
Abstract
Study Design
Retrospective analysis of prospectively collected observational data.
Objective
To assess the safety and efficacy of anterior lumbar interbody fusion (ALIF) as a salvage option for lumbar pseudarthrosis following failed posterior lumbar fusion surgery.
Methods
From 2009 to 2013, patient outcome data was collected prospectively over 5 years from 327 patients undergoing ALIF performed by a single surgeon (R.J.M.) with 478 levels performed. Among these, there were 20 cases of failed prior posterior fusion that subsequently underwent ALIF. Visual analog score (VAS), Oswestry Disability Index (ODI), and Short Form 12-item health survey (SF-12) were measured pre- and postoperatively. The verification of fusion was determined by utilizing a fine-cut computed tomography scan at 12-month follow-up.
Results
There was a significant difference between the preoperative (7.25 ± 0.8) and postoperative (3.1 ± 2.1) VAS scores (p < 0.0001). The ODI scale also demonstrated a statistically significant reduction from preoperative (56.3 ± 16.5) and postoperative (30.4 ± 19.3) scores (p < 0.0001). The SF-12 scores were significantly improved after ALIF salvage surgery: Physical Health Composite Score (32.18 ± 5.5 versus 41.07 ± 9.67, p = 0.0003) and Mental Health Composite Score (36.62 ± 12.25 versus 50.89 ± 10.86, p = 0.0001). Overall, 19 patients (95%) achieved successful fusion.
Conclusions
Overall, our results suggest that the ALIF procedure results not only in radiographic improvements in bony fusion but in significant improvements in the patient's physical and mental experience of pain secondary to lumbar pseudarthrosis. Future multicenter registry studies and randomized controlled trials should be conducted to confirm the long-term benefit of ALIF as a salvage option for failed posterior lumbar fusion.
Introduction
Spinal fusion has evolved as a treatment modality for the management of spinal conditions that require stabilization, which include symptomatic degenerative disk disease, infection, scoliosis, traumatic injuries, and neoplasia. 1 Several techniques are available to achieve stabilization of the lumbar spine, which include the anterior lumbar interbody fusion (ALIF), posterior lumbar interbody fusion (PLIF), transforaminal lumbar interbody fusion (TLIF), direct lateral interbody fusion, posterolateral onlay (intertransverse) fusion, and facet screw or pedicle screw/rod placement. 2 In addition, minimally invasive variations of these techniques have also been developed to minimize soft tissue dissection with the intention of minimizing intraoperative blood loss and complications as well as reducing postoperative pain and subsequent hospital stay. 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10
Fusion of the affected segments is influenced by surgical technique including end plate preparation, by patient factors such as smoking and diabetes, and by the choice of bone graft, all of which are critical in influencing the degree and rate of fusion. 11 If the fusion is incomplete, there is the risk of developing a painful pseudarthrosis of which there are four types: atrophic, transverse, shingle, and complex. 12 The transverse type is the most common, 13 where there is a horizontal discontinuity despite remodeled bone. The source of pain is partly attributed to the sclerotic bone adjacent to fibrous soft tissue accompanied by microfractures of cancellous bone and motion of this segment. 12 Although difficult to diagnose, pseudarthrosis following lumbar fusion surgery is one of the most common complications, 14 and together with the chronic pain and disability that ensues, 13 , 15 , 16 is a common indication for revision surgery. 17 , 18
Despite its relatively high prevalence, there is a lack of robust clinical evidence on salvage options for lumbar pseudorthrosis. 19 A prospective study was conducted to assess the radiographic and functional outcomes of ALIF as a salvage option for pseudarthrosis following posterior lumbar fusion surgery.
Methods
Institutional Ethics Board Review approval was obtained from the South Eastern Sydney Local Health District, New South Wales Australia–Northern Sector (SESLHD-NS) ethics committee, Ref: HREC 11/183. From 2009 to 2013, patient outcome data was collected prospectively over 5 years from 327 patients undergoing ALIF performed by a single surgeon (R.J.M.) with 478 levels performed. Among these were 20 cases of failed prior posterior fusion that subsequently underwent ALIF and were retrospectively analyzed. Inclusion criteria specified patients who were at least 9 months post–posterior fusion with no evidence of infection or malignancy. Symptomatic nonunion was diagnosed with a combination of the following: movement on flexion/extension X-rays at the previous operative level, halo around the pedicle screws on fine-cut computed tomography (CT) scan, no evidence of bone integration through or around the interbody implants, and uptake on bone scan consistent with nonunion.
