
Abstract
Study Design
Prospective follow-up design.
Objective
Ureteral injury is a recognized complication following gynecologic surgery and can result in hydronephrosis. Anterior lumbar surgery includes procedures like anterior lumbar interbody fusion (ALIF) and total disk replacement (TDR). Anterior approaches to the spine require mobilization of the great vessels and visceral organs. The vascular supply to the ureter arising from the iliac arteries may be compromised during midline retraction of the ureter, which could theoretically lead to ureter ischemia and stricture with subsequent hydronephrosis formation.
Methods
Potential candidates with previous ALIF or TDR via anterior retroperitoneal access between January 2008 and March 2012 were chosen from those operated on by a single surgeon in a university hospital setting (n = 85). Renal ultrasound evaluation of hydronephrosis was performed on all participants. Simple descriptive and inferential statistics were used to generate results.
Results
A total of 37 voluntary participants were recruited (23 male, 14 female subjects; average age 51.8 years). The prevalence of hydronephrosis in our population was 0.0% (95% confidence interval 0 to 8.1%).
Conclusions
Retraction of the ureter across the midline in ALIF and TDR does not result in an increase in hydronephrosis and appears to be a safe surgical technique.
Keywords
Study Rationale and Context
It is documented in the literature that ureteric injury is a complication following gynecologic procedures. 1 , 2 , 3 , 4 , 5 , 6 Untreated ureteral injury can lead to acute kidney injury and hydronephrosis, with long-term consequences.
With this fact is mind, it is plausible to suggest that other surgery involving ureter mobilization can lead to hydronephrosis.
Objective/Aim or Clinical Question
This study is the first of its kind looking at whether ureteric injury as measured by hydronephrosis is a complication following anterior lumbar interbody fusion (ALIF) or total disk replacement (TDR).
Methods
Study Design
Prospective follow-up design.
Objective/Aim
To determine the frequency of hydronephrosis following ALIF or lumbar TDR procedures.
Inclusion Criteria
Over 18 years of age
Single-level anterior lumbar spinal surgery at least 12 months and no longer than 5 years previously
Exclusion Criteria
Multiple abdominal surgeries prior to spinal surgery
Known structural anomalies of the kidney or ureter
Previous renal complication such as strictures or hydronephrosis
Patient Population and Intervention
Patients who had ALIF or TDR for symptomatic disk degeneration via an anterior retroperitoneal approach conducted by a single team between January 2008 and March 2012 were invited to participate. All patients had normal kidney function with no evidence of renal disease prior to ALIF or TDR.
The participants underwent renal ultrasound. Ultrasound is a well-recognized sensitive and specific test for detecting hydronephrosis. 7 The scan was conducted by a single consultant radiologist targeting the kidney on the side of the retroperitoneal approach. If it was not clear which side this kidney was, both kidneys were scanned. If hydronephrosis was detected on a single kidney, a scan of the second kidney was conducted. If bilateral hydronephrosis was present, the patient was advised to contact his or her general practitioner to conduct kidney function tests and be referred to an urologist.
Outcomes
Hydronephrosis was classified as not present, mild, moderate, or severe. Mild hydronephrosis was defined as enlargement of the calices with preservation of the renal papillae; moderate hydronephrosis, as rounding of the calices with obliteration of renal papillae; severe hydronephrosis, as calyx ballooning with cortical thinning. 8 , 9
Analysis
The statistical package SPSS (IBM, Armonk, New York, United States) was used for analysis and management of the data set.
