectiveness on a 4-point scale (from ‘very effective’ to ‘not effective at all’) or, if relevant, record that the strategies had been ceased before its effectiveness could be judged.
Sample
We received 3486 consecutive fully completed returns before removing the questionnaire from the website. Because our current objective was to obtain regional data from those who were likely to have experienced clinical depression, we limit analyses to a subset of 2692 subjects who met four criteria: ≥18 years; lived in Australia; completing the survey for the first time; and reporting a depressive episode lasting ≥2 weeks or longer. The subjects’ mean age was 40.0 years (SD = 12.0 years; range = 18–77 years), 70.8% were female, 52.5% were married or living with a partner, while 45.9% were employed full-time and a further 20.1% were employed part-time.
Data analyses
Statistical analyses were conducted using the statistical software package SPSS version 13.
Results
Onset and duration of depression
The reported mean age of the respondents’ first depressive episode was 23.4 years (SD = 11.4 years), while the mean duration of the longest episode of depression experienced was 38.2 weeks (SD = 73.9 weeks).
Treatments trialled
In terms of professionals ever consulted for a depressive episode, 83.1% of respondents indicated that they had consulted a general practitioner; 57.9% a psychologist; 51.6% a psychiatrist (88.4% had consulted one or more of these three groups), while one or more ‘other professionals’ had been consulted by 34.8% of the sample. Psychiatrists, psychologists or general practitioners had been consulted by the majority, and all but 11.6% had consulted at least one of those professional groups for a depressive episode. Further, psychotherapy or counselling had been received by 78.3%, while a majority (73.6%) had received one or more antidepressant medications. Tables 1–3 present the frequencies of respondent-rated effectiveness judgements for antidepressants, psychological therapies and other techniques that had been trialled by at least 100 respondents, which limited the tricyclic (TCA) set to four drugs only. Examining individual therapies and techniques, the most commonly trialled strategies were exercise (79.5%), relaxation (71.0%), a selective serotonin re-uptake inhibitor (SSRI; 62.9%), counselling (65.5%), yoga/meditation (45.1%), Cognitive behaviour therapy (CBT; 45.4%), ‘other psychotherapy’ (43.9%) and massage (39.3%).
Response to antidepressant medications: frequencies
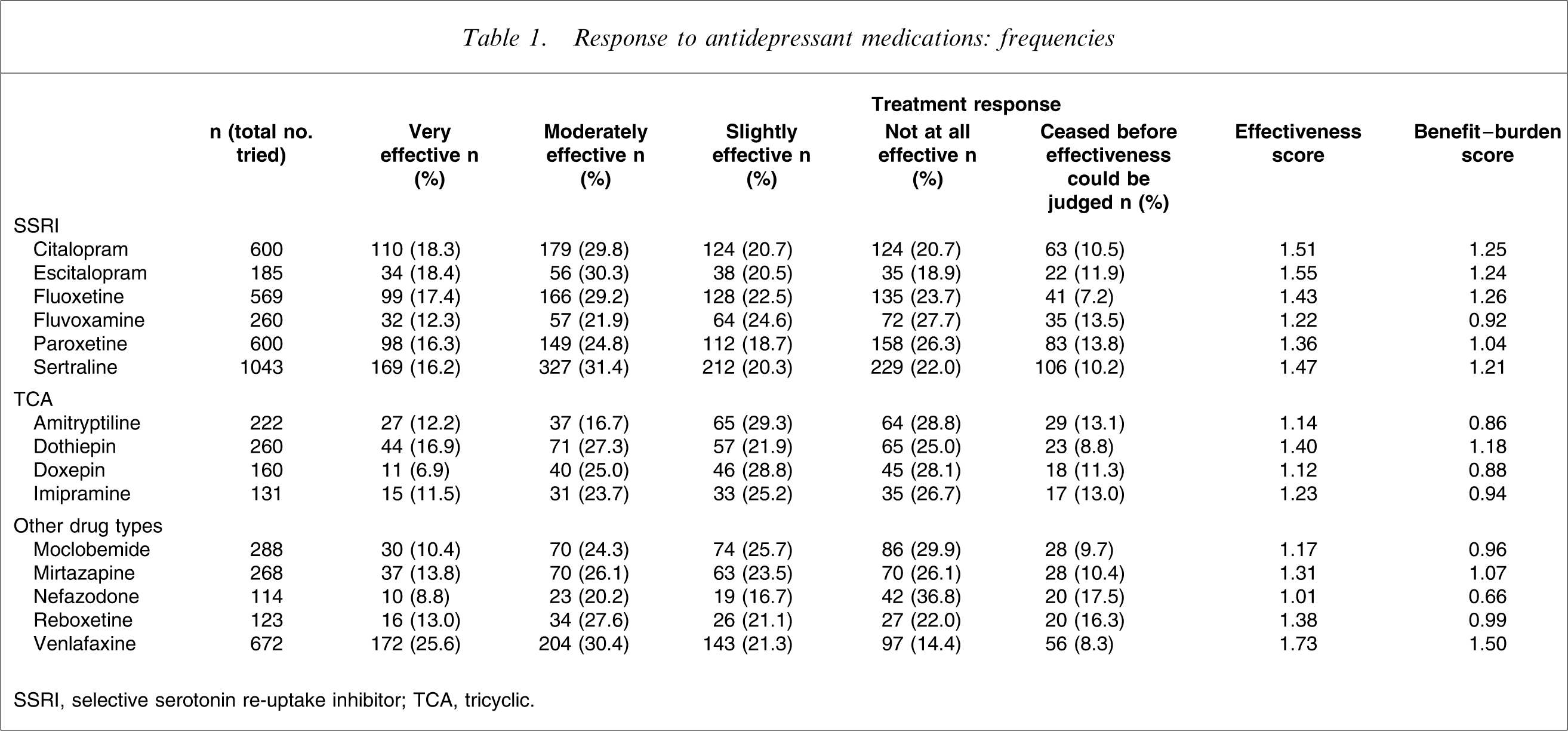
SSRI, selective serotonin re-uptake inhibitor; TCA, tricyclic
Response to psychological therapies: frequencies
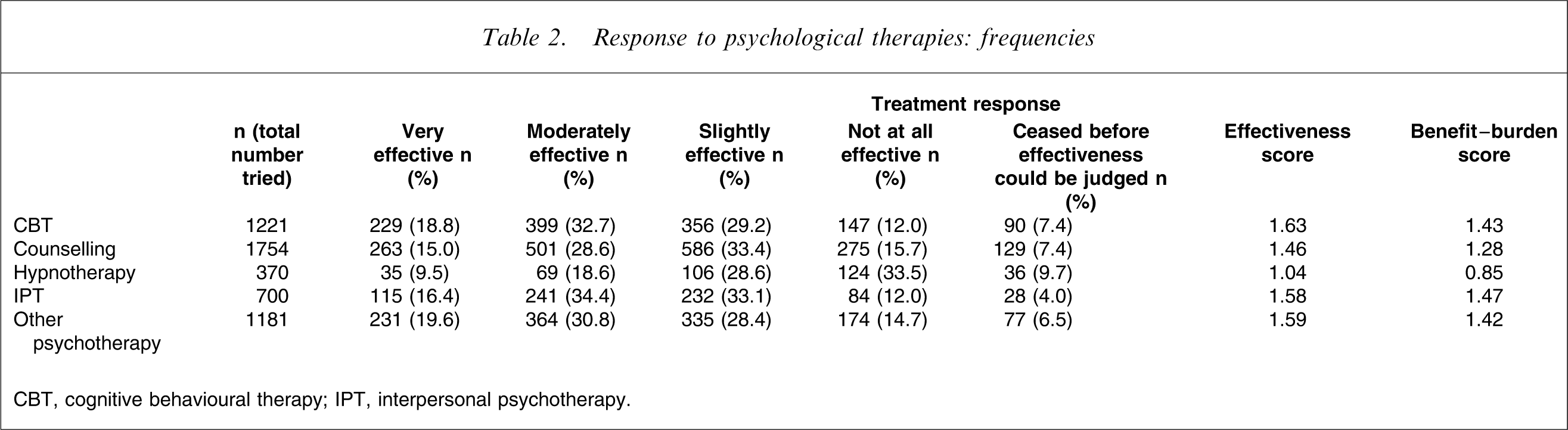
CBT, cognitive behavioural therapy; IPT, interpersonal psychotherapy.
