
Abstract
Objective:
This study aimed to assess the magnitude and patterns of chronic musculoskeletal disorders among the population in East Gojjam zone, Northwest Ethiopia.
Methods:
A community-based cross-sectional study with 846 recruited study participants was done using a multistage sampling technique in conjunction with a simple and systematic random sampling technique. Face-to-face interviews, physical examinations, a semi-structured questionnaire adapted from the Community Oriented Program for Control of Rheumatic Diseases, and other literature were used to collect data. EpiData 3.1 was used to enter the data, which were then exported to STATA 14.0 for analysis.
Result:
The study had a response rate of 98.8%, with about 836 people out of a total of 846 expected to take part. The magnitude of musculoskeletal disorders was found to be 40.1%. Back pain was the most common musculoskeletal condition (16%) of the population, followed by osteoarthritis (10%) and other forms of arthritis (rheumatoid arthritis (8%), gout arthritis (6%)). The most common comorbidity (multimorbidity) patterns were hypertension (9.8%), diabetes (5.6%), obesity (3.9%), and others (2.2%).
Conclusion:
Almost one in four participants have at least one musculoskeletal disorder in Northwest Ethiopia. Rheumatoid arthritis, osteoarthritis, low back pain, and gout arthritis were the most common musculoskeletal disorders. The most common comorbidity patterns were hypertension, diabetes, obesity, and others. An in-depth investigation of the musculoskeletal burden at the national level will be critical for implementing evidence-based strategies, as well as early detection and screening, linking to health institutions, and direct interventions.
Introduction
The increasing prevalence of chronic non-communicable diseases (NCDs) is a serious concern throughout the world, as they are the leading cause of disease, disability, and mortality and have a significant influence on the healthcare system. Approximately 1.71 billion people suffer from musculoskeletal (MSK) conditions worldwide. 1
Musculoskeletal disorders (MSDs), which encompass more than 150 conditions affecting the bones, muscles, ligaments, and other connective tissues, are one of the world’s leading causes of chronic morbidity and disability, and a major contributor, accounting for 1.7%−3.4% of the global disease burden. 2 MSDs are the leading cause of activity limitation, loss of function, and long-term disability, as they cause fatigue, leading to early retirement from work, pain, and deformity of a joint. Back and neck pain, osteoarthritis (OA), rheumatoid arthritis (RA), and fractures are among the most disabling MSDs, posing considerable difficulties to healthy aging by reducing physical, mental, and functional capacities. 3
Globally, the burden of disease is changing away from communicable diseases to long-term NCDs, which typically include MSDs. 4 In the 2017 Global Burden of Disease (GBD) study, lower back pain remained the leading cause of disability, with MSDs accounting for three of the top 10 conditions in terms of disability and NCD burden, accounting for 16% of all years lived with disability (YLDs). 5 MSDs account for a higher proportion of overall YLDs in developed countries, and the growth was more gradual, rising from 27.3% in 1990 to 28.1% in 2010. 6 In the developed and developing countries, MSDs and disease burden account for only 3.4% and 1.7%, respectively. 7
MSDs are the most prevalent chronic disorders in the developing world, ranked second in the East Mediterranean and third in Africa, and they are on the rise among the general and working populations. 8 MSDs are the second most common cause of years lost to disability, according to GBD 2017, yet years of life lost in sub-Saharan Africa are decreasing, while the burden of MSDs will only increase as the sub-Saharan population ages. 9 Due to an emphasis on more serious and life-threatening health problems such as infectious illnesses, MSDs are less emphasized and empirically unrepresented in low- and middle-income countries (LMICs), particularly in Ethiopia. 10
MSDs are common occupational health issues that are characterized by a variety of symptoms such as pain, stiffness, and discomfort in various body locations that are either caused or exacerbated by poor fitness and poor health habits, but a large proportion of MSDs are caused by physical work exposures.11,12 According to studies, the prevalence of work-related MSDs in Ethiopia’s adult population ranges from 35% to 74.5%. 13
According to the World Health Organization (WHO) report, the increased prevalence of MSDs has been associated with both work-related and nonwork-related exposures. 14 The WHO and the International League of Associations for Rheumatology (ILAR) developed the Community Oriented Program for Control of Rheumatic Diseases (COPCORD) to collect information on MSK diseases as a major public health problem due to secondary disability and increased use of health resources. 15 Although the WHO-ILAR COPCORD recommends population-based epidemiological studies to assess the burden of MSDs in developing countries, previous studies in Ethiopia revealed that MSDs are focused on work-related (office workers) conditions, excluding large segments of the population such as farmers, unemployed, non-office workers, housewives, and others.16–19 As a result, despite extensive study on MSDs in the developed world, there is a paucity of information in Ethiopia that comprehensively analyzes the magnitude and patterns (pain locations, frequency, and distribution over the body) of chronic MSDs. Therefore, the reasons mentioned above triggered us to conduct this research to assess the magnitude and patterns of comorbidities of chronic MSDs among the population in Northwest Ethiopia. Furthermore, the finding of this research is essential for collecting population data, educating the community, identifying risk factors, early detection and screening, and linkage to health institutions. The study’s findings will also be used to develop evidence-based policies and guidelines for hospital administrators, health professionals, regional and national policymakers, and program managers in developing nations, including Ethiopia. In addition, the results of this study will be used as baseline data for future scholars.
