
Abstract
Study Design
Cross-sectional survey.
Objectives
This study aimed to investigate work-related neck pain among AO spine surgeons in different regions by estimating its prevalence, predictors, consequences, and management methods.
Methods
A cross-sectional survey of 411 spine surgeon members of AO spine was conducted during March–May 2021, using the Modified Nordic Questionnaire and the Neck Disability Index. Data on neck pain experience during the last 12 months and its consequences and risk factors were collected. Logistic regression analysis was done to identify significant predictors of neck pain. Significance was set at P < .05.
Results
The 1-year neck pain was experienced by 66.7% of surgeons. According to the Neck Disability Index, more than one-half (52.8%) experienced disability due to neck pain of mild (45.5%), moderate (6.5%), and severe (.8%) grades. Neck pain was responsible for stopping work in 17.5% of surgeons, with a median of 3.5 (IQR, 2-7.8) days off work. One-half of the participants (56.3%) were treated by medical care, 31.5% by physiotherapy, and 16.5% requested rest days and sick leave. Physical stress (P < .001) and non-exercising (P = .04) were the significant predictors of neck pain.
Conclusion
The 12-month prevalence of neck pain was high among spine surgeons, with an impact on activities of daily living, mainly of a mild degree, reported by one-half of surgeons. Physical stress was the only significant predictor, while sports practice was a protective factor against neck pain. Medication was the primary management adopted—an increased focus on pain prevention through improved workplace ergonomics and sports activity programs is recommended.
Introduction
Neck and low back pain cause personal suffering, disability, and impaired quality of work and life in general, which can be a great socio-economic burden on patients and society.1-4 In the Netherlands, the total cost of neck pain in 1996 was estimated at 686 million US dollars, 5 whereas, in 2006, Katz 6 proposed that the total cost of low back pain in the United States exceeds 100 billion US dollars per year.
There are potential societal “costs” directly attributable to surgeon musculoskeletal disorders (MSD). Direct costs of time off work or specific treatment for MSD include disability insurance and reduced income. Indirect costs include delay in evaluation and management of patients. In previous study, 7 31.9% took time off work attributable to MSD, ranging from a half day to forced retirement. The public health impact of surgeon absence because of MSD is unknown.
Orthopedic surgeons are exposed to a particularly hazardous day-to-day working environment with risks of exposure to infection, radiation, smoke, chemicals, excessive noise, emotional and physiological disturbances, and musculoskeletal injuries. 8 In 1995, Mirbod found higher rates of subjective physical injuries in orthopedists as compared to general surgeons, with the most commonly injured areas reported as the back, neck, shoulders, arms, and hands. 9 In 2011, Auerbach and colleagues conducted a survey of spine surgeons and reported a similarly high incidence of low-back, neck, shoulder, wrist, and hand pain. 7
Various risk factors for cervical spine disease have been explored, however few have been studied in surgeons. Prior studies of the general population have shown certain risk factors for cervical spine disease including older age, female gender, elevated body mass index (BMI), decreased quality of life, increased stress, and possibly cigarette smoking.10-15 Occupational risk factors for cervical spine disease include repetitive movements, carrying heavy loads on one’s head, and extension or flexion strain.16-20 Currently, there are limited studies that have addressed the known risk factors for cervical disease in the physician population.
