
Abstract
Study Design
Prospective cohort study.
Objective
To clarify long-term surgical outcomes of C3–6 laminoplasty preserving muscles attached to the C2 and C7 spinous processes in patients with cervical spondylotic myelopathy (CSM).
Methods
Twenty patients who underwent C3–6 open-door laminoplasty for CSM and who were followed for 8 to 10 years were included in this study. Myelopathic symptoms were assessed using Japanese Orthopaedic Association (JOA) score. Axial neck pain was graded as severe, moderate, or mild. C2–7 angle was measured using lateral radiographs of the cervical spine before surgery and at final follow-up.
Results
Mean JOA score before surgery (11.7) was significantly improved to 15.2 at the time of maximum recovery (1 year after surgery), declining slightly to 14.9 by the latest follow-up. Late deterioration of JOA score developed in eight patients, but was unrelated to the cervical spine lesions in each case. No patient suffered from prolonged postoperative axial neck pain at final follow-up. The mean C2–7 angle before surgery (13.8 degrees) significantly increased to 19.2 degrees at final follow-up.
Conclusions
C3–6 laminoplasty preserving muscles attached to the C2 and C7 spinous processes in patients with CSM maintained satisfactory long-term neurologic improvement with significantly reduced frequencies of prolonged postoperative axial neck pain and loss of C2–7 angle after surgery.
Keywords
Introduction
Some problems can be associated with cervical laminoplasty such as axial neck pain and deterioration of sagittal alignment of the cervical spine 1 ; we have previously reported that C3–6 laminoplasty preserving muscles attached to the C2 and C7 spinous processes can significantly reduce the incidence of postoperative axial neck pain and kyphotic deformity in the short term. 2 , 3 , 4 Moreover, our prospective 5-year follow-up study revealed that our C3–6 laminoplasty can maintain satisfactory neurologic recovery with significantly decreased frequencies of postoperative prolonged axial neck pain and loss of cervical lordosis in the medium term. 5 However, a major concern for C3–6 laminoplasty is whether it can maintain neurologic recovery over a long period. In addition, we must also examine whether the preservation of muscles attached to the C2 and C7 spinous processes can maintain reduced frequencies of postoperative axial neck pain and kyphotic deformity over a long period. Therefore, we conducted further follow-up study (average 9-year follow-up) to clarify the long-term surgical outcomes of C3–6 laminoplasty in patients with cervical spondylotic myelopathy (CSM).
Materials and Methods
Most patients at Osaka University Hospital with cervical stenotic myelopathy have been treated using C3–6 open-door laminoplasty since September 2002, except for patients with cervical kyphosis ≥ 15 degrees, single-level anterior lesion without narrow spinal canal, or spinal cord compression at the C7 and/or caudal levels. Based on our criteria, only three patients with CSM underwent C3–7 or C3–T1 laminoplasty and 26 patients with CSM underwent our original C3–6 laminoplasty between September 2002 and December 2004. Our original C3–6 open-door laminoplasty preserving muscles attached to the C2 and C7 spinous processes represents a modification of the previously described unilateral-opening laminoplasty. 2 , 6 For the first 2 weeks after surgery, all patients wore a soft collar. Twenty (15 men, 5 women) of the 26 patients who underwent C3–6 laminoplasty for CSM have been followed for ≥8 years and were included in this study (follow-up rate = 76.9%). The remaining 6 patients were lost to follow-up; 1 patient died because of reasons unrelated to cervical spine lesions; 3 patients relocated; 2 patients were lost to follow-up due to unknown reasons. Mean age of the 20 patients at surgery was 61.2 years (range, 36 to 87 years; Table 1). Mean follow-up period was 9.0 years (range, 8 to 10 years; Table 1).