Response to other therapies and techniques: frequencies
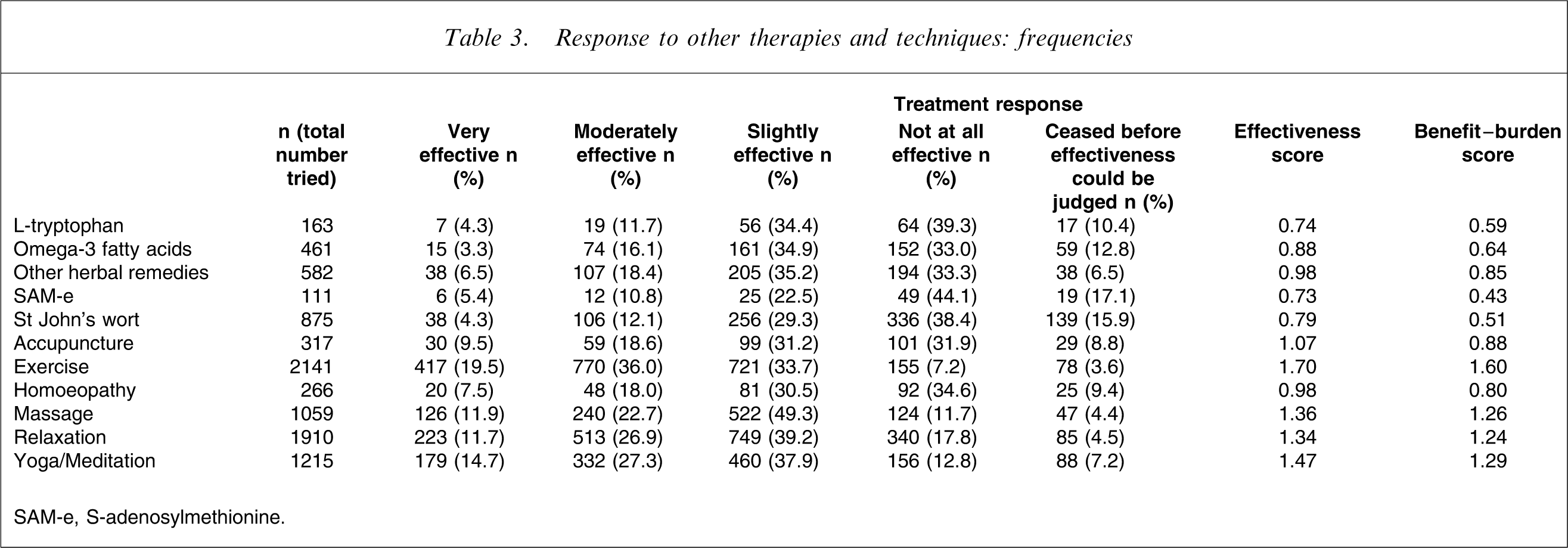
SAM-e, S-adenosylmethionine.
Quantitative analyses
We created treatment effectiveness scores by summing scores for each treatment (very effective, 3; moderately effective, 2; slightly effective, 1; not effective, 0), and dividing that score by the number of respondents who had tried the treatment (but not including those who ceased that treatment before its effectiveness could be judged). We did not contrast the differing treatments statistically because the large samples might suggest that one treatment was necessarily superior to another, and instead offer broad interpretations. Table 1 data (focusing on antidepressant drugs) suggest several differences. The TCA drugs, with the exception of dothiepin, tended to be judged as less effective than the SSRI drugs. Within the SSRI class, individual SSRI drugs appeared generally comparable, apart from fluvoxamine, which generated the lowest effectiveness score. In the ‘other’ drug category, venlafaxine scored as distinctly more effective than other drugs within this grouping (and as more effective than TCA and SSRI class drugs), while moclobemide and nefazodone were less effective than other group members and the SSRI.
Assuming that ceasing a drug before its effectiveness could be judged might be influenced by the negative impact of the drug (e.g. side-effects, lack of perceived benefit) – although patient factors such as non-compliance would also contribute – we also calculated a benefit–burden score (here, a −1 score was given to those who ceased a strategy before its effectiveness could be truly judged, preserving the +3, +2 and +1 for those who had tried a strategy and judged it as having some effectiveness, and dividing total scores by the number having tried that drug). Table 1 data suggest a similar (but not identical) rank order to the differing drug treatments for those benefit–burden calculations.
In Table 2 we undertook similar analyses for counselling, hypnotherapy and several psychotherapies. CBT, interpersonal psychotherapy (IPT) and the ‘other psychotherapy’ groupings returned comparable effectiveness and benefit–burden scores, rated as superior to counselling, which, in turn, rated as superior to hypnotherapy.
In Table 3 we report similar analyses for a range of ‘other’ treatments that are commonly trialled by patients with depression. Exercise had the highest effectiveness and benefit–burden scores, followed by yoga/meditation, relaxation and massage. Acupuncture and homoeopathy returned moderate ranking scores, while the various drugs, herbal preparations and omega 3 fatty acids returned the lowest ratings.