There is a paucity of research on occupational hazards associated with orthopedic spine surgery.21,22 Surgeons too often are neglectful of their health, despite the fact that health is associated with length of career and with work-related stress.21,23,24 Several studies have examined certain psychosocial aspects of choosing a surgical career, including quality of life, divorce rates, alcohol or substance abuse, burnout, and stress.21,25
Risk factors such as nonneutral posture, repetitive forceful movements, and nonergonomic instrumentation are common factors in orthopedics that contribute to the development of musculoskeletal injury.26,27 Neck pain and cervical radiculopathy/myelopathy are common among orthopedic surgeons. Associated factors included older age, higher stress levels, and performing arthroscopy. 28
Loupes are also commonly used and could result in altered posture during surgical procedures. The prevalence of neck pain or radiculopathy in the orthopedic cohort associated with loupe or arthroscopy use has not been fully assessed. 28 Sivak-Callcott 29 identified that the use of loupes and headlamps were potentially contributing sources of pain.29-31 A 2004 survey conducted by Esser and colleagues found 16 of 17 Mayo Clinic surgeons performing Mohs surgery had musculoskeletal symptoms caused by or made worse by performing surgery, with the most common complaints being stiffness in the neck, shoulders, and lower back. 32
To the best of our knowledge, no study has evaluated the prevalence of neck pain among orthopedic spine surgeons, despite the fact that work- related injuries constitute more than 60% of all occupational illnesses.33,34 The aim of this study was to investigate work-related neck pain among AO spine surgeons in different AO regions, by (1) estimation of the prevalence of work-related neck pain, and (2) determination of its predictors, its personal and occupational consequences, and the different management methods adopted for it.
Methods
Study Design
AO Spine is the leading global academic community for innovative education and research in spine care. A cross-sectional study of spine surgeon members of AO spine, from different AO regions, within a period of 2 months during March and May, 2021. All active on duty surgeons during the survey were eligible for inclusion. Those who were pregnant at the time of study were excluded. Sample size was estimated based on a prevalence of neck pain of 59% among spine surgeon members of the Scoliosis Research Society. 7 With a margin of error of 5%, and 95% CI, the estimated sample size was 372. To compensate for an average of 10% no response/incomplete surveys, a sample size of 419 surgeons was adopted. A total of 411 surgeons responded with valid, completed questionnaires.
Data Collection
We developed an online, web-based, cross-sectional survey adapted from the previously validated Nordic Musculoskeletal Questionnaire (NMQ),35,36 using an online survey generator. The e-questionnaire was structured into five sections:
Section (1) consists of Surgeons’ demographic information, which is personal information on surgeon’ height and weight. These were used to calculate participants’ body mass index. Information on the age, gender, marital status, and ever history of neck pain or radiculopathy, were also collected.
