
Abstract
Study design
Retrospective cohort study with a cross-sectional comparison.
Objectives
To assess sexual function and experience in adult women who had scoliotic correction for adolescent idiopathic scoliosis (AIS).
Methods
Women ages 18–40 years with a history of scoliosis, who were braced or underwent uncomplicated posterior scoliosis correction for AIS, followed for two years or more since treatment were included. Sexual function was assessed using the Female Sexual Distress Scale-Revised (FSDS-R) and the Female Sexual Function Index (FSFI) questionnaires. Participants’ scores were compared to those of a control group consisting of age-matched healthy women.
Results
Of 115 women who responded to the questionnaires, 40 (35%) had surgical treatment (mean age 25.1; range 19–35 years; mean time since surgery 8.2 years; range 3–12 years) and 35 (30%) were braced (mean age 23.3; range 18–27 years; mean time since treatment 3.6 years; range 3–5 years). The control group consisted of a cohort of 40 (35%) aged-matched healthy women. According to the FSDS-R, significantly more women with scoliotic correction for AIS reported sexual distress compared to healthy controls (25% vs 12%, respectively), and the difference in the total mean scores (7.05 vs 5.34, respectively), was significant (P < .001). Additionally, the mean overall FSFI score for scoliotic-corrected women was 24.2 (range 17.5–29.1) within the pathological range (<26.55) of sexual dysfunction.
Conclusions
High rates of sexual distress and dysfunction were reported in women with a history of AIS, thus, there appears to be long-term consequences years after deformity correction by brace or surgical correction.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS), a deforming pathology resulting in curvature of the spine, develops in adolescence, has an overall prevalence of .47–5.2%, with 2:1 female to male ratio. 1 Moreover, the severity of scoliosis is also higher in girls than in boys, which can have significant ramifications on body image, particularly stress related to disfigurement or spinal deformity might promote within the patient a negative self-image, compounded with experiencing difficulties in social interaction, due to the visibility of their condition. 2 Body image and health-related quality of life (HRQL) are complex and significant issues for AIS patients, that might continue to pose limitations on psychosocial functioning into adulthood.3,4
Negative body image has an apparent impact on sexual function, an important component of HRQL. Moreover, in women who suffered from AIS sexual function may be affected by multiple and complex physical, interpersonal, and psychological problems (as low sexual desire, low self-esteem, and feelings of being unattractive).5,6 Sexual dysfunction might be due to the pathology of the disease, including stressful memories of having a visible spinal deformity during the patient’s emotionally sensitive teenage years. Sexual dysfunction could result from the treatment (i.e., the trauma of being forced into braces at a critical stage of life); Or ensuing disability (decreased spinal flexibility, due to the fusion of the lumbar spine segments); Or the accompanying depression, or body image issues.2,7,8
Several retrospective longitudinal follow-up studies on HRQL in female AIS-braced and surgically treated patients reported similar scores in both physical and mental components.8,9 While others showed previously braced female AIS patients had significantly lower HRQL in all the subscales compared to healthy controls. 10 However, there are limited data assessing the effect of scoliosis correction on sexual function in AIS-braced and surgically treated female patients, with only few follow-up studies that reported on impaired sexual function in comparison to healthy controls.6,11
The aim of our study was to assess sexual function and experience and their possible relationship to depression in adult women with corrected AIS who A) underwent treatment with Boston Brace or Milwaukee Brace for a year or more, or B) were surgically treated with posterior pedicle fixation for the management of AIS. We evaluated the influence of depression to determine what role, if any, it had in explaining sexual dysfunction in women who had undergone scoliotic correction. The results obtained from these groups were compared with those of aged-matched healthy peers.
Material and Methods
Study Design
Retrospective cohort study with a cross-sectional comparison took place between 2012 and 2016. The study was approved by the Institutional Review Board of the University Medical Center.
Study Population
Inclusion criteria for participating in this study were: age restriction of 18–40 years; women who had been treated for AIS with either a thoraco-lumbar brace (Boston Brace) or a cervico-thoraco-lumbar-sacral brace (Milwaukee Brace) for 18 months or more, and women who underwent surgery with an all-pedicle or combined pedicle-and-hook construct specifically for the treatment of AIS were considered for enrollment in this study. Among the women who underwent surgery after exclusion, due to postoperative complications, 40 women were enrolled. Among women who underwent bracing, 35 were enrolled. For the cross-sectional cohort, this group of women were matched with 40 healthy peers of comparable age and education who served as a control group.
