
Abstract
Study Design
Retrospective cohort study with a cross-sectional comparison.
Objective
To compare the rates of anesthesia prescription and satisfaction with surgery, prevalence and severity of low back pain, prevalence of depression, and sexual dysfunction among pregnant and nonpregnant patients with AIS undergoing correction surgery with pedicle-based systems and healthy woman with a history of pregnancy.
Methods
Women between the ages of 18 and 40 years who underwent correction surgery for AIS with a pedicle screw system were interviewed regarding pregnancies, child delivery, method of pain control during delivery, and any long-term outcome after delivery. In addition, sexual dysfunction (Female Sexual Distress Scale–Revised [FSDS]), depression (the Beck Depression Assessment Questionnaire), and Scoliosis Research Society 24 (SRS24) questionnaires were administered. Data was compared between patients with AIS without a history of pregnancy and healthy controls.
Results
Satisfaction with surgery in the AIS pregnant group using the SRS24 questionnaire scored 3.76/5 (p = 0.0047 when compared with nonpregnant AIS group). Six of the 17 of the women with AIS had severe back pain during pregnancy (35%) mandating home treatment or hospitalization. Of the 17 women, 13 complained of a sustained back pain after child delivery (76%) that impacted their life. In the nonscoliosis group, no back pain attributed to pregnancy was reported. The rates of regional anesthesia prescription among pregnant patients with AIS who underwent correction surgery was 30% (5/17), whereas among healthy pregnant women, rates were 100% (6/6). The SRS24 scores in the patients with AIS were 72% (88/120), showing a low score of 3.69/5 in the pain domains (p = 0.0048 when compared with nonpregnant patients with AIS). Depression rates were in the normal range and similar in all groups. FSDS scores, used to assess sexual dysfunction, were 4.02 in the pregnancy group and 5.67 in the nonpregnant group (not significant) and 4.6 in the nonscoliosis control group (not significant).
Conclusion
Women who underwent scoliosis correction suffered from long-term back pain after pregnancy and had decreased satisfaction with surgery. In addition, anesthesiologists refused epidurals in a large number of these patients. A larger study is needed on the topic.
Study Rationale and Context
Adolescent idiopathic scoliosis (AIS) is the most common form of scoliosis. 1 AIS is present in 2 to 4% of children between 10 and 16 years of age. With small curves of 10 degrees, the ratio of female to male is equal but increases to 10 females for every male with curves greater than 30 degrees. 2 Women more commonly require surgical treatment for AIS than men, 3 leading to long-term consequences on life.
Previous publications addressing patients’ quality of life and sequela of back pain years after surgery to correct deformity demonstrated no significant impairment of health-related quality of life. 4 , 5 With regard to pregnancy after the correction of a scoliotic deformity, 40% of the women suffered from increased low back pain during pregnancy. 6 However, no significant obstetric complications or long-term orthopedic problems (such as enlargement of the scoliosis curve or diastasis symphysis pubis) were seen in these patients. In one study, the main consequence of deformity correction was anesthesiologists being less inclined to offer neuroaxial regional anesthesia to patients in labor who had undergone anterior spinal surgery. 7 However, current data with posterior pedicle-based based systems is lacking.
Objective or Clinical Question
This study aimed to investigate the effect of deformity correction on pregnancy and delivery in women who have undergone surgery for AIS. The objectives of the study are:
To compare the rates of regional anesthesia prescription among pregnant patients with AIS who underwent correction surgery with posterior pedicle-based systems and healthy pregnant women
To compare the rates of satisfaction with surgery among pregnant and nonpregnant patients with AIS who underwent correction surgery with posterior pedicle-based systems
To compare prevalence and severity of low back pain among pregnant and nonpregnant patients with AIS who underwent correction surgery with pedicle-based systems and healthy woman with a history of pregnancy
To compare the prevalence of depression among pregnant and nonpregnant patients with AIS who underwent correction surgery with pedicle-based systems and healthy woman with a history of pregnancy
To compare the prevalence of sexual dysfunction among pregnant and nonpregnant patients with AIS who underwent correction surgery with pedicle-based systems and healthy woman with a history of pregnancy
Methods
Study Design
Retrospective cohort study with a cross-sectional comparison. The project was approved by the institutional review board of the Hadassah Medical Center, Jerusalem, Israel.