Simple descriptive statistics were used to generate results. Categorical data was described using frequency and percentages. The prevalence of hydronephrosis was calculated by dividing the number of patients with hydronephrosis by the number of patients receiving ultrasound. The “rule of three” was used to estimate the upper bound of the 95% confidence interval. 10
Results
Patient Characteristics
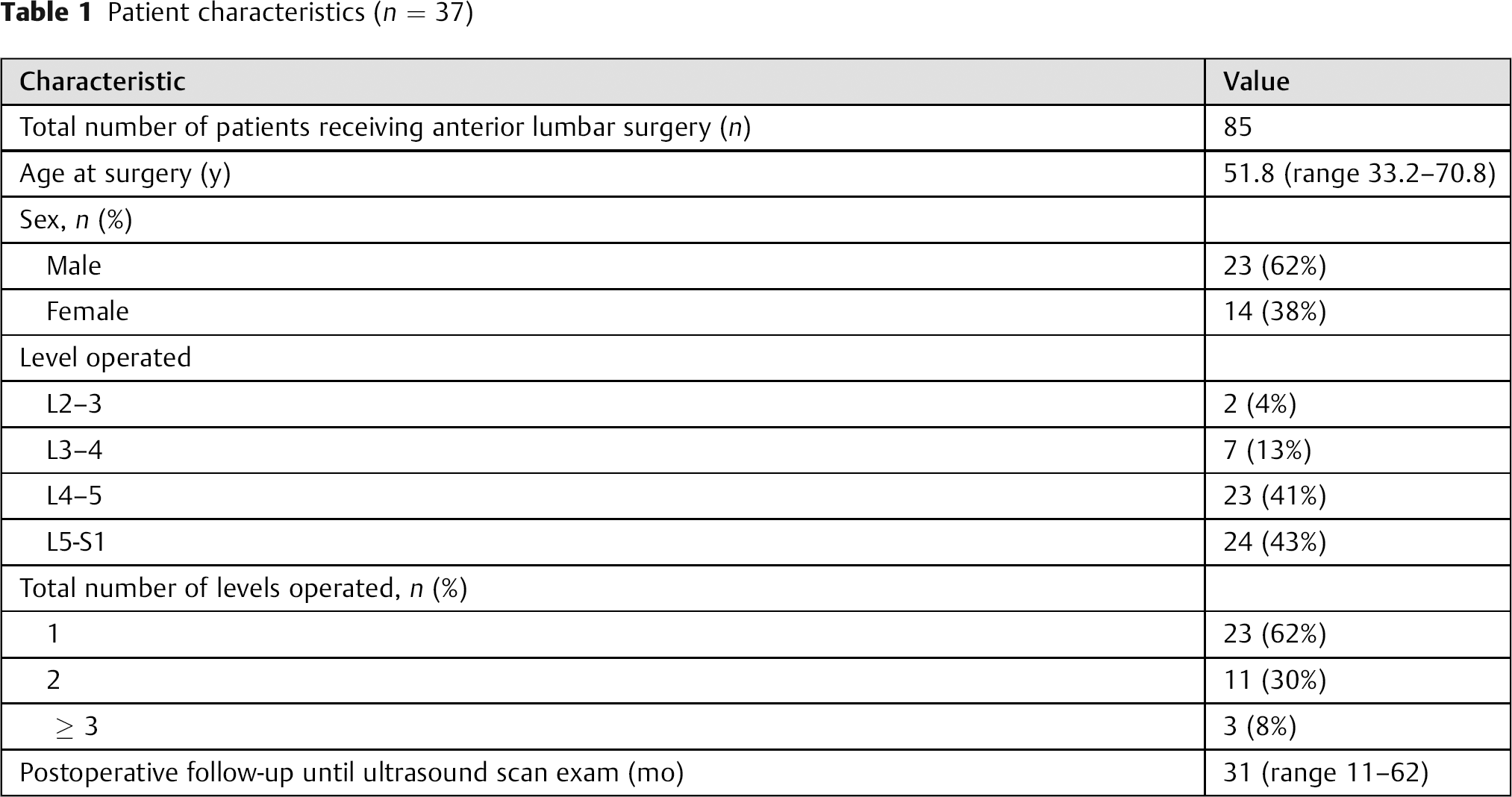
During the study period, 85 patients received anterior lumbar surgery (ALIF, n = 67; TDR, n = 18). Of these patients, 37 returned for evaluation (Table 1;
Patient characteristics (n = 37)
Outcome Results
All 44 kidneys were successfully scanned (Fig. 1). Among these, renal length and parenchymal thickness measurements were available in 36. The average renal length in these participants was 11.08 cm (range 9 to 13) The average parenchymal thickness was 1.7 cm (range 1.1 to 2.4). All 44 kidneys were successfully scanned. Hydronephrosis was not detected in any of the participants. The prevalence of hydronephrosis in our population was 0.0% (95% confidence interval 0 to 8.1%).