Clinical Evaluation
Data was retrospectively collected from patient medical records, radiographic analysis reports, and analysis of information provided by the women through validated questionnaires assessing sexual distress and sexual function and depression rates.
Radiographic Evaluation
Concerning patients who had been braced, images taken after the removal of braces and within two years of this study were evaluated for changes in the magnitude of the deformity.
In the surgical group, patients were stratified according to the degree of deformity presented prior to surgery and the degree of correction achieved. This retrospective evaluation was based on full-spine standing preoperative and postoperative anteroposterior and lateral radiographs of the spine. Curve extension and magnitude were assessed on the basis of the consensus of two experienced fellowship-trained spine surgeons using the Lenke classification. 12
Questionnaires
Several self-reporting tools developed to address body image and sexual function were used to evaluate these issues with respect to patients who have had scoliotic correction. The Female Sexual Distress Scale-Revised (FSDS-R) questionnaire, 13 a statistically validated tool used to identify women who suffer from sexual distress, and the Female Sexual Function Index (FSFI), 14 a questionnaire about sexual experiences within the last four weeks designed to target specific sexual pathology, in six domains: desire, sexual arousal, lubrication, orgasm, sexual satisfaction, pain during sexual activity. Analysis of responses to these two questionnaires were used to compare the sexual function of women previously treated for AIS with a cohort of age-matched and educationally comparable healthy peers to control for the possible influence of age and education on sexual experience. Similarly, given that depression can impact on sexual functioning, its role in impaired sexuality among women who underwent scoliotic correction was also evaluated. Depression rates were assessed using the Beck Depression Inventory. 15 Scores range from 0 to 63, with 0–9 categorized as not depressed, 10–15 as mildly depressed, 16–23 as moderately depressed, and 24–63 as severely depressed.