Because we used the same effectiveness quantification strategy across all modalities, comparison of the differing strategies identified four antidepressant medications, four talking therapies (CBT, IPT, ‘other psychotherapy’, counselling) as well as exercise and yoga/meditation in the 10 highest rating strategies.
Discussion
This study sought to determine from those who were likely to have experienced clinical depression, how effective they judged a number of antidepressant treatments and strategies. While we did not formally establish whether subjects had met lifetime operational criteria for major depression, confidence is advanced by the majority having consulted a professional, receiving psychotherapy or counselling, receiving one or more psychotropic drugs, and reporting a mean duration of 38 weeks for their longest depressive episode.
Mental health literacy studies have informed us about community members’ views about the likely effectiveness of varying antidepressant strategies. For example, Jorm et al. had community respondents to a postal survey read a vignette of major depression, and rate the likely helpfulness of a range of interventions and coping strategies [3]. At baseline, highly rating interventions were counselling, physical activity and relaxation, while consulting a professional, taking an antidepressant drug or receiving psychotherapy rated as only likely to be moderately helpful. At follow up of the initially symptomatic individuals, actual consulting of a professional or receiving an antidepressant drug or psychotherapy was less likely than using simple self-help strategies.
Most such surveys comprise general community subjects or those with mild expressions of depression. But, and the question posed by our study design, do such preferences hold up in those who are likely to have actually experienced clinical depression and trialled differing strategies? Further, to what extent are differing strategies tried in clinical groups? Our study established that antidepressant drug, psychotherapy or counselling, as well as exercise, were all relatively ubiquitous strategies.
Synthesizing comparative effectiveness judgements from such a study is clearly problematic. On our benefit–burden measure, exercise was judged as the most beneficial strategy, and superior to all drugs and all psychotherapies. While exercise has been recently evaluated and supported in an intriguing efficacy study [4], it would be facile, however, to take such rankings at face value. The therapies and strategies may have been primary, secondary or adjunctive therapies, so that treatment sequencing may differ across strategies. Clearly, many are practitioner-delivered and others self-help strategies. Some may be targeted at depression while others may more address the consequences of depression and associated conditions. Each may invite differing therapeutic expectations and end-points. Equally importantly, a treatment (e.g. a tricyclic antidepressant) that might be highly specifically effective for a minority depressive condition (e.g. melancholia) might, if prescribed beyond its therapeutic appropriateness or prescribed at low dose, have its true effectiveness compromised and so rank comparatively poorly. To limit such interpretive risks, comparative judgements are best limited to comparable therapeutic modalities. For example, examining antidepressant drugs, venlafaxine rated above the SSRI, one SSRI (fluvoxamine) appeared to rate disproportionately low in the SSRI class, the TCA dothiepin appeared somewhat superior to the other TCA and, in the ‘other drug’ class, moclobemide and nefazodone returned low ratings. In the ‘psychological therapies’ class, all three optional psychotherapies (i.e. CBT, IPT, ‘other psychotherapy’) rated comparably and as somewhat superior to counselling. In the ‘other therapies’ class, exercise, yoga/meditation, relaxation and massage rated higher than acupuncture, homoeopathy and other herbal remedies. The drugs listed in that class (i.e. St John's wort, L-tryptohan, S-adenosylmethionine (SAM-e), omega-3 fatty acids) received both low effectiveness and benefit–burden scores compared to virtually all formal antidepressant drugs, and that finding may well reflect a true clinical effectiveness differential.
As reviewed earlier, the public do not necessarily share the views of professionals about effective therapies for depression. The present study, obtaining the judgements of those who had clearly had significant mood disorders as well as extensive formal treatments, extends earlier mental health literacy studies to suggest that a very wide set of strategies are used by clinically depressed individuals. The implications to such comparative judgements are less clear. Just as it would strain credulity for a practitioner to recommend exercise instead of a physical treatment for a patient with a bipolar depressive episode, it would also be facile for practitioners to merely recommend strategies identified here as being of distinct benefit. Thus, we suggest that there are few direct therapeutic implications to the findings other than intra-class comparisons of the antidepressant drugs and of the psychotherapies. However, it might be distinctly useful to study the highly rated ‘other’ strategies more closely, given their positive reception, relatively low cost and limited side-effect profile. Rather than merely consider their efficacy, it might be more important to determine the circumstances (e.g. the assumptive world or preferences of the patient, characteristics of the depressive disorder, the extent to which they are primary or augmenting, or advance pluralism) that are associated with their judged utility.
Footnotes
Acknowledgements
We thank the NHMRC (Program Grant 223708), NSW Department of Health, and Pfizer International for funding support, and respondents to the survey.