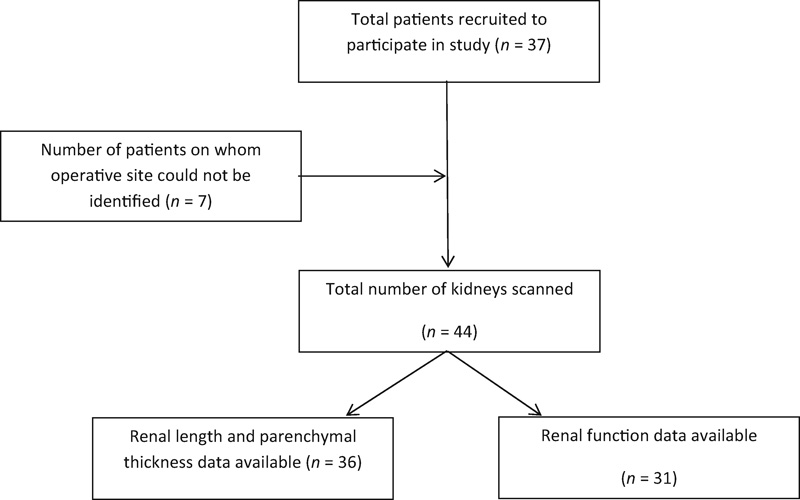
Patient sample and selection.
Discussion
As far as the authors are aware, this study is the first of its kind examining hydronephrosis as a potential complication in anterior spine surgery.
Ureter injury has an incidence between 0.26 and 30% following gynecologic procedures. 6 Untreated ureteral injury can lead to acute kidney injury and hydronephrosis. 1 , 2 , 3 , 4 , 5 , 6 It is important to counsel patients regarding this risk.
It is plausible to suggest that other surgeries that involve mobilization of the ureter can have similar complications, including anterior lumbar spinal surgery in which the ureter is mobilized medially to gain access to the spine.
The ureter can broadly be divided into three sections; the blood supply differs to each section (Fig. 2). The ureter has extensive anastomoses above and below from the gonadal, vesical, and renal vessels. 11 , 12 , 13 Medial mobilization of the ureter across the midline stretches this supply. Direct injury of the ureter, however, is rare. 14
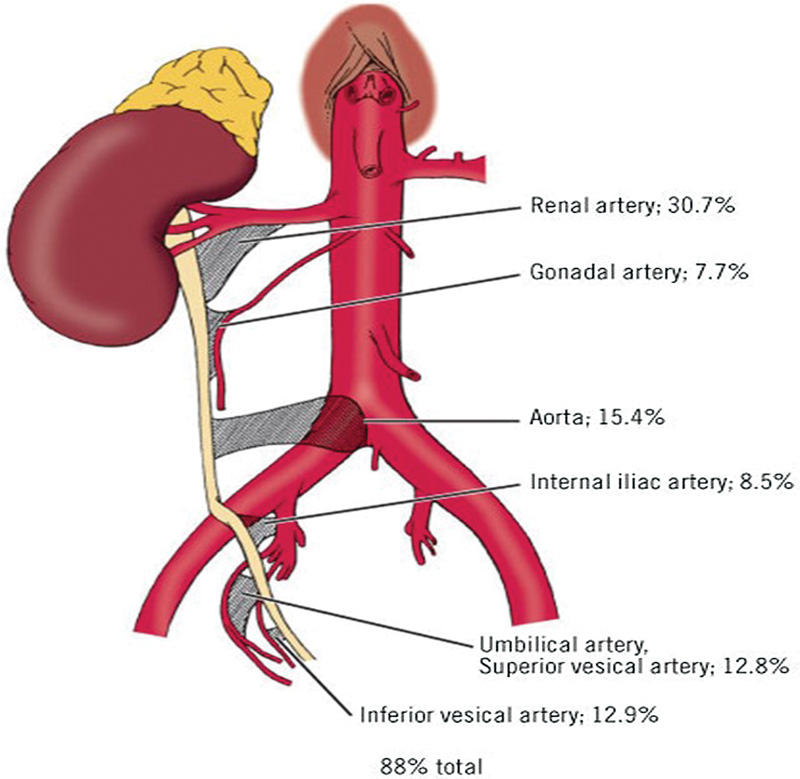
Vascular supply of the ureter with percentage contribution from important vessels.