Materials and methods
Study design, period, and area
A community-based cross-sectional study design was conducted in East Gojjam zone, from January 2018 to October 2018. East Gojjam zone districts include: Aneded, Awabel, Baso Liben, Bibugn, Debay Telatgen, Debre Elias, Debre Markos Town, Dejen, Enarj Enawga, Enbise Sar Midir, Enemay, Goncha, Goncha Siso Enese, Gozamin, Hulet Ej Enese, Machakel, Shebel Berenta, and Sinan. Debre Markos town, the capital city of East Gojjam zone, is located 300 km northwest from Addis Ababa, the capital city of Ethiopia. According to the 2007 Population and Housing Census of Ethiopia, the projected total population of the zone was 2,451,959 (1,199,952 males and 1,252,006 females). 20
Population
The source populations were all adults who are residing in East Gojjam zone for at least 6 months. The study population was all adults from randomly selected kebeles living in the East Gojjam zone for at least 6 months.
Eligibility criteria
All adult (18+ years old) participants who had lived in the study area for at least 6 months before the study were included, and participants who were critically ill during the study period and those with MSD congenital disorders were excluded from the study. In addition, participants who reported any history of fractures or soft tissue injuries in any location of the body in the previous 6 months were excluded to minimize overestimation.
Sample size determination and sampling procedures
The sample size (846 participants) is determined using single population proportion formula by assuming 95% confidence level, 5% margin of error, 50% proportion of musculoskeletal disorders (MDs), design effect of 2, and 10% non-response rate. Due to the use of multistage sampling technique, the design effect was taken into account to reduce sampling error and ensure representativeness

Regarding sampling procedures, the multistage sampling method was used to select the study participants. First, six districts (30% of districts) such as Debre Markos town, Machakel, Bibugn, Dejen, Enbise Sar Midir, and Hulet Ej Enese were selected randomly using a lottery method from a total of 17 districts of the East Gojjam zone. Second, the district was classified into kebeles and some of the kebeles were selected using a simple random sampling technique (lottery method). Finally, households from each of the kebeles were selected using a systematic sampling technique. The numbers of households sampled from the selected kebeles were determined using proportionate-to-population size (the number of populations in each selected kebele divided by total population from all selected kebeles and multiplied by total sample size). The sampling interval (K) value was calculated for each selected kebele by dividing the total households in each selected kebele by the corresponding proportional sample size (total number of basic sampling units in the population divided by the number of sampling units needed for the sample). The first household was selected using the lottery method; if there are two or more study units within the household, the lottery method was used to select the participants. Then the next household was selected at every Kth interval. If there was no eligible candidate in a selected household or the selected household is closed even after revisit, the sampling process was continued to the next household until getting an eligible participant.
Study variables
The magnitude and pattern of chronic MSD comorbidity were dependent variables, while demographic factors like age, sex, educational background, occupation, and ethnicity; chronic diseases such as diabetes mellitus, hypertension, obesity, and others; behavioral and occupational characteristics like alcohol consumption, smoking, working posture, duration of working hours, and physical activity were independent variables.