Demographic, clinical, and radiographic data in each patient
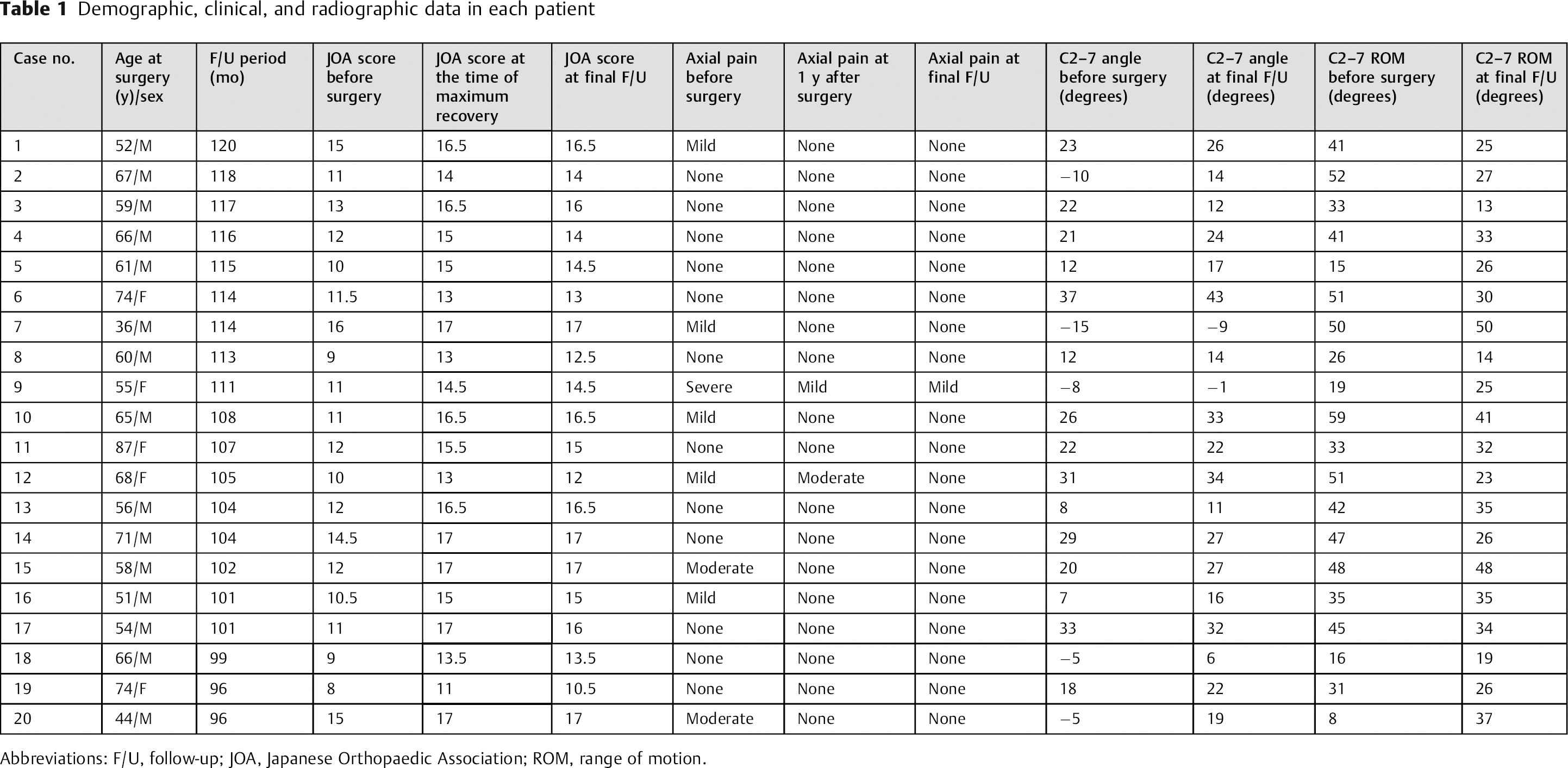
Abbreviations: F/U, follow-up; JOA, Japanese Orthopaedic Association; ROM, range of motion.
All 20 patients underwent follow-up examinations every 3 months for the first 1 year after surgery, and every 1 year thereafter. Myelopathic symptoms were assessed using the Japanese Orthopaedic Association (JOA) score 7 and recovery rate. 8 In patients who developed late deterioration of JOA score during postoperative follow-up, causes of deterioration were investigated.
Flexion, neutral, and extension lateral radiographs of the cervical spine were assessed before surgery and at final follow-up. The C2–7 angle was measured as sagittal alignment of the cervical spine. The C2–7 angle is formed by two lines drawn parallel to the posterior margin of the C2 or C7 vertebral body on a radiograph in the neutral position (Fig. 1). Kyphosis was defined as C2–7 angle ≤ −10 degrees, lordosis as C2–7 angle ≥ 10 degrees, and straight as −10 to < 10 degrees. C2–7 range of motion (ROM) of the cervical spine was calculated by subtracting flexion C2–7 angle from extension C2–7 angle.
