
Abstract
Study Design
Randomized controlled trial.
Objective
The purpose of this study was to identify the effect of a theory-based educational intervention program on the level of knowledge and Health Belief Model (HBM) constructs among nurses in terms of the adoption of preventive behaviors.
Methods
This pretest/posttest quasi-experimental study was conducted on 100 nurses who were recruited through the multistage sampling method. The nurses were randomly assigned to intervention and control groups. The participants were evaluated before and 3 months after the educational intervention. A multidimensional questionnaire was prepared based on the theoretical structures of the HBM to collect the data. Data analysis was performed using descriptive and inferential statistics.
Results
There was no significant difference in the mean values of HBM constructs prior to the intervention between the intervention and control groups. However, after the administration of the educational program, the mean scores of knowledge and HBM constructs significantly increased in the intervention group when compared with the control group (p < 0.0001).
Conclusion
The results of the current study revealed that the educational intervention based on the HBM was effective in improving the nurses’ scores of knowledge and HBM constructs; therefore, theory-based health educational strategies are suggested as an effective alternative to traditional educational interventions.
Introduction
Low back pain (LBP) is one of the most prevalent occupational problems. It can cause lifelong physical disability and increases work absenteeism and health service use. 1 , 2 , 3 Almost 84% of the worldwide population will, at some point, experience LBP in their lifetime, making it a major public health problem. 4 , 5 Data from the United States shows that the number of physician visits due to back pain has changed a little in the past decade, 6 and the medical costs have increased substantially. 4 Due to the nature of their profession, nurses are vulnerable to the development of musculoskeletal disorders including LBP. A systematic review by Dawson et al reported that LBP was six times more prevalent among nurses when compared with other professionals, 7 and 18% of the nursing staff quit their jobs because of back pain. 8 The prevalence of LBP among nurses varies across different regions, ranging from 41 to 75% in European countries to 40 to 60% in Asian countries and 47% in the United States. 9 The prevalence of LBP among Iranian nurses has been reported to be more than 50% (annual prevalence = 59.6%, lifetime prevalence = 62%). 10 Despite the high prevalence, the underlying causes and the nature of LBP have not yet been fully understood. Many studies in various occupational settings have found a strong association between the musculoskeletal disorders and work-related risk factors11; this association has also been found among nurses. 12 In the available literature, the risk factors of LBP have either an individual or a workplace-related origin including manual patient lifting and handling, unusual immobility posture, poor workplace design and equipment, hard physical work, and poor work organization. 13 , 14
Due to the scarcity of methodologically appropriate studies, the effectiveness of educational interventions in LBP prevention remains highly controversial. 15 A Cochrane review on “back schools” provided moderate evidence with regards to the effectiveness of back schools in the workplace to decrease LBP16; however, the results of the review were not in accordance with a meta-analysis that found that the existing literature could not serve as a basis for decision making on whether or not to use back schools for the management of LBP. 17
Systematic reviews, however, have supported the beneficial effects of applying the Health Belief Model (HBM) in different health educational programs. 18 , 19 , 20 The HBM has served as a valuable tool in the field of educational evaluation to explain preventive health behaviors. It contains two main components that seek to predict preventive behaviors: threat perception and behavioral evaluation. Concerning injury prevention, threat conception comprises two main concepts: beliefs regarding susceptibility to an injury (perceived susceptibility) and beliefs concerning the anticipated severity of the consequences of an injury (perceived severity). Behavioral evaluation consists of the beliefs about the benefits of performing a recommended health behavior and the barriers to changing injury-related behaviors. Self-efficacy is the belief in one's own ability to successfully accomplish something.21 The HBM suggests that the behavior is also influenced by cues to action. Cues to action are events, people, or things that motivate people to change their behaviors (e.g., illness of a family member, media reports, mass media campaigns, advice from others, reminder postcards from a health care provider, or health warning labels on a product; Fig. 1). 22 , 23 The current study was conducted to determine the effect of an HBM-based health educational program on the knowledge level and HBM constructs among nurses in terms of the adoption of preventive behaviors of chronic LBP.