Section (2) consists of lifestyle information, which is information on the surgeons’ lifestyle and behaviors such as walking, running or other sports for 15 minutes/day, and smoking habits.
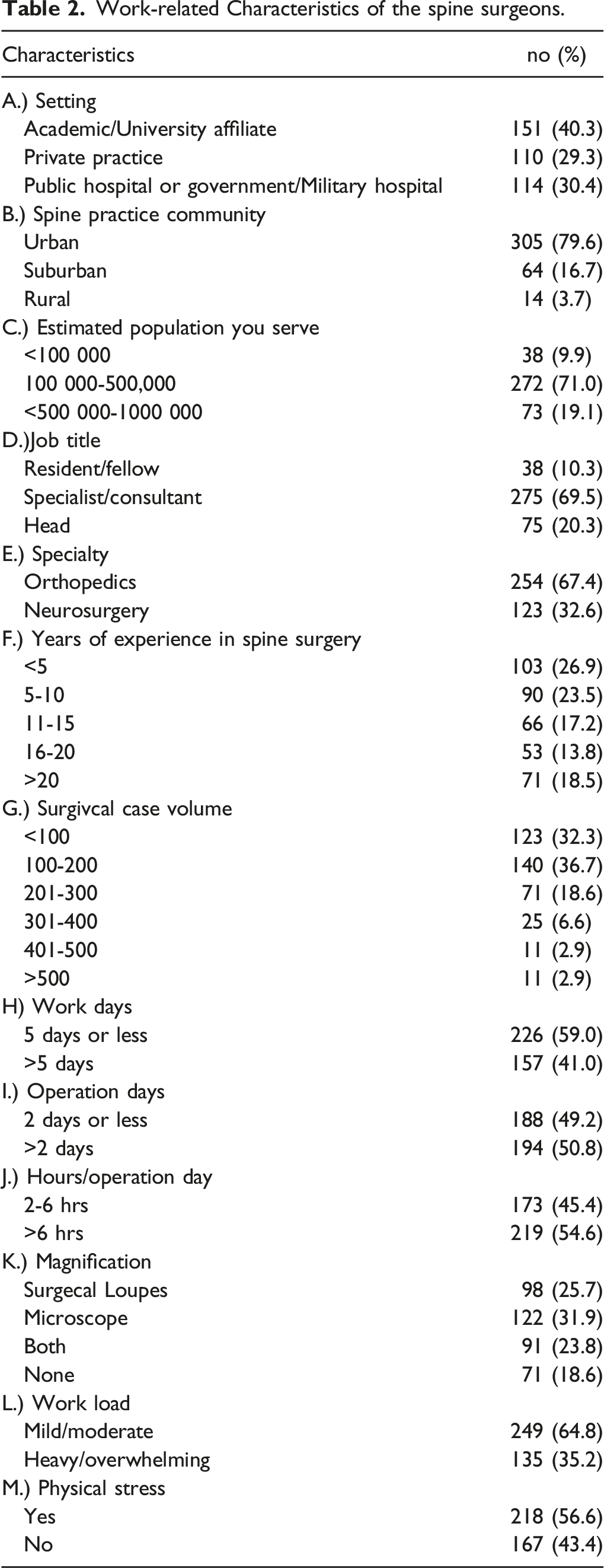
Section (3) is work-related characteristics, which investigates the nature of the participants’ responsibilities. Questions regarding the work setting, spine practice community, amount of work load [estimated population served, specialty (orthopedics or neurosurgery), years of experience, surgical case load, work days/week, work hours/operation day], level of work load, presence or absence of physical stress, and the use of magnification (surgical loupes, microscope or both) were included.
Section (4) is Work-related neck pain, which is information on the presence of neck pain in last 12 months preceding this present study using a modified Nordic questionnaire.35,36
Section (5) Neck pain consequences. Information were collected on neck pain consequences on activities of daily living was collected using the Neck Disability Index (NDI), 37 which is a questionnaire designed to give information as to how subject neck pain has affected his/her ability to manage in everyday life. It has become a standard instrument for measuring self-rated disability due to neck pain and is used by clinicians and researchers alike. It is composed of 10 sections, each section assesses the level of disability in one of the daily activities, such as dressing, reading, sleeping, driving, etc. Each of the 10 items is scored from 0 - 5 (0 = no impact, 5 = high impact). The grade of disability from neck pain was determined for each surgeon based on the total score in the NDI, as follows; no disability (0-4 points), mild disability (5-14 points), moderate disability (15-24 points), and severe disability (25-34 points). Time off work and sick leaves due to neck pain, and how the pain was managed were inquired about.
This study was conducted electronically between March 2021 and May 2021, with a total of three contacts (two reminders) made resulting in an 82% response rate
Data Analysis
SPSS software version 27 was used for data entry and analysis. Descriptive statistics such as mean score and standard deviation, as well as frequency and percentages of all independent variables were used. Prevalence rates were calculated as the ratio of the number of reported symptoms to the total number of participants (n = 411). Analytic statistics were applied to test associations of the neck pain prevalence and surgeons as well as work-related characteristics. Chi-square test was used for qualitative data and Student’s t-test was applied for quantitative data. Univariate analysis was used to examine relationships between neck pain and individual/lifestyle and work-related factors. Odds ratios and corresponding 95% confidence intervals were estimated to assess the strength of association between the prevalence of neck pain possible risk factors. To determine the significant predictors of neck pain, logistic regression analysis was performed including only variables that were shown significant in the univariate analyses. Statistical significance was considered at P-values of ≤.05.
Results
Personal Characteristics
Spine surgeons’ personal characteristics.