Clinical factors including smoking, diabetes, and worker's compensation were recorded. Clinical parameters such as the visual analog score (VAS), Oswestry Disability Index (ODI), and Short Form 12-item health survey (SF-12) were measured pre- and postoperatively. The verification of fusion was determined by utilizing a fine-cut CT scan at 12 months postoperatively, performed and agreed on by an independent neuroradiologist and a senior spine surgeon (R.J.M.). Statistical analysis using Student t test was used to analyze the clinical parameters from the outcome questionnaires.
Results
From the prospective database of ALIF procedures, 20 patients had previous failed posterior fusion (either TLIF or PLIF) and thus met the inclusion criteria of the present study. The baseline characteristics of the study population are summarized in Table 1. The patient group had revision surgery on average 17.5 months (range: 9 to 36) after the initial posterior fusion over a total of 27 lumbar spinal levels. There was an equal gender distribution with an average age of 56 years (range: 32 to 81) with 5 (25%) smokers, 3 (15%) diabetics, and 4 (20%) patients receiving workers’ compensation (Table 1). Bone grafts included the following 20 : 1 (5%) received autograft and 8 (40%) received iFactor (Cerapedics, Inc., Denver, CO, United States), 11 (55%) patients received allograft and INFUSE (Medtronic, Memphis, TN, United States), and the remainder used allograft and recombinant human bone morphogenetic protein-7 (osteogenic protein 1; Stryker, Boston, MA, United States; n = 2, 10%). There were 2 postoperative complications including 1 hernia and 1 case of postoperative hematuria. No postoperative infections occurred.
Baseline characteristics of included patients
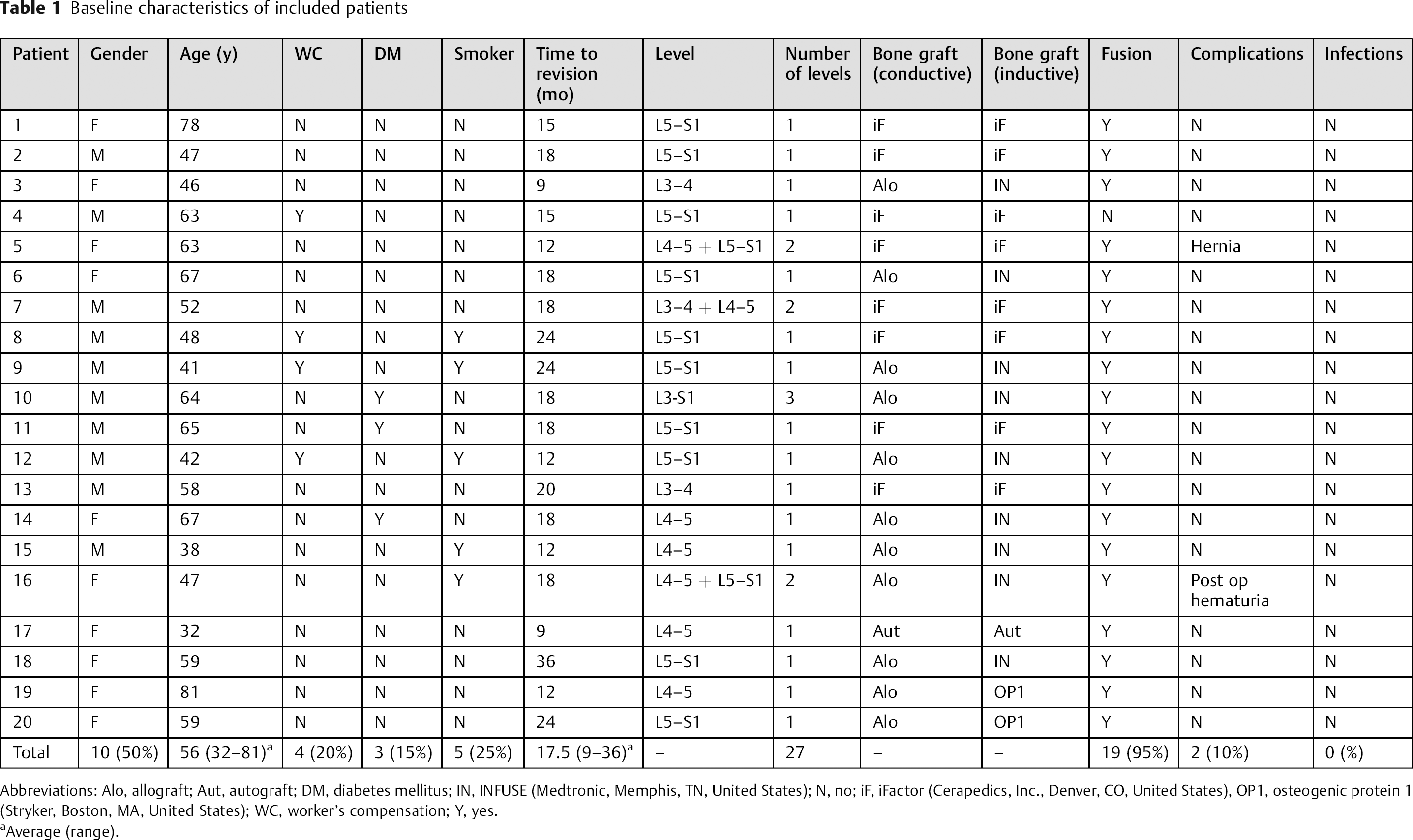
Abbreviations: Alo, allograft; Aut, autograft; DM, diabetes mellitus; IN, INFUSE (Medtronic, Memphis, TN, United States); N, no; iF, iFactor (Cerapedics, Inc., Denver, CO, United States), OP1, osteogenic protein 1 (Stryker, Boston, MA, United States); WC, worker's compensation; Y, yes.