Patient Population
The study took place between 2010 and 2013. Seventy consecutive women between the ages of 18 to 40 years who underwent correction surgery for AIS with a pedicle screw system in Hadassah Hebrew University Medical Center, Israel, were considered for enrollment in this study. Among these, 25 (36%) had subsequent pregnancies. Among these 25 women, 5 were excluded due to postoperative complications, leaving 20 women (80%) enrolled in the AIS pregnancy cohort (Fig. 1). Among the 45 nonpregnant subjects, 8 were excluded due to postoperative complications, leaving 37 women (82%) who were enrolled in the AIS nonpregnant cohort (Fig. 1). For the cross-sectional cohort, 55 healthy women were approached in various acceptable public venues and signed up for study participation. Among these, 40 (73%) met study criteria and agreed to participate in the healthy women nonsurgical cohort (Fig. 1). Six of these women (15%) experienced pregnancy and delivery. The study was approved by the Institutional Review Board of the Hadassah Hebrew University Medical Center.
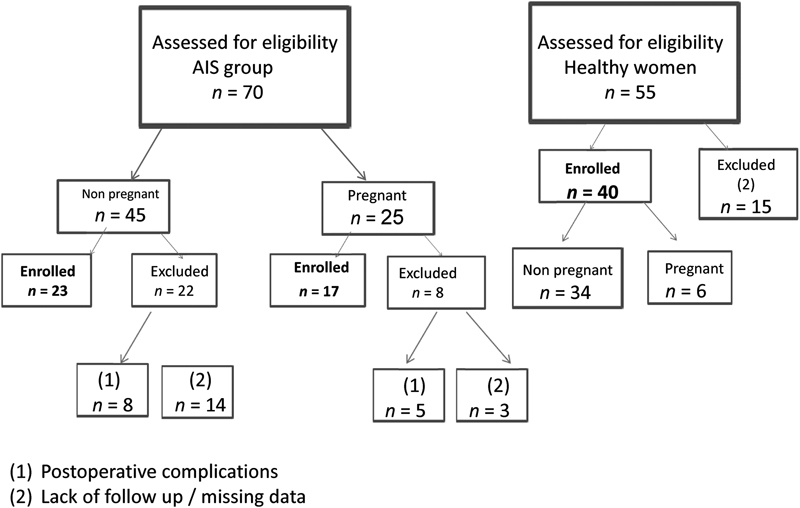
Graphic breakdown of patient population. Healthy and AIS female patients were assessed for this study. They were either enrolled, or excluded, as depicted in the figure. AIS, adolescent idiopathic scoliosis.
Inclusion Criteria
Age restriction: 18 to 40 years old
Women who have undergone surgery for AIS with a history of one or more pregnancies
Women who have undergone surgery for AIS without a history of pregnancy
Healthy women with a history of one or more pregnancies
Exclusion Criteria
Postsurgical: women who underwent surgery with postoperative complications
Nonsurgical: patients with other medical comorbidities or major spine anomalies
Clinical Evaluation
Data was collected from various sources including medical record notes, radiographic analysis reports, and information provided by women through interview.
Patient Characteristics and Risk Factors
Number of pregnancies
Age of the women in each pregnancy
Type of delivery (vaginal/cesarean section)
Type of anesthesia (neuroaxial epidural anesthesia)
Measurements of the baseline scoliosis curve using full-spine standing preoperative anteroposterior and lateral radiographs of the spine
Education (high school versus academic)
Marriage (married versus not married)
Mean degrees of surgical correction of the deformity and follow up X-rays for progression evaluation of the deformity
Radiographic Evaluation
Curve extension and magnitude were assessed using the Lenke classification by two experienced fellowship-trained spine surgeons using a consensus building method. 8 Patients were stratified according to the deformity in terms of type of curve pattern and curve magnitude determined by the Cobb method based on retrospective evaluation of full-spine standing preoperative and postoperative anteroposterior and lateral radiographs of the spine.
Clinical Outcomes
Rate of anesthetic methodology was measured by information provided through medical records (anesthesiology documentation system).