Our findings suggest that the ureter tolerates retraction at the level of the lumbar spine. The vascular supply is not found at the level of retraction (L4–S1) but distal to this location.
There are several limitations to our study. The sample size is small and therefore hydronephrosis as a complication of spinal surgery cannot be excluded entirely. However, we have attempted to estimate the upper bound of the confidence interval using the rule of three, which gives an upper bound of 8%, thereby still having a low incidence compared with that reported in gynecologic procedures, as previously mentioned. 6 We appreciate that given the potentially low rate of complication of ureteral injury in gynecologic surgery (as little as 0.26%), our cohort may be too small to have had a ureteral complication. Furthermore, exposure for gynecologic surgery in terms of mobilizing the uterine artery in relation to the ureter may predispose to a higher rate of injury than that in accessing the spine. Out of our potential pool of participants, only 44% underwent ultrasound examination. It is possible that those who did not undergo ultrasound may be more or less likely to have hydronephrosis.
Summary and Conclusion
There are clear mechanisms to cause hydronephrosis as a potential complication after ALIF and TDR. These are primarily due to retraction and pressure on the ureter during mobilization. In our study, hydronephrosis was not detected in any participants. We conclude that hydronephrosis may not be a frequently recognized long-term complication after anterior lumbar surgery.
Ethical Approval
Obtained by Nottingham Research and Ethics Committee.
Disclosures
Ruth M. Parks, none
Eyal Behrbalk, none
Syed Mosharraf, none
Roger M. Müller, Consulting fee/honorarium: AOSpine International
Bronek M. Boszczyk, Fellowship support: Synthes
Funding
Thanks to Nottingham University Hospitals NHS Trust.
Our Evidence-Based Spine-Care Journal–Global Spine Journal reviewers commend Parks and her coauthors on a good study idea. The authors retrospectively reviewed 85 patients and were able to follow up on 37 patients with renal ultrasounds to determine if there was hydronephrosis. They scanned 44 kidneys and found no evidence of hydronephrosis. The conclusion is that the risk of ureteral injury from retraction is lower than in gynecologic surgery, which has an incidence of 0.26 to 30%. These conclusions most likely are true, but the methods for coming to this conclusion deserve further scrutiny. The number of patients available for follow-up is low (44%), and the number of kidneys evaluated is even lower (60% of the patients scanned, or 26% of the entire series), assuming each patient has two kidneys. Given the potentially low rate of complication of ureteral injury in gynecologic surgery (0.26%), the cohort in the spine series may be too small to have had a ureteral complication. Although not zero, ureteral injury in primary anterior retroperitoneal approach for ALIF and TDR is extremely rare in primary surgeries. The ureter is usually carefully swept to the right side along with the peritoneum. The ureter should not be significantly disturbed during exposure unless the ureter is skeletonized inappropriately during primary cases. The real importance of ureteric injury arises in revision cases where the risk of ureter injury is higher, and ureteric stenting to identify and protect the ureter has been recommended by some. The ureteric stent would then remain in situ for ∼6 weeks after surgery, when the stent is then removed with outpatient cystoscopy.
The reviewers also commented that the retroperitoneal exposure for gynecologic surgery is different from the retroperitoneal surgery in lumbar spine surgery. The ureteric blood supply has extensive anastomoses above and below from the gonadal vessels, the vesical branches of the internal iliac, and branches of the renal arteries. In gynecologic surgery, the location of the uterine artery relative to the ureter may predispose the ureter to a higher rate of injury than in ventral exposures for spine surgery, therefore comparing these surgeries may not be valid, and furthermore, this comparison may not give a good approximation of how many patients are needed in the spine cohort to accurately determine the complication rate.
That said, the reviewers endorsed publication of the article as it adds an important awareness to the potential for ureteral and kidney damage during anterior retroperitoneal surgery.