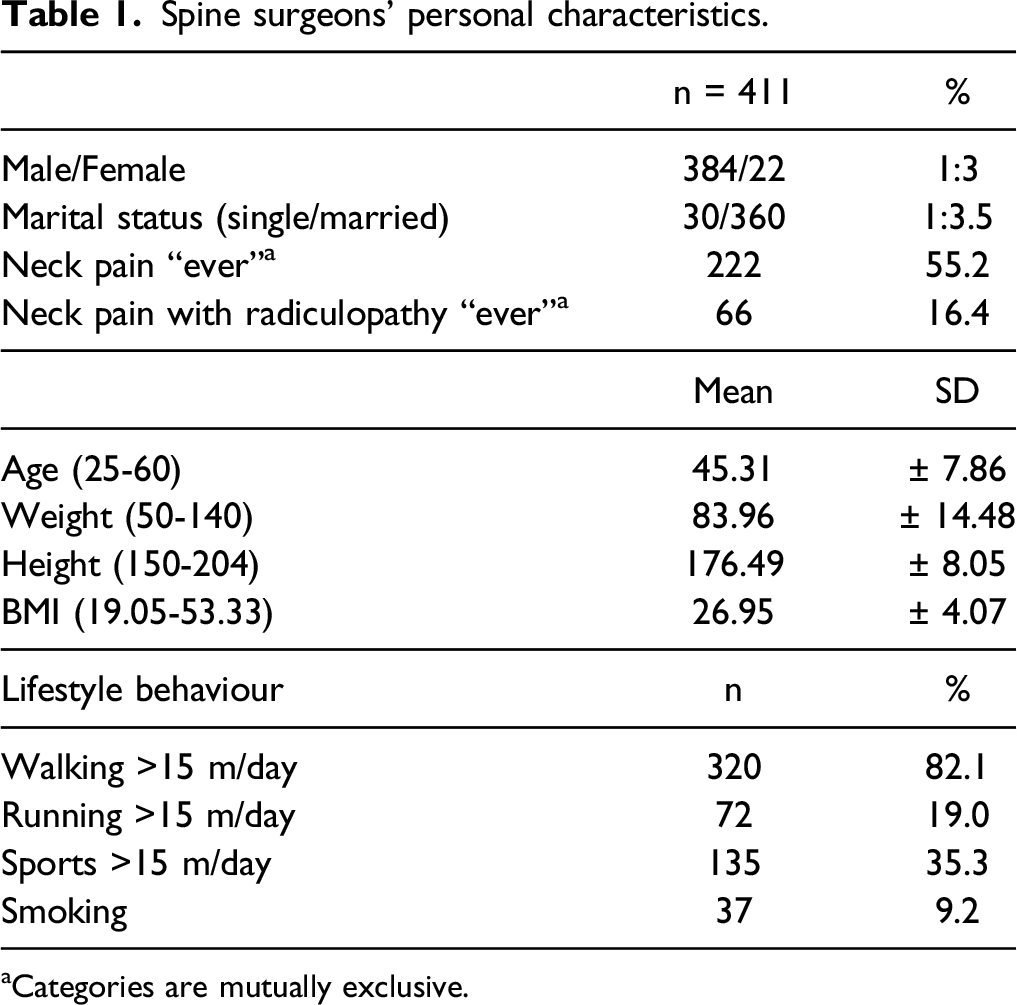
aCategories are mutually exclusive.
Work-Related Characteristics
Work-related Characteristics of the spine surgeons.
Prevalence of Neck Pain and Associated Work-Related Neck Pain
Prevalence and consequences of neck pain among spine surgeons in the past 12 months.