Average (range).
Clinical outcome parameters showed overall mean improvements in the VAS (Fig. 1), ODI (Fig. 2), and SF12 (Fig. 3) scales. There was a significant difference between the preoperative (7.25 ± 0.8) and postoperative (3.1 ± 2.1) VAS scores (p < 0.0001). The ODI scale also demonstrated a statistically significant reduction from preoperative (56.3 ± 16.5) and postoperative (30.4 ± 19.3) scores (p < 0.0001). Likewise, the SF-12 scores also demonstrated statistically significant improvement after ALIF surgery: Physical Health Composite Score (32.18 ± 5.5 versus 41.07 ± 9.67, p = 0.0003) and Mental Health Composite Score (36.62 ± 12.25 versus 50.89 ± 10.86, p = 0.0001). The SF-12 total score was significantly higher after ALIF fusion (68.78 ± 12.39 versus 93.21 ± 16.16, p < 0.0001).
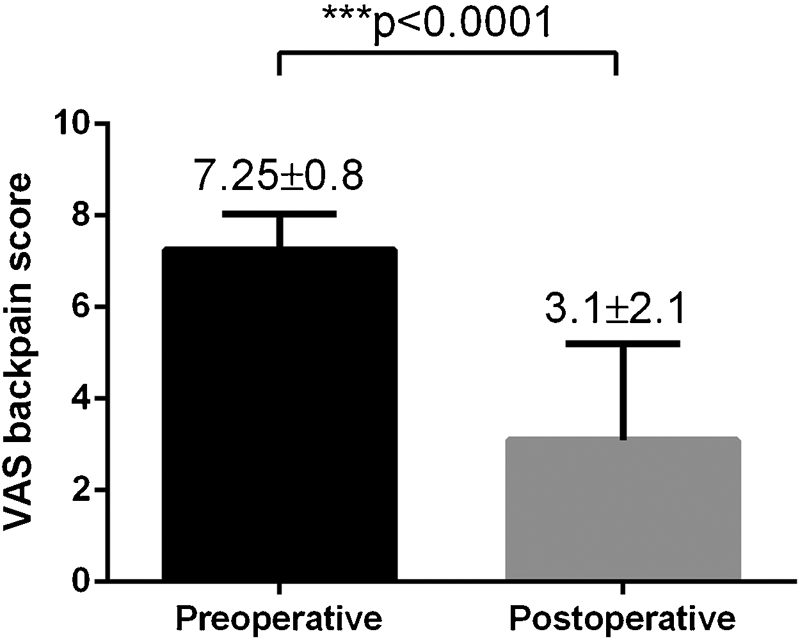
Preoperative versus postoperative visual analog score (VAS) for back pain following anterior lumbar interbody fusion revision surgery.