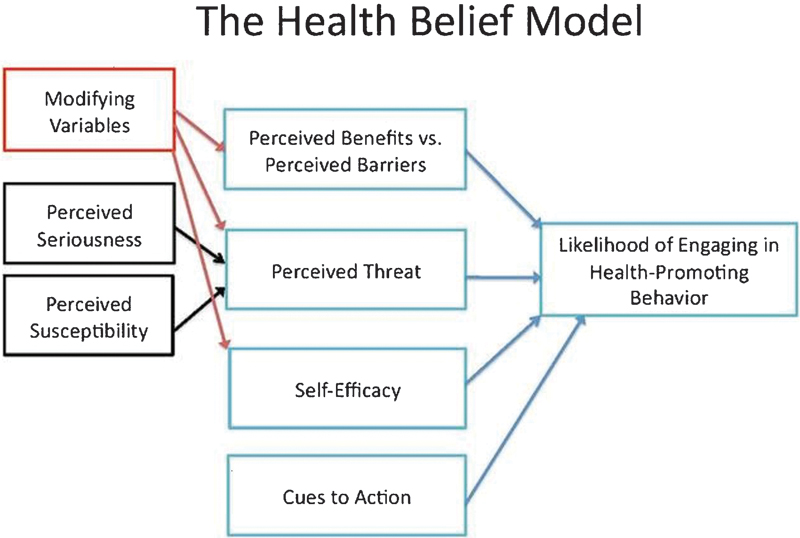
The constructs of Health Belief Model.
Materials and Methods
This pre-/posttest quasi-experimental study was conducted on nurses in teaching/nonprivate hospitals affiliated with Arak University of Medical Sciences, Iran. Written consent was obtained from all the participants prior to the start of the study. This study was approved by the Research Ethics Committee of Arak University of Medical Sciences (registration number: 91–137–5), and the study protocol was registered at the Iranian Registry of Clinical Trials (IRCT2013082814512N1). The inclusion criteria were (1) having at least 1 year of clinical experience; (2) being a full-time employee; (3) not having any medical conditions causing back pain.
All the major concepts of the HBM were used to provide a theoretical framework for the proposed study. The HBM-based educational program consisted of four 60-minute sessions presented through lecture, role-play, and discussion groups. The educational intervention sessions were provided by the research team including ergonomic experts and public health educators. The content of the educational interventions included information about chronic LBP, its risk factors and complications, the benefits of acquiring preventive behaviors, the identification of barriers in the workplace, individual and social management regarding LBP, and the prevention skills and approaches against LBP among nurses. Educational interventions involved electronic media, print media (pamphlets, posters, and brochure), and face-to-face active interactions.
Sample
The sample size was estimated using a sample size calculator. In a review of the literature, 24 a mean difference of 0.8 (standard deviation = 0.9) was found for behavioral changes to be clinically significant. The sample size of the study was calculated as 38 participants in each group with an α of 0.01 and a power of 90%. However, the number of participants assigned to each group was 50 to allow for 10% attrition.
The samples were selected in stages. In the first stage, we identified the hospitals (Amirmomenin and Amirkabir) through a simple random sampling procedure. In the second stage, Amirkabir General Hospital was selected for intervention by the manual method of drawing lots. In the third stage, the population was first segmented into mutually exclusive subgroups based on the different wards in each hospital, and then the participants were selected from each segment based on equal proportion (n = 100). Of 100 nurses included in the study, 50 were assigned to the intervention and 50 to the control group. Postintervention surveys were conducted 12 weeks after the initiation of the intervention.