Data collection tools and procedure
The data were obtained through a face-to-face interview at the respondents’ homes, using a pre-tested (5% of the study population) and standardized questionnaire. The questionnaire covered MSK problems, sociodemographic factors, behavioral and occupational characteristics, and chronic diseases. The questionnaire was initially written in English and translated into Amharic with cultural adaptations (local and national language), and then translated back to English with cultural adaptations to ensure consistency. The main questionnaire used in this survey to identify MSDs was the COPCORD Core Questionnaire, 21 and it was developed by reviewing the relevant literature. The questionnaire included socioeconomic status, demographics, work-related MSDs, medical and surgical conditions, pain intensity, physical limitation, and help-seeking behavior. Data on the population were collected in three stages: first, to find cases, a local health worker conducted a house-to-house survey; second, the community nurse used interview-based questionnaires to record pain and disability; and finally, all patients who reported pain, swelling, or stiffness in the last 7 days or at any point in their lives were considered positive for clinical assessment by trained health professionals, and a standard medical evaluation was performed using standardized criteria for RA, 22 OA, 23 back pain, 24 and gout arthritis (GA). 25
Data quality assurance
Data collectors were given 3 days of training in data collection procedures and research ethics. The data collection process was supervised by the investigator. The collected data were checked for completeness, accuracy, and consistency by the investigator. The coded data were checked for accuracy and completeness before being analyzed. Trained persons conducted interviews and anthropometric measurements in at least two visits to participants’ homes.
Statistical Analysis
The data were checked, cleaned, entered into EpiData version 3.1, and exported for analysis to STATA version 14. To summarize the data and identify the association of independent variables with outcome variables, descriptive statistics were used.
Ethical consideration
The actual gathering of data started after the study was approved by Debre Markos University Ethical Review Board. Local administrative bodies were also communicated about the study, and permission was obtained before the study. Finally, informed written consent was obtained from the participants.
Operational definition
MSDs are defined in this study as pain and/or discomfort in at least one of the following body parts at least once in the past 6 months: neck, shoulder, upper back, elbow, lower back, wrist/hand, hips/thighs, knee, or ankle/feet.
Result
Population characteristics
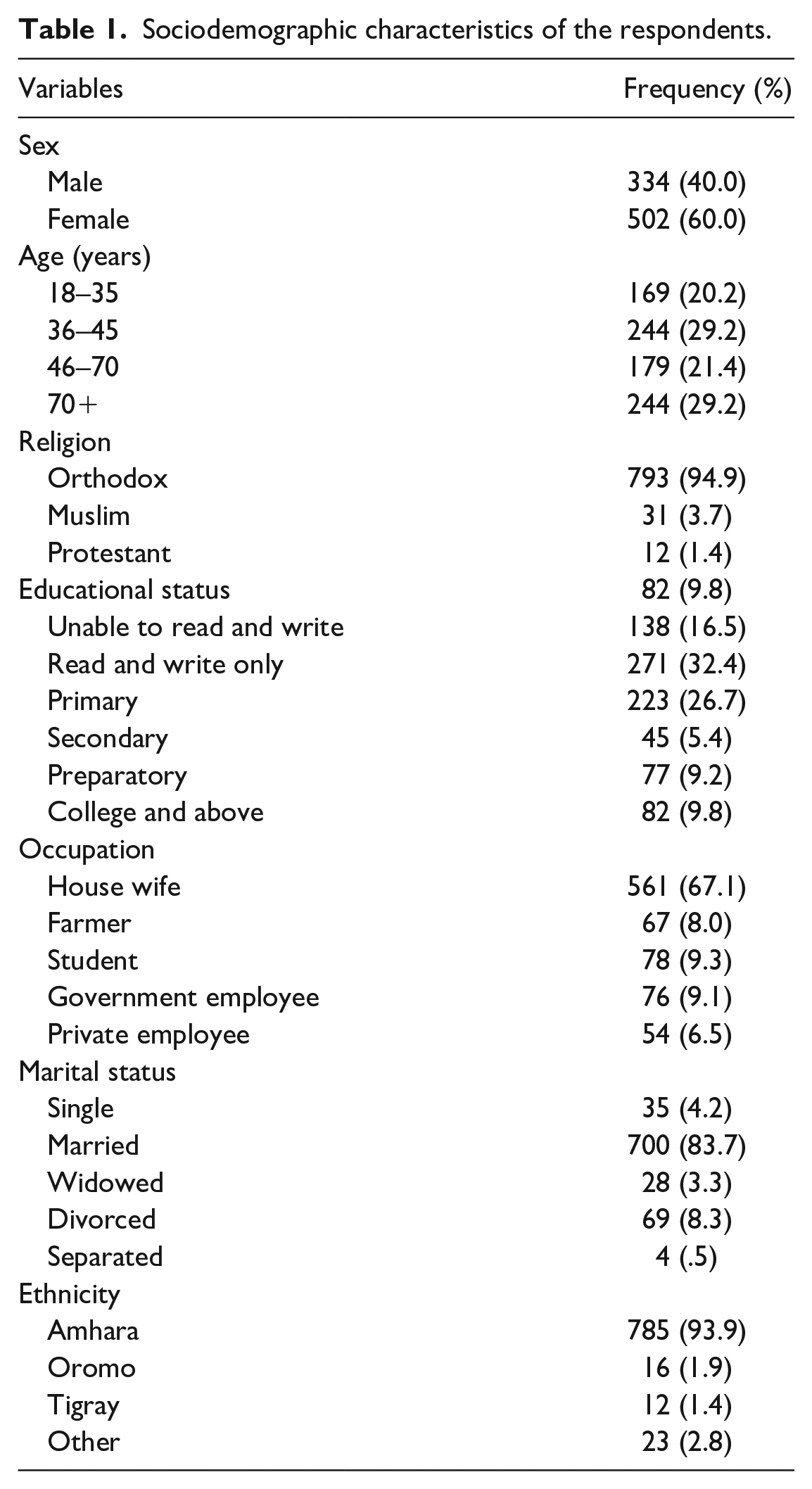
A total of 836 participants aged 18–82 years were interviewed in this study, with 244 (29.2%) aged 36–45 years. With regard to educational level, 271 (32.4%) can read and write and 223 (26.7%) completed primary school (Table 1).