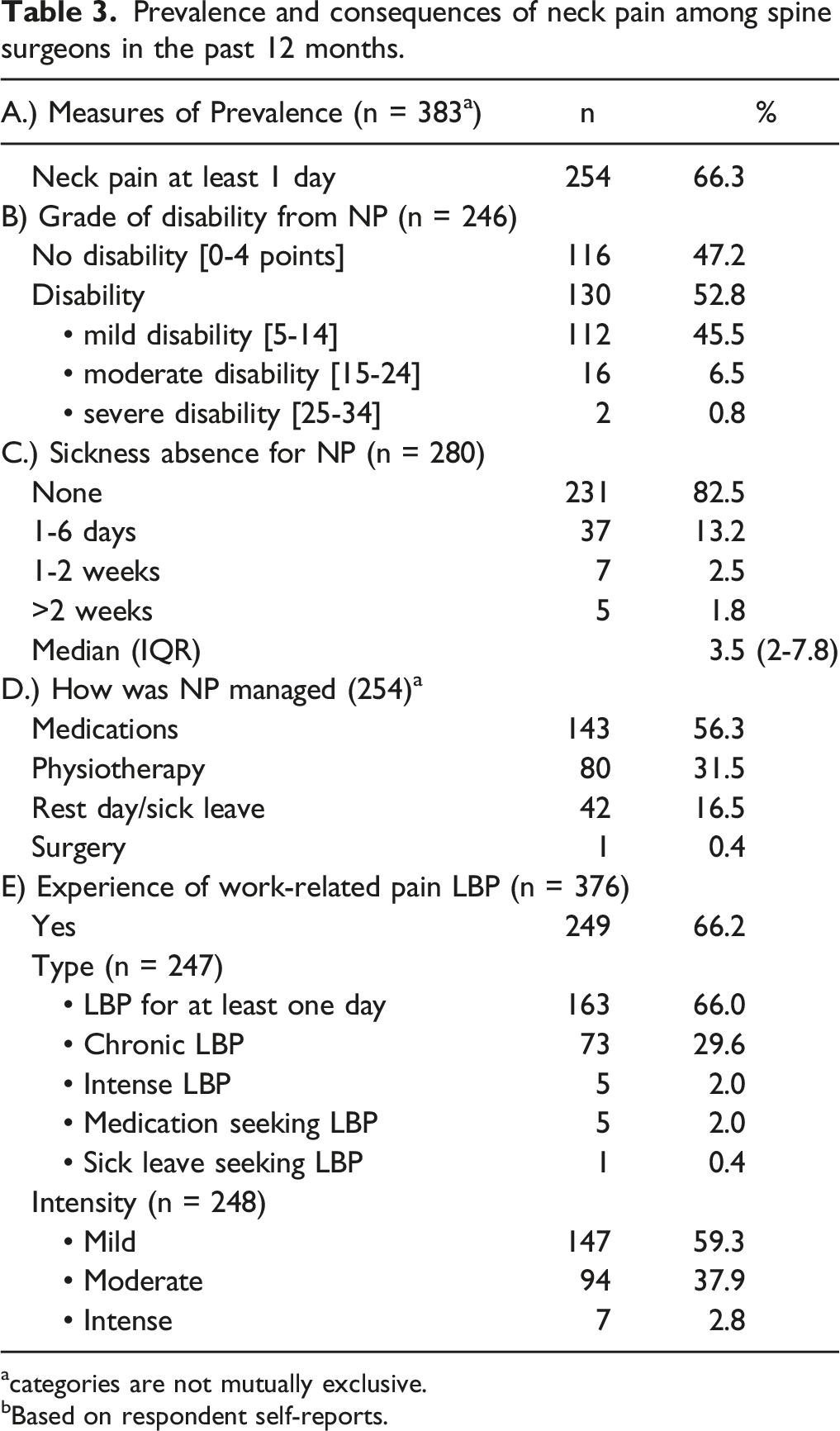
acategories are not mutually exclusive.
bBased on respondent self-reports.
Factors Associated With Neck Pain
Prevalence of Neck pain and Association with Some characteristics among spine surgeons.