Measurement Instruments
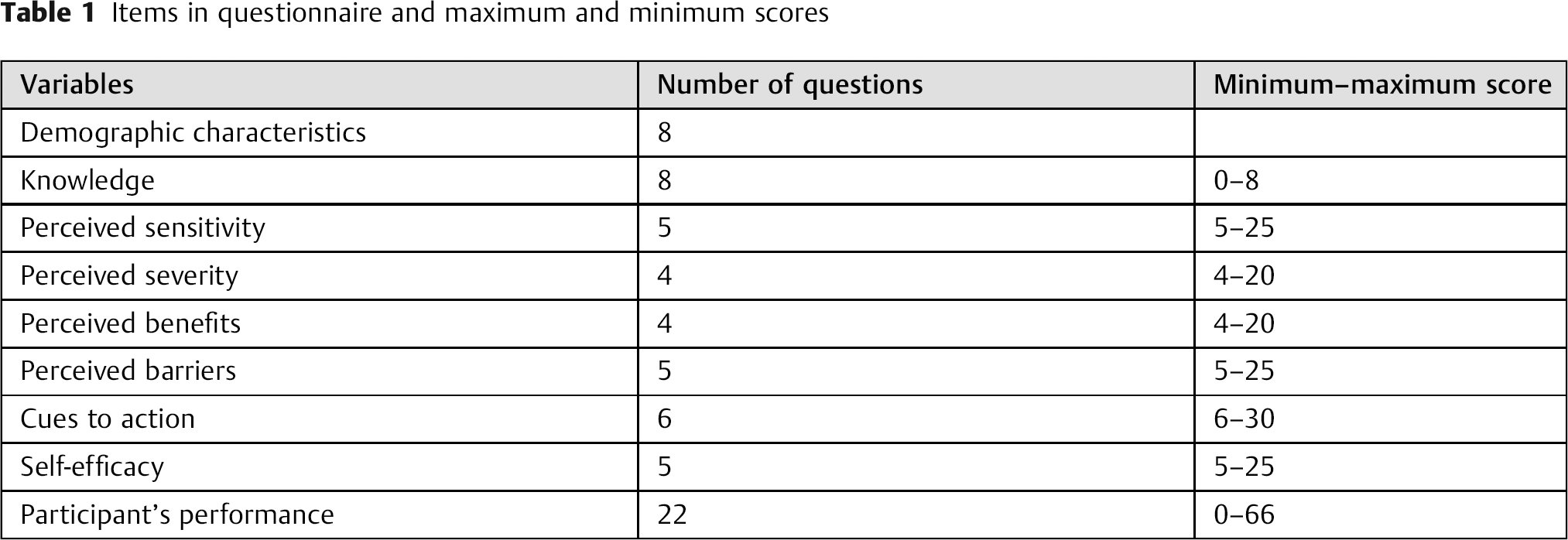
A self-reported questionnaire was used as the data collection tool. The questionnaire included four sections: (1) the demographic characteristics of the nurses, (2) the knowledge quiz, (3) the HBM constructs and self-efficacy, and (4) a checklist to assess the participants’ performance levels of adopting preventive LBP behaviors (Table 1). The content validity was evaluated using a content validity questionnaire by a panel of experts, a comprehensive review of relevant literature, 25 ,26,27 and the clarity of the wording of the questions and rating of the responses. The panel consisted of public health faculty members, ergonomic experts, and occupational health professionals. Reliability tests were conducted for the scales, and a Cronbach α of 0.7 or higher was considered acceptable. To evaluate whether the questions measured the underlying constructs, 59 items were analyzed in a sample of 30 nurses who shared similar demographic characteristics. Of all participants, 2% dropped out of the study (response rate = 98%).
Items in questionnaire and maximum and minimum scores
All statistical analyses were performed using SPSS v.20.0 (IBM Corp., Armonk, NY, United States). We analyzed the data by performing paired and independent t tests. Statistical significance was set at α = 0.05 in all analyses.