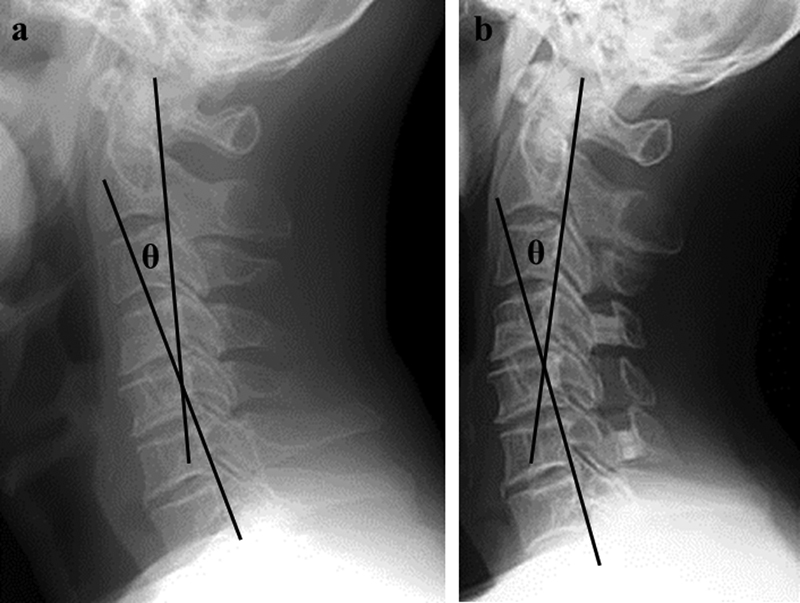
C2–7 angle (θ) was measured as sagittal alignment of the cervical spine. (a) Before surgery, (b) at the latest follow-up.
Postoperative axial neck pain was defined as posterior neck and/or periscapular pain that developed or became aggravated after surgery. According to our previous reports, 2 , 3 , 4 , 5 , 6 pain intensity was graded as severe (painkillers or local injection needed regularly), moderate (physiotherapy or compress needed regularly), or mild (no treatment needed). Severe or moderate pain after surgery was considered to constitute postoperative axial neck pain.
The paired t test, Friedman test, Wilcoxon signed-rank test (with Bonferroni correction), and Fisher exact probability test were applied for statistical analyses using JMP version 5.0.1 software (SAS Institute, Cary, North Carolina, United States), as appropriate. Values of p < 0.05 were considered to indicate statistical significance.
The protocol of this prospective long-term follow-up study was approved by the institutional review board of the hospital, and written informed consent was obtained from all participants.
Results
Myelopathic Symptoms
The mean JOA score ( ± standard deviation) improved significantly from 11.7 ± 2.1 before surgery to 15.2 ± 1.8 at the time of maximum recovery (at 1 year postoperatively; mean recovery rate, 71.7 ± 23.8%), declining slightly to 14.9 ± 1.9 (mean recovery rate, 67.1 ± 25.4%) by final follow-up (Fig. 2, Table 1).
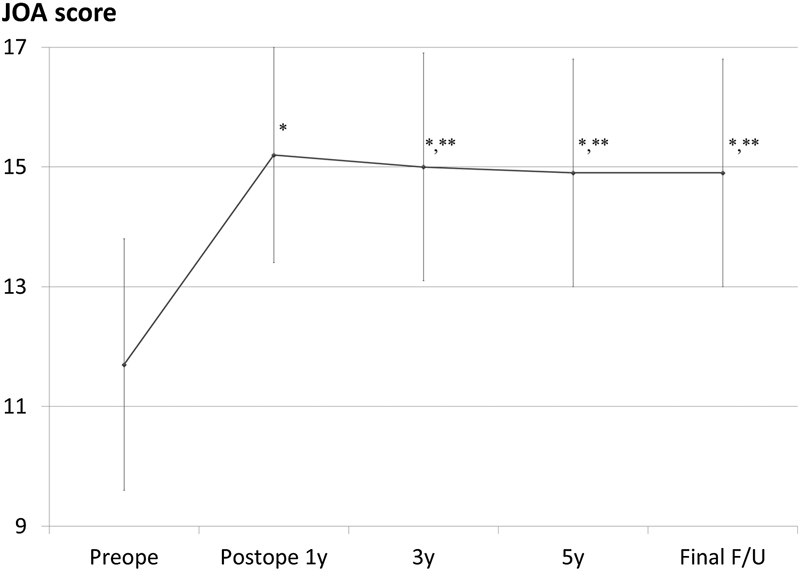
Changes in mean Japanese Orthopaedic Association (JOA) score over time. Bars indicate standard deviations. Mean JOA score peaked at 1 year after surgery. Thereafter, mean JOA score slightly decreased by 5 years postoperatively and was maintained by final follow-up (F/U). *Significantly higher than before surgery (Wilcoxon signed-rank test with Bonferroni correction, p = 0.0001). **Not significantly lower than at the time of maximum recovery (Wilcoxon signed-rank test with Bonferroni correction, p = 0.03).