Satisfaction with surgery was measured using the Scoliosis Research Society 24 (SRS24) questionnaire for satisfaction with surgery domain.
Prevalence of back pain after delivery was reported by the study participants through yes-or-no responses.
Severity of back pain was measured with SRS24 questionnaire, with questions regarding general function or daily activities that are impaired because of back pain. There are seven questions in the pain domain, which establishes a mean pain score and indicates its severity.
Prevalence of depression was assessed using the Beck Depression Inventory score. The threshold used to diagnose women with depression was a score more than 9.
Prevalence of sexual dysfunction was assessed using the Female Sexual Distress Scale–Revised (FSDS) questionnaire. A score of 11 or greater suggests female sexual dysfunction.
Analysis Plan
The Student t test was used to compare the nonpregnant AIS group with the pregnant AIS group with respect to continuous variables (e.g., SRS scores). The chi-square test was used to compare these groups with respect to dichotomous outcomes (e.g., prevalence of back pain). Descriptive statistics were used for the healthy cross-sectional cohort.
Results
Among the 37 women enrolled in the nonpregnant AIS cohort, 14 were missing data or lacked complete follow-up, leaving 23 subjects (62%) for the analysis. From the 20 women enrolled in the pregnancy AIS cohort, 3 were missing data or lacked complete follow-up, leaving 17 subjects (85%) for the analysis. Thirty-nine pregnancies were documented in 17 women. The average age of women in the AIS group who delivered a child was 31 (range 21 to 40). The time from surgery to first pregnancy was 7.3 years (range 3 to 12 years). Compared with the general population for which the infertility rate is assumed to range between 3 and 7%, 3 patients in the AIS group had difficulty conceiving (17%) and needed to undergo fertility treatments (Table 1).
Descriptive patient characteristics of AIS pregnant and nonpregnant women
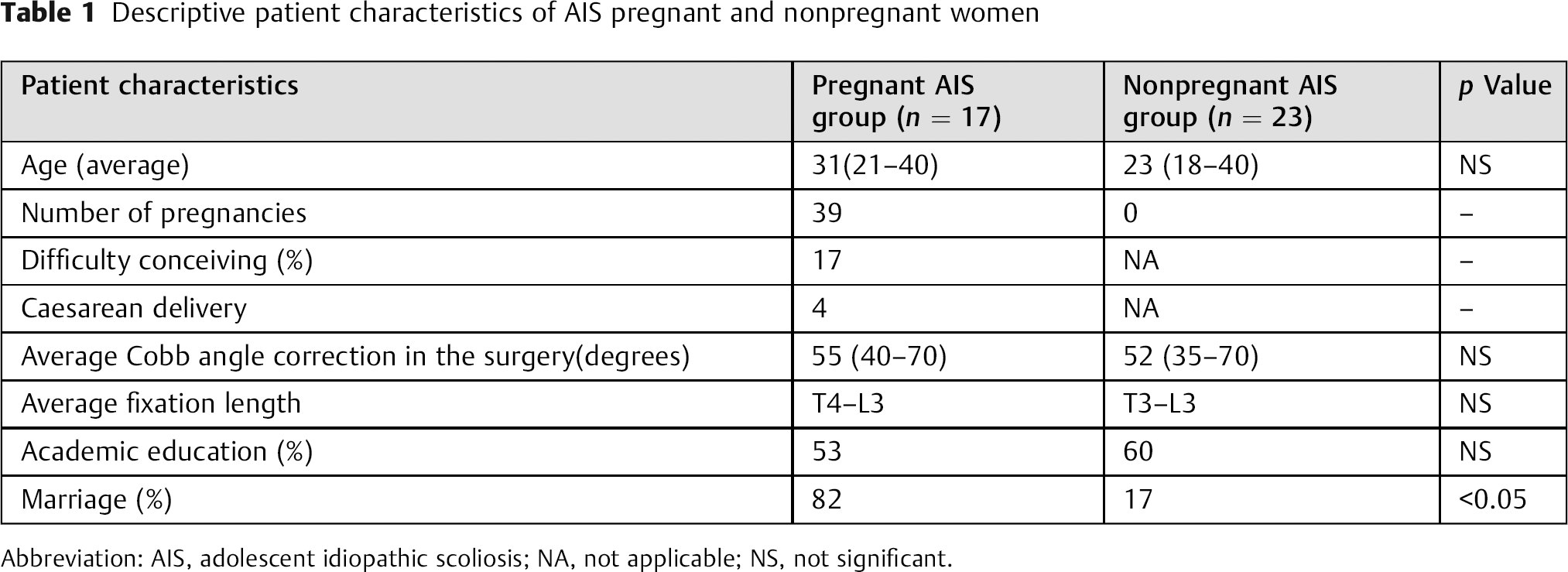
Abbreviation: AIS, adolescent idiopathic scoliosis; NA, not applicable; NS, not significant.