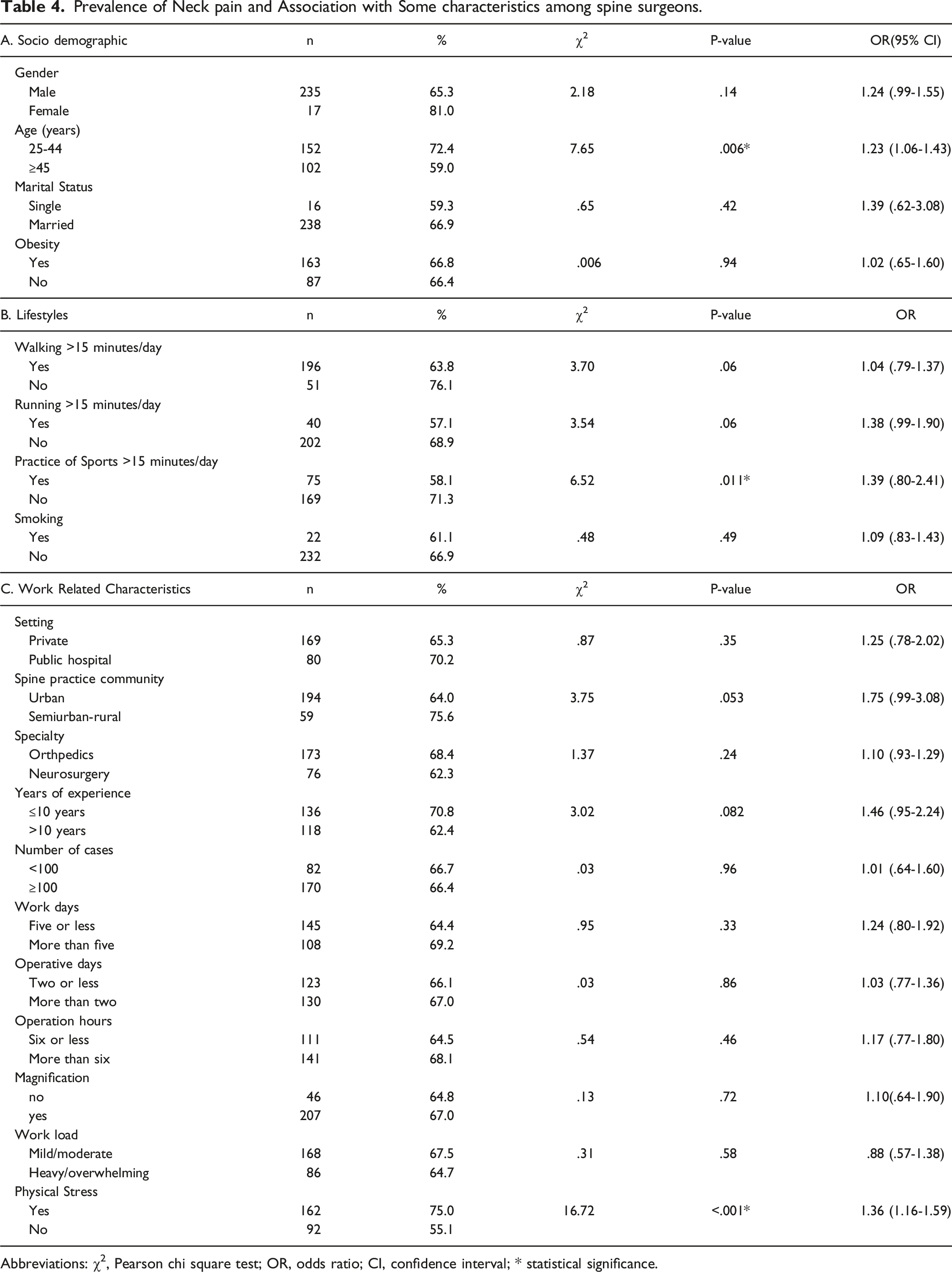
Abbreviations: χ2, Pearson chi square test; OR, odds ratio; CI, confidence interval; * statistical significance.