Certified translations of the questionnaires into Hebrew, Arabic, and Russian, the languages spoken by the study subjects, were administered by a female medical student who was not associated with the treating physician or surgeon who performed the correction of scoliosis.
Statistical Analysis
Analyses were performed using SPSS statistical software (version 18.0, SPSS/IBM, Chicago, IL, USA). The Student’s t-test, T-squared test, ANOVA, and Fisher’s exact test were used to compare the cohorts. A binary logistic regression analysis was used to identify possible predictors of sexual dysfunction in women previously treated for AIS and control subjects. Scores are presented as mean ± SD. P > .05 was defined to be statistically significant.
Results
Study Population
Of 150 patients (50 in each group) who were asked to take the questionnaire, 115 women responded, yielding a response rate (RR) of 76%. Among responders, 75 underwent treatment for AIS: 40 (35%) had undergone surgical treatment (mean age 25.1; range 19–35 years) and 35 (30%) had undergone bracing with a Boston or Milwaukee brace (mean age 23.3; range 18–27 years). For the cross-sectional cohort, 40 (35%) age-matched controls (mean age 26.7; range 18–33) were included in the study. See Figure 1-STROBE flow chart of patient’s and participant’s identification and enrollment for analysis. STROBE flow chart of patient’s and participant’s identification and enrollment for analysis.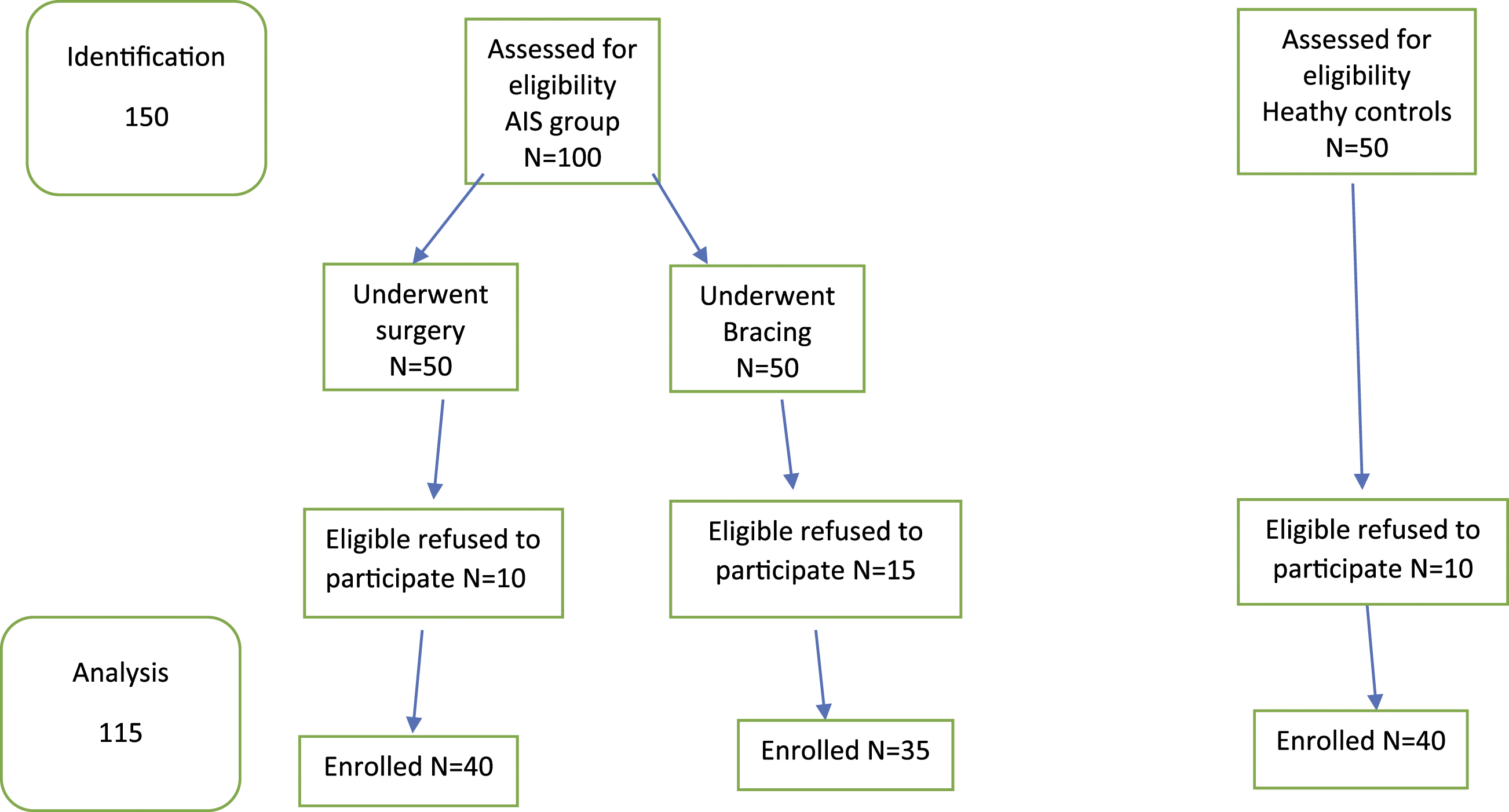
Socio-demographic characteristics of patient groups and healthy controls.

Type of Scoliosis Treatment
(A) Bracing: of the 35 AIS-treated women who had undergone bracing, 26 patients were treated with a Boston (thoraco-lumbar) Brace and 9 women were treated with a Milwaukee (cervico-thoraco-lumbar-sacral) Brace for 18–22 hours per day; Bracing was used on average for 18 months (range 12–30 months), mean time since treatment 3.6 years (range 3–5 years). Average Cobb angle at latest imaging was 34.5 degrees (range 25–40).
Post-surgical group patient clinical characteristics.