Results
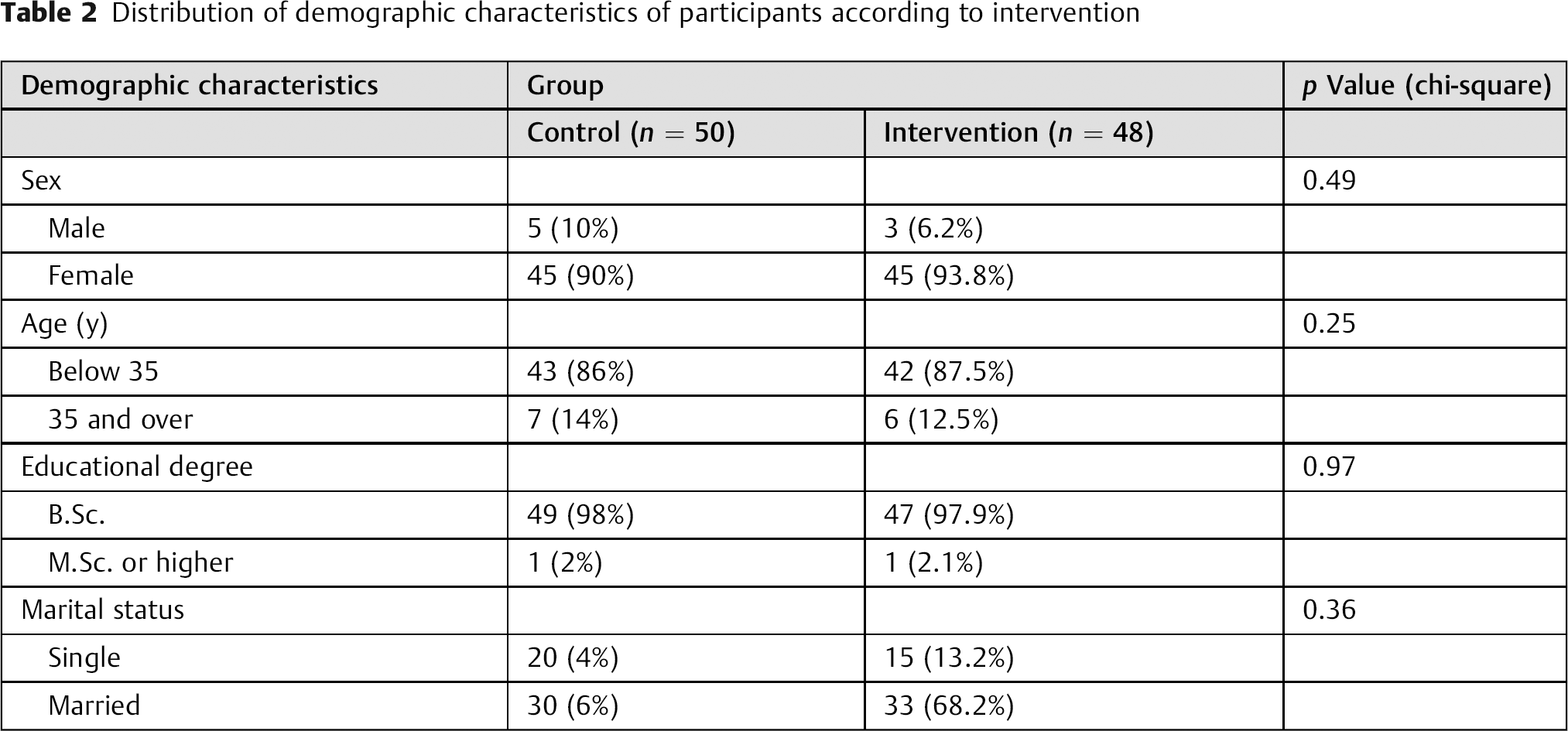
The result of the questionnaire reliability revealed that Cronbach α ranged from 0.72 to 0.79 in the four parts (the knowledge quiz, the HBM constructs, self-efficacy, and the checklist of performance). There was no significant difference in the demographic characteristics between the case and control groups (Table 2).