Significant predictors of Neck Pain among Spine Surgeons.

Abbreviations: OR, odds ratio; CI, confidence interval; β, beta coefficient; SE, standard error; *, statistical significance.
Discussion
Neck pain and cervical radiculopathy/myelopathy are common among orthopaedic surgeons. 28 In our study, a prevalence of neck pain over the past 12 months was 66.3% among spine surgeon members of AO spine, a rate that compares with figures of 59 and 59.5% in two previous studies among orthopedic surgeons,7,35 and exceeds the prevalence of 38.9% in a third one. 9 It exceeds ophthalmologists (51%), urologists (28%), and dentists (26%).38-40 The higher rates among orthopedic spine surgeons may be expected from sustained neck flexion during prolonged manual procedures. In support of this, Gerbaudo et al recently demonstrated that awkward posture accounted for 71% of work-related MSD among health care workers, which was greater than that seen in workers who were exposed to manual lifting of weights. 41
We hypothesized that increased age, increased job stress, and the use of loupes or arthroscopy would be associated with greater rates of neck pain. The general surgery literature acknowledged that laparoscopic surgery,42-48 and the use of loupes and headlamps was associated with higher rates of pain and musculoskeletal disorders.29-31 Nguyen and colleagues 44 attributed their findings of pain with laparoscopic surgery to the static positions of the neck and trunk and associated frequent movements of the upper extremities. In the present study, the majority of surgeons reported the use of microscope, surgical loupes or both, with no significant association between the use of magnification and neck pain. However, the duration of performing endoscopy, which places surgeons at higher risk of spine problems, with a cumulative effect on the spine, 42 was not investigated in our study. In a previous study of occupation-related cervical spine disease in orthpedic surgens, 28 those who had a greater number of years performing loupe procedures or arthroscopy procedures had markedly increased rates of neck pain and cervical radiculopathy/myelopathy, but after adjusting for age and sex, performing loupe procedures did not increase the odds ratio for neck pain. 28 In the present study, nearly one-half of surgeons reported an experience of more than 10 years (49.5%), with no significant association between neck pain prevalence and years of experience. As technologies such as robotics become more prevalent, the way surgeons operate could change and affect the prevalence of neck pathology in the orthopedic community.49,50 Prior to the advent of digital operating rooms with mobile or customizable positioning of the monitors on booms, surgeons often maintained a rotated position of their cervical spine in order to view the monitor while operating. 42
Demographic factors such as; sex and age have been investigated as risk factors for MSK disorders.28,35,51,52 Previous studies have shown greater rates of neck pain in women.51,53-55 In our study, there was no significant association between gender and neck pain, in agreement with a previous study by Wyatt et al. 28 Older age was associated with increasing rates of neck pain and cervical radiculopathy/myelopathy.28,51,52 A previous study reported high rates of MSK pain among resident orthopedic surgeons (59%), which was a concerning finding in a very early stages of their careers. 35 In our study, young age surgeons reported higher prevalence of neck pain than did the older age ones. However, after adjusting for other variables, this association disappeared. This association might be due to possible less experience or due to more physical stress. The high prevalence of musculoskeletal complaints among young surgeons could also be due to poor ergonomics in the operating room. While it is hopeful that as these young surgeons advance in their careers, they will learn how to operate with more appropriate body positions and to perform their tasks more ergonomically, earlier education in orthopedic ergonomics may reduce these rates and limit lifetime exposure to hazardous body positions. 35
While there are various physical stresses and hazards applied to physicians in general, orthopedics surgery is one of the most physically taxing of the medical specialties. Prolonged working hours in ergonomically challenging postures have been identified as risk factors in other professions.56,57 In our study, heavy/overwhelming work load and physical stress were reported by mere than one-third and one-half of surgeons respectively (35.2% and 56.6% respectively), and Increased levels of physical stress were markedly associated with neck pain. This finding was consistent with previous studies.28,51,53,58,59 The intense psychological and emotional challenges of surgical training, coupled with the focus on the safety and health of the patient, and a lack of education regarding surgical ergonomics creates an environment that may contribute to these high rates of neck pain. 35