Sociodemographic characteristics of the respondents.
Magnitude and pattern of comorbidities of chronic MSDs
Almost one (40%) in four participants have at least one MSD. RA, OA, low back pain (LBP), and GA are the most common MSDs. Of these, chronic LBP was the most prevalent chronic MSD in both men and women. Back pain was the most prevalent MSD, affecting 134 (16%) of the population, followed by OA (84%) and other types of arthritis (RA 67 (8%), GA 50 (6%)). A total of 180 (21.5%) of those with a MSD also had at least one other chronic disease. The most common comorbidity (multimorbidity) patterns were hypertension (9.8%), diabetes (5.6%), obesity (3.9%), and others (2.2%). Females were more common than males to have chronic back pain (10.8% vs 5.3%) and OA (6.3% vs 3.7%), whereas all other conditions were equally prevalent in both genders (Table 2).
Disease characteristics of the study participants (n = 836).

RA: rheumatoid arthritis; CBP: chronic back pain; GA: gout arthritis; OA: osteoarthritis; BMI: body mass index; MSD: musculoskeletal disorder.
Heart disease, mental and behavioral problems.
Discussion
MSDs, which include more than 150 different conditions, have a major impact on quality of life and well-being due to acute and chronic pain, discomfort, physical restrictions, comorbidity, and mental health challenges. 1
MSDs caused approximately 1.3 billion prevalent cases, 121.3 thousand deaths, and 138.7 million disability-adjusted life years (DALYs) globally in 2017. 26 MSDs have historically received less attention in Africa, particularly in Sub-Saharan Africa, and many African nations’ scarce health resources are being prioritized to meet the issues of infectious and communicable diseases. 27 Although various studies have been conducted on the prevalence of MSDs worldwide, there has been no research done on the magnitude and patterns of MSD comorbidity in Ethiopia.
Thus, this study aimed to assess the magnitude and patterns of comorbidities of chronic MSDs among the population in Northwest Ethiopia.
The overall prevalence of MSDs among the population in Northwest Ethiopia was found to be 40.1%. This finding was comparable to that of a study done in Vietnam, 28 South Asia, eastern sub-Saharan Africa, and central Latin America. 26 However, the current study’s findings were lower in comparison with research conducted in the United Kingdom (52%), Norway (56%), Sweden (64%), and Taiwan (90%),29–32 but higher than the research conducted in the United States (29.0%), 33 France (from 10% to 50%), 34 and Pakistan (31.6%). 35 This discrepancy could be attributed to changes in methodology, study setting, differences in geographical areas, sample size, individual pain perception, cultural differences, and study participants’ income which are related to differences in work conditions and the impact of occupational hazards. 36 Another reason for the disparity could be the age of the participants, as well as the different assessment tools used to evaluate MSDs. MSD prevalence has been observed to vary across geographical boundaries and occupational categories, 37 and the magnitude of MSDs varies due to a variety of data collection tools, the subjectivity of terminologies, cultural differences in MSD perception and reporting, and organizational differences in work environments.