The rates of anesthetic techniques used among pregnant patients with AIS who underwent correction surgery with pedicle-based systems and among healthy pregnant women were as follows: 12 women (70%) in the AIS pregnant group were refused epidural anesthesia by anesthesiologists, mostly due to the perception of absence of an access site for catheter placement. The healthy pregnancy group did not encounter any refusal of epidural anesthesia.
The SRS24 questionnaire showed a satisfaction score with surgery of 3.76/5 among pregnant and nonpregnant patients with AIS who underwent correction surgery with posterior pedicle-based systems, which is comparable with general satisfaction from AIS correction surgery.
Six of the 17 of the women with AIS had severe back pain during pregnancy (35%) mandating home treatment or hospitalization, and 13 of the 17 women continued to experience sustained back pain that impacted their life after child delivery (76%). In the healthy nonscoliosis group, no back pain was attributed to pregnancy, as reflected in the SRS24 scores, which were low at 72% (88/120) and had a low score in the pain domain of 3.69/5 (p = 0.0048 when compared with nonpregnant patients with AIS; Tables 2 and 3).
Clinical characteristics of pregnancies in AIS and healthy women
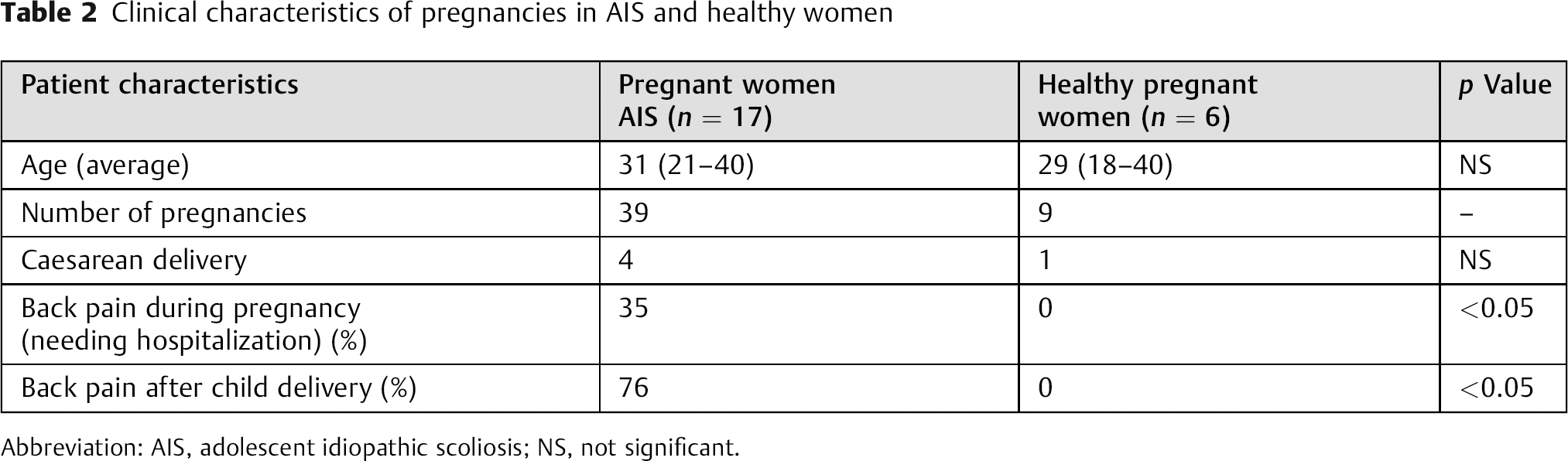
Abbreviation: AIS, adolescent idiopathic scoliosis; NS, not significant.