Total spine caseload was found to be a risk factor for neck pain, most likely due to sustained neck flexion. 7 In a previous study, High case volume was the strongest predictor of cervical pain among laparoscopic surgeons, irrespective of age, height, or practice length. 60 In our study, population of 100 000-500,000 was the estimated population for the majority of surgeons, with a modal surgical case volume of 100-200 cases, modal work days of five or less days, and a modal work hours per an operation day of 6 or more hours. However, non of these work load-related factors was associated with neck pain. Neck pain and cervical radiculopathy/myelopathy are common among orthopedic surgeons. Associated factors included older age, higher stress levels, and performing arthroscopy. 29
There are potential societal “costs” directly attributable to surgeon MSD. Direct costs of time off work or specific treatment for MSD include disability insurance and reduced income. Indirect costs include delay in evaluation and management of patients. In a previous study, 7 31.9% of spine surgeons took time off work attributable to MSD, ranging from a half day to forced retirement. In our study, sick leave days due to work-related neck pain in the last year was reported by 17.5% of spine surgeons, ranging from 1day to more than weeks, with a median of 3.5 sick leave days (IQR, 2-7.8 days). The public health impact of surgeon absence because of neck pain needs to be evaluated.
Common treatments employed for neck pain included anti-inflammatory agents, narcotics, or muscle relaxants physical therapy/exercise, and brace or other form of temporary immobilization. 7 Many surgeons tried to relieve neck pain on their own through conservative modalities such as; nonnarcotic medications, heat or ice, and changing their sleeping environment. 28 This was the situation in our study, where medication raked first as the neck pain modality of management, followed by physiotherapy and rest, while only one surgeon experienced surgery to relief his/her neck pain. Although topical NSAIDs have shown some efficacy for the treatment of neck pain, there have been few studies on the efficacy of systemic NSAIDs for neck pain specifically.61,62 Therefore, there should be an increased focus on pain prevention through improved workplace ergonomics
Literature with respect to the effect of physical activity on neck and low back pain was contradictory.63-67 The results of a systemic review indicated limited evidence for no association between physical activity during leisure time and neck pain in the working population. 63 With regard to lifestyle, our study showed that the majority practised walking for more than 15 min/day, one-third practice sports for more than 15 min/day, and only 19.0% practiced running. However, our study showed that practice of sports was a the only significant protector against neck pain among spine surgeons. Further studies to prove this finding are recommended.
Limitations
Our study has limitations. First, this is a descriptive study of the career prevalence of neck pain in the spine surgeon population with no control group. Second, methodological differences in studies across disciplines and in the general population limit comparisons. Third, the anonymous nature of the survey precluded any comparison between responder and non-responder populations, and raises the possibility of selection bias. For example, the non-responders may include a higher proportion of unaffected individuals, with possible overestimation of the prevalence of neck pain because those who are affected by neck pain may be more likely to respond Fourth, this cross sectional study is not designed to be able to assign causality; therefore, the causal association between the outcome (neck pain) and other possible risk factors such as; sports practice and physical stress is not guaranteed.
Conclusion
Neck pain is common among orthopedic spine surgeons. Physical stress was the only predictor of neck pain, while sports practice was the only protector against its contraction. Use of magnification was not associated with neck pain prevalence. Utilization of simple ergonomic changes over time can lead to a reduction in neck pain and improved long-term workplace comfort. Institutions should also implement ergonomic training and allow for more convenient reporting of workplace injury.
Footnotes
Acknowledgments
This study was approved by the AO SPINE Research Commission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.