The patterns of multimorbidity among MSDs are assessed in this study. Because MSK diseases are such a clinically diverse group, the prevalence of multimorbidity may vary by subtype. Hypertension, diabetes, and obesity were the highest prevalence of multimorbidity of MSDs in this study. This was supported by the studies done in the WHO and the Lebanese Ministry of Health (MOH).38,39
Among major MSDs, chronic LBP has the highest prevalence in this study. A study reported that the prevalence of chronic LBP and OA ranged from 0.9% to 24%.40–42
According to this study, females were more common than males to have chronic back pain (10.8% vs 5.3%) and OA (6.3 vs 3.7%), but the prevalence of all other disorders was relatively similar between males and females, which is supported by a study done in Australia. 43 The mechanism underlying these sex differences is unclear, but they could be due to differences in sex-related biological factors (hormones or physiology), differences in pain severity, or women’s tendency to perceive and cope with pain differently, as well as differences in social or psychological factors.44,45
According to COPCORD studies, the prevalence of RA was 0.4% in India and from rural areas of other developing countries has ranged from 3.95% to 8.5%. 46 The reason for the higher prevalence of OA in the current study compared with other rural areas would need to be researched further. Because of the high prevalence of these diseases and the need for healthcare in rural areas, these ailments should be treated at a low cost through early diagnosis and screening, linking to health institutions, and direct treatments at the village level through the public healthcare system. It was found in our study that 21.5% of participants had one or more MSDs. Comorbidity among persons with chronic MSDs differed by age, with older people having more comorbidities than younger ones. This is in line with a study conducted in Australia and Brazil, which indicated that as people got older, the number of chronic diseases increased. 47 This could be because as people get older, they are more likely to have physical and functional incapacities, which can reduce their quality of life. 48
Because of their extended duration, incapacitating effects, and continual use of healthcare services and resources, MSDs cannot be disregarded as minor problems. 49 MSDs can have considerable medical, economic, and societal impacts, as well as play a significant role in the population’s health profile. 50 Hence, while planning healthcare services and determining research priorities and implementation across the health system, specific concerns tailored to MSD screening and management must be taken into account. Despite significant investment in reducing the prevalence of MSDs in LMICs, little research is available to inform policy and decision-making. As a result, more research is needed to establish consolidated evidence on a global level, as well as in developing countries in particular.
Limitation of the study
The data limitations and gaps associated with these analyses should be kept in mind for future research and interpretation of the primary findings provided here. The results of this study should be interpreted with some limitations. Because the sample was obtained from community-dwelling groups and did not include those living in care facilities or hospitalized patients, a selection bias toward sampling healthier respondents is anticipated. Furthermore, because some of the data collected are based on self-reported symptoms, recall bias may exist. Despite these limitations, this is the first study in the region to use a COPCORD questionnaire to assess the magnitude and patterns of comorbidities of MSDs in Northwest Ethiopia.
Conclusion
Almost one in four participants have at least one MSD in Northwest Ethiopia. RA, OA, LBP, and GA were the most common MSDs. The most common comorbidity patterns were hypertension, diabetes, obesity, and others. MSDs have a high prevalence of comorbidities, which should be incorporated in the patient’s routine workup and integrated with a holistic approach to the patient for screening and future standardized comorbidity management programs.
An in-depth investigation of the MSK burden at the national level will be critical for implementing evidence-based strategies, as well as early detection and screening, linking to health institutions, and direct interventions.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221085109 – Supplemental material for Musculoskeletal disorders among the population in Northwest Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221085109 for Musculoskeletal disorders among the population in Northwest Ethiopia by Yoseph Merkeb Alamneh, Bickes Wube Sume and Abtie Abebaw Shiferaw in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our gratitude to the study participants, data collectors, and supervisors, including Getachew Chane, Mengistu Ayele, and Asfaw Gerbi.
Authors’ contributions
YMA and AAS wrote the proposal and participated in data collection; approved the proposal with some revisions; developed the design and methodology of the study, literature review, and quality evaluation. YMA and BWS performed statistical analysis, data interpretation, and drafting of the article; developed the study design and protocol, literature review, statistical analysis, interpretation of the data, and developing drafts of the article. All authors read and approved the final article.
Availability of data and material
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethical clearance letter has been received from the research and review committee at Debre Markos University (SOM 0013/14). In addition, before beginning, data collection permission was obtained from the hospital authority.
Informed consent
Informed written consent was received from each participant after explaining to them the research objectives. The participants were briefed on the study’s purpose, procedures, potential risks, and benefits. In addition, the participants were told that failure to agree to or withdraw from the study would not change or endanger their access to treatment.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.