Outcomes of pregnancies in AIS and healthy women as assessed by questioners
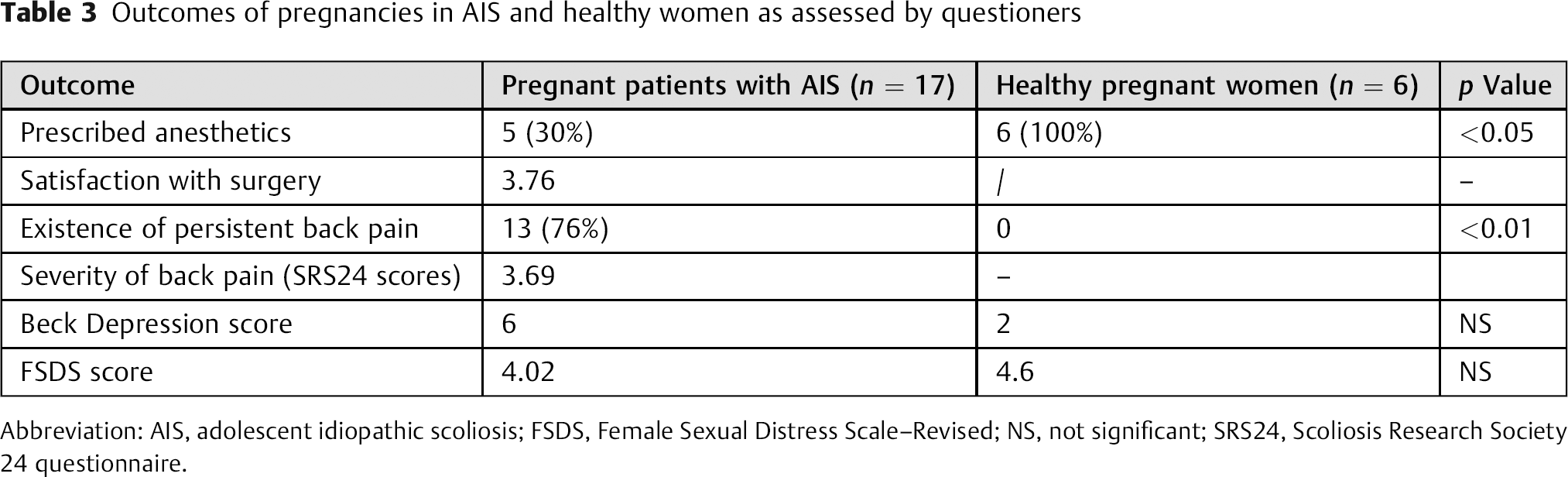
Abbreviation: AIS, adolescent idiopathic scoliosis; FSDS, Female Sexual Distress Scale–Revised; NS, not significant; SRS24, Scoliosis Research Society 24 questionnaire.
The prevalence of depression among pregnant and nonpregnant patients with AIS undergoing correction surgery with posterior pedicle-based systems and healthy woman with a history of pregnancy was in the normal range and was similar for all groups (Table 3).
In the scoliosis group, the average FSDS score was 4.02 in the pregnancy group and 5.67 in the nonpregnant group (not significant). The healthy group's score was 4.6 (not significant). These scores suggested no sexual dysfunction from scoliosis and surgical treatment as well as from pregnancy (Table 3).
Discussion
Regional anesthesia was used less often among pregnant patients with AIS who underwent correction surgery with posterior pedicle-based systems compared with healthy pregnant women. We suspect that anesthesiologists avoid spinal anesthetic techniques in patients with AIS because of concerns about potential side effects this technique. However, to investigate this hypothesis in more depth, a larger study would be required.
The pregnant group was satisfied with the surgical outcomes of their deformity correction. Moreover, recent X-rays of the women showed solid fusion, with satisfactory results.