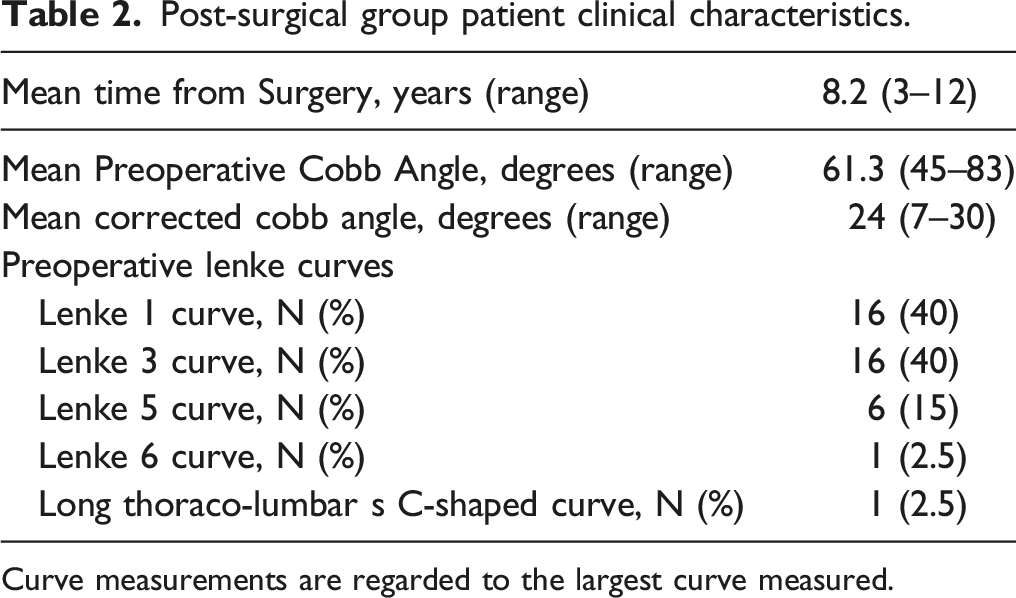
Curve measurements are regarded to the largest curve measured.
Mean Cobb angle correction following the surgery was 24 degrees (range 7˚–30˚).
The Female Sexual Distress Scale-Revised
Female Sexual Distress Scale-Revised (FSDS-R) Scores.

AIS: Adolescent idiopathic scoliosis.
The Female Sexual Function Index
The women in the AIS-treated group with a pathological score on the FSDS-R questionnaire (N = 19) were then requested to respond to the Female Sexual Function Index (FSFI) questionnaire, as the former reflects sexual distress, while the latter addresses sexual dysfunction in specific domains. The mean overall FSFI score for scoliotic-corrected women was 24.2 (range 17.5–29.1) with 10 patients scoring within the pathological range (below 26.55). In this measure, lower scores indicate worse sexual function, while women scoring below the established cut-off of 26.55 should be considered at risk for sexual dysfunction. 14
Significantly, the AIS patients responding to the questionnaire scored within the normal range for sexual desire, pain during intercourse, and lubrication. However, their scores for sexual arousal, frequency of orgasm, and satisfaction were in the pathological range.
Beck Depression Inventory
The Beck Depression Inventory, a standard tool for the measurement of depression, was applied in this study. Four women in the braced group, eight women in the post-surgical group, and three women of the control group had scores in the pathological range (>13) using this instrument. This was not a statistically significant difference. No correlation was found between scores in the pathological ranges of the FSDS-R or the FSFI questionnaires and those of the Beck Depression Innovatory. This finding suggests that sexual dysfunction in these patients was not due to depression.
Discussion
Although medical care for adolescent idiopathic scoliosis (AIS) starts at a young age, the ramifications of this condition and its management continue throughout life. There is paucity of studies on female patients with spinal conditions that assess sexual function adequately using validated questionnaires as the FSFI and FSDS. We found that according to the FSDS-R, significantly more women with scoliotic correction for AIS (25%) reported sexual distress compared to those in the healthy control group (12%) and there was a statistically significant difference in the mean score between the two groups (P < .001).
Additionally, we found the mean overall sexual dysfunction (FSFI) score of 24.2, among women with scoliotic correction for AIS, was within the pathological range (score below 26.55) pointing to risk of sexual functioning clinical disorders.
This finding is in agreement with an earlier study from 2001 by Danielsson et al. who reported in a long-term 22-year follow-up, that AIS treatment in 247 women through bracing or surgery leads to significant limitations in sexual function, in 28% and 33%, respectively, as compared to healthy controls. The major reasons reported for the impaired sexual functioning were due to physical limitations to participate in sexual activities and self-consciousness regarding appearance. 6 In a psychological evaluation follow-up study among 146 AIS female patients (mean age 33), less than 10% admitted that the illness and surgical treatment had significantly affected their current sex life. Nonetheless, the study group reported on less often engaging in sexual relations and reduced satisfaction with their sex life, as compared to a control group of age-matched healthy participants. 16 Although these earlier studies did not use validated questionnaires for the assessment of sexual function, they nevertheless opened the window on the long-term effects of AIS scoliotic correction on sexuality.