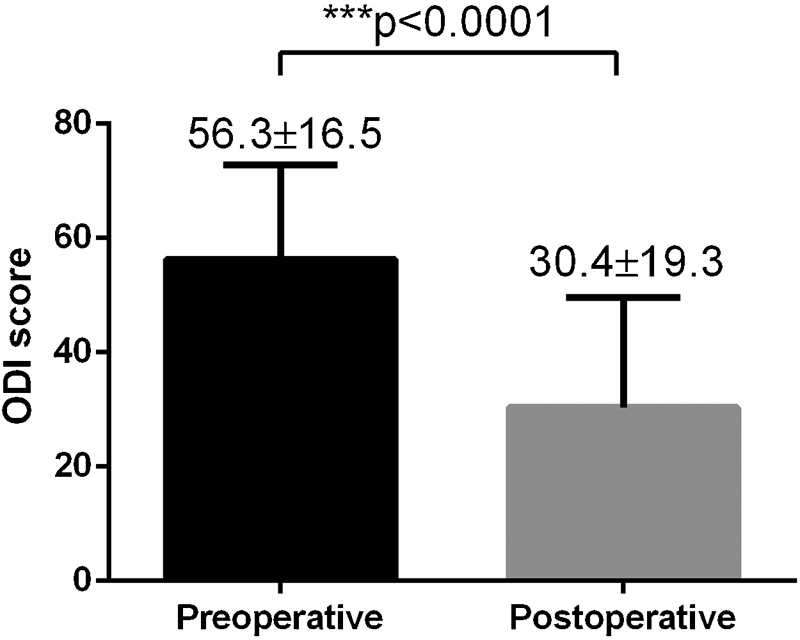
Preoperative versus postoperative Oswestry Disability Index (ODI) scores following anterior lumbar interbody fusion revision surgery.
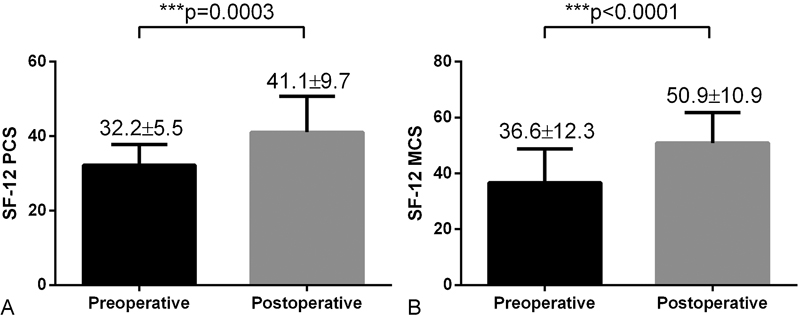
Preoperative versus postoperative Short Form 12-item health survey (SF-12) scores following anterior lumbar interbody fusion revision surgery. Significantly higher postoperative SF-12 PCS scores and MCS scores were observed postoperatively compared to preoperative scores. PCS, Physical Health Composite Score; MCS, Mental Health Composite Score.
Overall, 19 patients (95%) achieved successful fusion, as verified by at least 12-month follow-up with imaging. Radiographic improvements in bony fusions were confirmed by X-ray and CT, as demonstrated in Figs. 4,5 to 6.

Revision anterior lumbar interbody fusion performed 18 months after initial L3–L4 posterior onlay fusion. Arrow demonstrates lack of bone union across the motion segment.
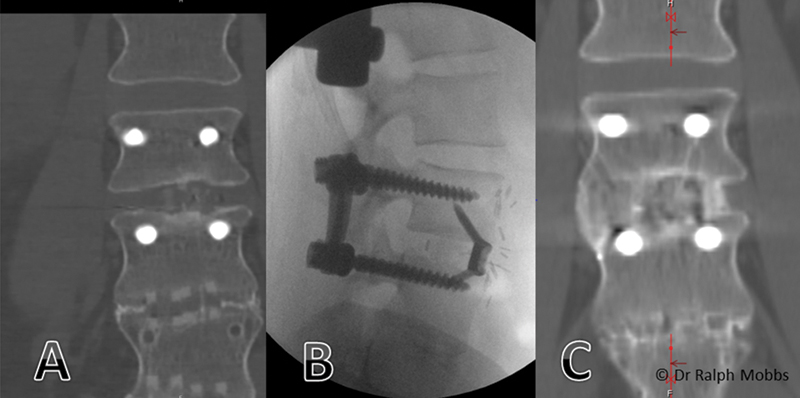
Sequence of events with nonunion. A 56-year-old woman presented with nonunion following minimally invasive transforaminal lumbar interbody fusion (TLIF) at L3–L4. (A) TLIF cage with no bone integration through implant. (B) Intraoperative X-ray demonstrating removal of TLIF cage and insertion of Synfix (Synthes Bettlach, Bettlach, Switzerland) anterior lumbar interbody fusion (ALIF). (C) Solid union of the L3–L4 motion segment can be seen at 12 months post-ALIF.

Utility of anterior lumbar interbody fusion (ALIF) for multilevel nonunion. (A) X-ray of multilevel posterior onlay fusion. (B) Intraoperative X-ray with three-level ALIF implants. (C) Computed tomography scan 12 months postoperatively with solid union through all three levels.