The rate of back pain requiring care in patients with AIS was higher during pregnancy than in the general population (p < 0.05). These symptoms did not resolve over time, which resulted in decreased patient-reported outcomes scores for satisfaction with surgery. We offer several possible reasons for the incidence of sustained back pain in these patients:
Stiffness of the back as an intended outcome of spine fusion surgery
Lack of physiologic compensation, especially in regards to sagittal balance during pregnancy
Increased rates of caudal adjacent segment degeneration as part of the natural history of adjacent-level degeneration, which is accelerated by a pregnancy
Increased sacroiliac joint pain due to stress transfer induced by fusions ending at more caudal segments
Radiologic assessment failed to shed light on more specific reasons for sustained back pain in many women after and during pregnancy.
Depression among pregnant and nonpregnant patients with AIS undergoing correction surgery with pedicle-based systems and healthy woman with a history of pregnancy did not differ between the groups and therefore could not explain the difference in pain after delivery.
The sexual function of women undergoing scoliosis correction appears somewhat impaired compared with healthy controls; however, no difference was seen between women who had pregnancies and those who had none. This finding is in agreement with an earlier study by Danielsson and Nachemson, who reported that scoliosis care (bracing or surgery) leads to impaired sexual function. 9
Conclusion
Women who underwent scoliosis correction surgery suffer from an increased incidence of long-term back pain after pregnancy. A larger study on this topic seems warranted.
Disclosures
Tal Falick-Michaeli, none
Josh E. Schoeder, none
Yair Barzilay, none
Mijal Luria, none
Eyal Itzchayek, none
Leon Kaplan, none
This article was warmly received by the reviewers, who provided excellent input during the finalization of this submission. The topic is of significant interest to the public as it addresses a common problem and seeks answers to questions that are frequently intuitively answered with little or no substance to support the recommendations made. The authors tackled these questions directly in a comprehensive fashion. From a methodological basis, the study is sufficiently powered as a pilot project; the authors rightly point out larger-scale population-based studies would seem warranted. The loss to follow-up was asymmetric between the groups, thus introducing a potential for type 2 bias. In the end, the reviewers accepted that the follow-up rates were felt to be within expected generally acceptable ranges and were asymmetric due to chance and not design, but the concerns about small groups and the potential for bias introduced by unequal follow-up rates is important to note for the EBSJ readership. Variables surrounding the back pain incidence and severity as well as the surgical factors such as retained motion segments and alignment including factors such as body weight, activity levels, and other factors were not addressed in this study.
The primary hypothesis—that back pain following pregnancy is increased in patients with previous scoliosis fusions compared with nonoperatively treated patients—is a significant finding and will need to be looked into in greater detail.
Other concerns such as depression and dysfunction were either nonfactors or not of statistical significance.
An interesting finding was the observation that anesthesiologists were apparently influenced in their choice of anesthetic based on previous scoliosis fusion surgery, with much reduced rates of regional spinal or epidural anesthesia rates offered to the fusion cohort despite objective evidence to suggest adverse interference of previous AIS fusion on success of epidural anesthesia placement. This finding is very interesting in itself and begs for a more global follow-up survey with larger cohorts.
For the benefit of our readership, EBSJ would like to address potential questions pertaining to the authors’ use of the SRS24 questionnaire. This outcomes tool has been globally validated largely for patients with pediatric spinal deformity and mainly addresses concerns pertinent to patients with adolescent idiopathic scoliosis. The Scoliosis Research Society has also produced other versions (with 22, 23, and 30 questions). The SRS24 questions cover seven domains: pain, self-image before surgery, self-image after surgery, function after surgery, general function, function-activity, and satisfaction with surgery. The concern was raised if an Oswestry Disability Index questionnaire would have been more appropriate to investigate low back pain for this population. EBSJ is not aware of any comparison studies; given that this outcomes tool is well validated in several languages for an AIS population and in light of the fact that the SRS24 test includes pain and function features, EBSJ finds no compelling reason to prefer another test over the SRS24. EBSJ invites its readers to look at the SRS questionnaire portfolio firsthand by visiting the SRS website and opening the Outcomes section (https://www.srs.org/professionals/SRS_outcomes/srs-24.pdf).
In conclusion, the authors deserve praise for their work with an excellent study idea and the variety of compelling questions they raised and addressed in this pilot-type study. EBSJ hopes that future researchers across the global AO community will pick up on this study idea and seek to answer the many interesting questions surrounding the quality of life for patients with adolescent idiopathic scoliosis with increasing emphasis on the impact of surgical treatment.