Conversely, a study among previously braced female AIS patients assessed sexual function using the FSFI observed on average the absence of sexual dysfunction among 36 AIS patients of similar age to our cohort, albeit comparable to our results they also assessed sexual arousal poorly and 15% of women with Cobb angle <30˚ scored within the pathological range. 11
Although AIS treatment had been completed relatively early in life, judging from the high rate of sexual distress and dysfunction in women with a history of AIS, there appears to be long-term consequences well after correction of the deformity. The AIS-treated women in the current study had normal scores on the FSFI assessment with regard to pain during intercourse and lubrication, possibly indicating that their sexual function is not impaired by physical dysfunction, but seemingly by psychological factors that affect sexual arousal, orgasm and sexual satisfaction, domains with scores in the pathological range.
Moreover, these may be related to body image issues, which have been shown to trouble women with scoliotic correction for AIS and that are also important factors in sexual satisfaction. 17 A 23-year follow-up study assessed self-perceptions of body image in 30 braced AIS female patients, (mean age 41), almost half reported to experience moderate stress related to body disfigurement or severe stress concerning body deformity, corresponding to HRQL rating with worst scores in the self-image sub-scale. 2
Surgery is typically associated with improvement of self-image and body image, as demonstrated in a study of 157 adult AIS-braced and surgically treated patients who reported on their body image as positive (8% vs 27%, respectively), neutral (42% vs 40%, respectively), or negative (50% vs 33%, respectively). 18
Our results show no difference between women treated with bracing or surgically for AIS with regard to rate of sexual dysfunction (25%), which is consistent with the findings in patients with other spinal conditions, who suffer from impaired sexual function. Several longitudinal follow-up studies addressed sexual function using the FSFI among traumatic spinal cord injury female patients. Similar to our findings, in a Scandinavian study among 532 women following spinal cord injury, more than half reported on difficulties becoming sexually aroused, reduced sexual desire, never or seldom reaching orgasm, and less than half were satisfied with their sex life. Psychological problems as low self-esteem and feelings of being unattractive were mentioned as obstacles to overcome these sexual function impairments. 19 While in a German study similar to our cohort, the majority of women reported no problems with impaired vaginal lubrication, however, as opposed to our results, the majority also reported being satisfied with their sexual life, especially those who were younger at the time of injury. 20 A study of 39 female patients following severe spinal cord injury reported on decreased sexual activity compared to healthy controls, yet demonstrated similar levels of sexual desire and satisfaction, but lower scores on the FSFI on components of orgasm and lubrication. 21
A recent study reported on worsened sexual function in the postoperative period following cervical spine surgery in 39% of the female patients. Moreover, the average FSFI score pointed to sexual dysfunction in 82% of the female patients, with lower scores in women treated for depression. 22 Indeed, depression is a major cause of sexual dysfunction, 23 yet in the current study, it was not shown to be significantly correlated with the incidence of sexual dysfunction in women who had been treated for AIS, corresponding to results from our previous study in AIS surgically treated females. 24
Limitations
Generalizability of this study is limited by its small number of participants. Nonetheless, a significant difference was found in the level of both sexual distress and dysfunction described by the women with scoliotic correction for AIS relative to their healthy peers.
Conclusions
Our study concludes that female AIS patients who had undergone bracing or surgical scoliotic correction can suffer from sexual distress and dysfunction, with decreased sexual satisfaction, less frequent orgasm, and decreased sexual arousal many years after the end of treatment.
Although AIS treatment had been completed relatively early in life, high rates of sexual distress and dysfunction were reported in women with a history of AIS, thus there appears to be long-term consequences well after correction of the deformity. Further research based on a larger sample of patients is needed to establish how representative these results are with respect to AIS-treated women and whether similar effects are seen in males who had scoliotic correction for AIS. Further study is warranted to identify the exact cause of the sexual dysfunction, specifically whether it is a function of somatic or psychological factors or a combination of both.
Footnotes
Author Contributions
The authors express their gratitude to Ms. Dalia Dawn Orkin for her English language contributions and editing services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval
There was IRB approval for the study – Number G125946.