Distribution of demographic characteristics of participants according to intervention
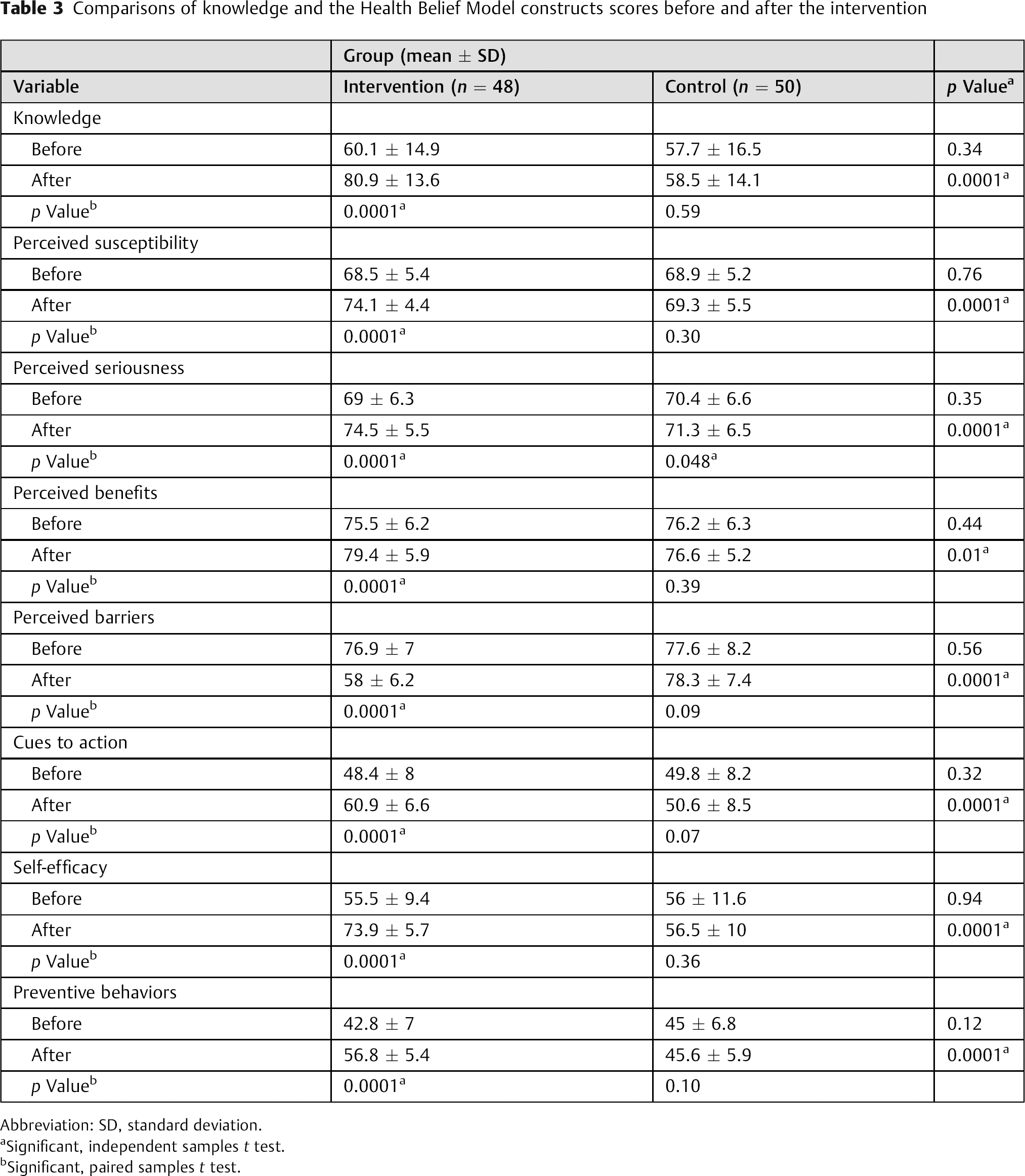
Preintervention evaluation of knowledge revealed that the majority of the nurses in both groups had insufficient knowledge regarding CLBP prevention (sometimes including postural advice and anatomical, physiologic, and ergonomic principles). Comparison of the baseline mean scores showed no significant difference in knowledge (t = −0.95, p = 0.34), perceived susceptibility (t = 0.30, p = 0.76), perceived barriers (t = 0.57, p = 0.56), cues to action (t = 0.98, p = 0.32), and self-efficacy (t = 0.76, p = 0.94) between the two groups (Table 3).
Comparisons of knowledge and the Health Belief Model constructs scores before and after the intervention
Abbreviation: SD, standard deviation.