Discussion
The aims of revision fusion surgery include correcting any technical errors, placement of superior graft material, maximizing end plate preparation, enhancing the biological environment for fusion, and improving biomechanical environment. 15 , 16 , 21 Although the literature demonstrates that ALIF has been used to correct previously failed fusions, the overall number of cases for ALIF as an indication for pseudarthrosis is low. Other approaches for revision surgery have been demonstrated to be costly and difficult to perform with varied and unpredictable outcomes. 13
The indications for ALIF dictate its utility as a surgical option for the management of pseudarthrosis as the technique offers several advantages. First, the direct visualization and efficient access to the anterior column allows for an easier and complete diskectomy while offering better distraction to increase the neuroforaminal volume and to allow the placement of a large interbody fusion device. 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 This technique achieves higher fusion rates, 26 , 28 , 32 restores lumbar lordosis, and reduces anterior listhesis as well as coronal and sagittal balance, 22 , 23 , 29 leading to reduced pain. 25 , 33 Second, placement of the intervertebral fusion device and graft material in the anterior column redistributes the load anteriorly providing greater stability, 21 placing the graft in direct compression together with contact against a larger osseous end plate surface area with a larger vascular supply, thereby increasing the fusion potential. 29 Third, there is reduced intraoperative blood loss, reduced operating times, 22 , 25 , 26 and reduced iatrogenic trauma to the paraspinal musculature, posterior spinal nerves, and posterior bony elements. 26 , 28 , 29 The authors therefore report on the utility of ALIF as a salvage procedure for painful established pseudarthrosis following posterior lumbar fusion.
Few studies have reported outcomes for revision or repair of the failed posterior lumbar fusion. In a study by Wetzel and LaRocca, 34 9 of 12 patients developed pseudarthrosis from previous PLIF interventions. After additional procedures for repair of pseudarthrosis and repeat decompression, only 5 patients reported improved pain relief, and 7 patients were thought to have a solid fusion. No correlation was detected between solid fusion revision and relief of pain. In another study, Highhouse et al retrospectively reviewed 6 patients with failed L4–L5 PLIF interventions. 35 After 38.5 months of follow-up after lateral intertransverse process fusions for salvage of the failed fusion, five of the six cases were still radiographically fused. Another recent study suggested similar outcomes for anterior versus anteroposterior approaches for salvage of pseudarthrosis following TLIF 20 ; however, it is not clear whether these salvage procedures have directly improved radiographic and functional outcomes of these patients compared with presalvage. Strengths of the present study include being one of the few studies investigating ALIF as a salvage option for pseudarthrosis. Its sample size is relatively larger than prior case series, and its prospective design allows a better comparison between preoperative and postoperative VAS back pain, ODI, and SF-12 scores.
The present study is limited by several constraints. First, the small sample size may not provide adequate statistical power to detect complication rates. In this study, only 2 of 20 (10%) patients reported complications, which is considerably lower than the 40% complication rate (12 of 30 patients) in a previous study using posterolateral revision fusion with stand-alone metallic cages. 36 Future multicenter registry studies with large population samples will likely determine more accurately the true complication rate. Second, the study population had confounders including smoking status, diabetes, and workers’ compensation. These factors are known to affect the outcomes of both primary and revision fusion surgery. 37 , 38 Given the small cohort size of this study, 39 the effects of these confounders on the outcomes of revision ALIF surgery for nonunion could not be adequately assessed and should be further investigated in future studies. Future studies should also prospectively compare ALIF versus TLIF approaches for salvage of pseudarthrosis following posterior lumbar fusion surgery. Increased follow-up would also allow assessment of long-term radiographic and functional outcomes of ALIF revision for pseudarthrosis.
Conclusions
Overall, our results suggest that the ALIF procedure results not only in radiographic improvements in bony fusion but also in significant improvements in the patient's physical and mental experience of pain secondary to lumbar pseudarthrosis. The advantages offered by the ALIF technique are theoretically sound, and it appears to be a viable option for salvage operations and is safe in well-trained hands. Our strong recommendation is that ALIF be considered as a salvage technique for patients who present with painful pseudarthrosis following posterior lumbar fusion.
Disclosures
Ralph J. Mobbs, Royalties: Stryker Spine; Stock/stock options: Medtronic, J&J
Kevin Phan, none
Ganesha K. Thayaparan, none
Prashanth J. Rao, none
Footnotes
Note
Ralph J. Mobbs and Kevin Phan contributed equally.