Significant, independent samples t test.
Significant, paired samples t test.
The results of paired sample t tests showed no significant difference in the pretest and posttest knowledge scores of the control group (p > 0.05). The pretest–posttest mean differences of the HBM constructs were not also statistically significant in the control group (p > 0.05), except for the mean difference of the perceived benefits that showed a marginally significant difference upon completion of the study (p = 0.048). The participants in the control group also demonstrated low self-efficacy in the adoption of preventive behaviors of chronic LBP (t = −0.91, p = 0.36).
The mean knowledge score of CLBP was 60.1 ± 14.9 before the education and 80.9 ± 13.6 after the implementation of intervention in the intervention group. The difference between preintervention and postintervention mean knowledge scores was statistically significant (t = −9.28, p = 0.0001; Table 3).
The paired t test of health belief scores showed that the scores of the health belief subscales were mostly higher after the intervention when compared with before the intervention (p < 0.0001) in the intervention group (Table 3). The mean score of perceived barriers decreased significantly after the intervention (t = 14.37, p = 0.0001). The greatest increase was seen for the self-efficacy scores; the pretest average was 55.5 ± 9.9 and increased to 73.9 ± 5.7 after the intervention.
The subscales of HBM, perceived susceptibility (t = −6.64, p = 0.0001), perceived benefits (t = −4.01, p = 0.0001), perceived barriers (t = 14.37, p = 0.0001), cues to action (t = −11.24, p = 0.0001), and self-efficacy (t = −12.92, p = 0.0001) for LBP prevention behavior showed significant differences between the two groups after the intervention (Table 3).
Discussion
In this study, an educational program was performed based on the HBM. The results of this study showed an increase in the mean scores of perceived susceptibility, perceived severity, perceived benefits, and self-efficacy and also a decrease in the mean score of perceived barriers after the implementation of the educational program in the intervention group. Preintervention evaluation of the knowledge level showed a deficit in the nurses’ knowledge of LBP prevention in both the intervention and control groups. Other studies also reported inadequate knowledge of the nurses about LBP prevention. 28 , 29 , 30 There is also a strong body of evidence that nurses with sufficient knowledge of and positive attitude toward LBP prevention are inclined to practice a higher level of LBP preventive behavior. 28 , 29 The findings of the current study suggested that the HBM could be used in prevention programs aiming at promoting behavioral changes.
The results also showed that among the HBM constructs, the greatest increase was seen in the mean score of self-efficacy after intervention, indicating that the nurses had a stronger belief in their own capabilities to execute preventive actions required for the prevention of LBP. In a study by Fongsri et al, the intervention reduced LBP and increased the tendency to engage in the recommended health behavior through the promotion of self-efficacy. 31
In our study, the perceived barriers decreased while the other subscales including perceived severity, perceived susceptibility, perceived benefits, and cues to action increased, indicating that the HBM-based educational intervention was successful. The program provided the participants with substantial empirical support for the HBM; however, more studies are needed to examine whether nurses put into practice the educational information they receive via LBP preventive interventions. A randomized controlled study designed to prevent low back injuries among 4,000 postal employees showed that the educational program did not change the rate of LBP, average costs of an injury, employees’ absence due to injury, and the rate of injury recurrence after returning to work. 32 A probable explanation for the existing conflict can be the multifactorial nature of LBP, which demands multicomponent interventions including educational and training programs, multidisciplinary interventions, and interventions to treat employees with LBP.
Limitations
The quasi-experimental design utilized in this study does not allow generalization of the results to other groups of nurses because many factors may not have been fully controlled.
Conclusions
The results of the study showed that an educational intervention program based on the HBM could promote preventive behaviors among nurses. Therefore, it is suggested that educational interventions based on health educational models replace routine interventions.
Disclosures
Naser Sharafkhani, none
Mahboobeh Khorsandi, none
Mohsen Shamsi, none
Mehdi Ranjbaran, none
Footnotes
Acknowledgments
This research was funded by Arak University of Medical Sciences. The authors thank the deputies of education and research of the university, the director of the research affairs, and the nurses who participated in the study.