Eight of the 20 patients had JOA score decreased by ≥0.5 point from the score at maximum recovery by final follow-up (Table 1). In all 8 patients, late deterioration of the JOA score was unrelated to cervical spine lesions. Causes of late deterioration were as followings: lumbar spinal canal stenosis in 4 patients; osteoarthritis of the knee in 2; carpal tunnel syndrome in 1; and stress urinary incontinence in 1. We did not encounter any cases of symptomatic adjacent-level degeneration.
Radiographic Outcomes
The mean C2–7 angle (± standard deviation) increased significantly from 13.8 ± 15.8 degrees preoperatively to 19.2 ± 13.0 degrees at final follow-up (p = 0.005, Table 1). None of the 20 patients developed postoperative kyphotic deformity. Mean C2–7 ROM reduced significantly from 37.2 ± 14.3 degrees before surgery to 30.0 ± 9.7 degrees at final follow-up (p = 0.03, Table 1).
Axial Neck Pain
Only 1 patient (5%) suffered from aggravated axial neck pain at 1 year after surgery (Table 1). However, none of the 20 patient complained of postoperative prolonged axial neck pain at final follow-up (Table 1).
Discussion
To prevent several surgery-associated problems such as axial neck pain and loss of cervical lordosis, less-invasive selective laminoplasty has been recently applied to reduce damage to the paraspinal muscles and nuchal ligaments. 9 , 10 , 11 , 12 Regarding surgical outcomes of selective laminoplasty for CSM, no significant difference in JOA score was reported between a C3–6 laminoplasty group and a C3–7 group both before surgery and at 2 years after surgery. 9 More selective laminoplasty for CSM was reported to show equal neurologic improvement at 2 years after surgery, compared with conventional C3–7 laminoplasty. 10 Moreover, our prospective 5-year follow-up study revealed that our C3–6 laminoplasty can maintain satisfactory neurologic recovery in the medium term. 5 Conversely, there has been only one report of long-term outcomes of C3–6 laminoplasty for CSM. 12 A study with a mean follow-up of 9.6 years showed that none of the 42 patients developed late neurologic deterioration resulting from cervical spine lesions after C3–6 laminoplasty. 12 However, this was a retrospective study. This is the first prospective study reporting long-term (average 9.0 years) surgical outcomes of C3–6 laminoplasty for CSM.
In the present study, mean JOA score improved significantly from 11.7 before surgery to 15.2 at the time of maximum recovery (mean recovery rate, 71.7%), declining slightly to 14.9 (mean recovery rate, 67.1) by final follow-up. Eight of the 20 patients had a JOA score decreased by ≥0.5 point from the score at maximum recovery by final follow-up, but late deterioration of JOA score was unrelated to the cervical spine in each case. In patients with CSM, the prevalence of spinal cord compression at the C6/7 level is relatively low. 13 , 14 Given these results, we conclude that the risk of late neurologic deterioration resulting from the caudal adjacent segment degeneration after C3–6 laminoplasty may be reduced. Taken all together, our C3–6 laminoplasty for CSM maintained satisfactory neurologic improvement in the long term.
After conventional (no sparing of muscle insertions) C3–7 laminoplasty, loss of C2–7 angle has been reported to reach 6.2 to 11.7 degrees. 15 , 16 , 17 Kyphotic deformity often develops after laminectomy from C1 or C2 to the subaxial cervical spine. 18 Biomechanical analysis showed that the semispinalis cervicis and C2 lamina play an important role in dynamically stabilizing the cervical spine and that a loss of cervical lordosis results from detachment of the semispinalis attached to the C2 spinous process, 19 suggesting that a loss of cervical lordosis after laminoplasty mainly results from detachment of muscles attached to the C2 spinous process. 15 However, it has been recently reported that preservation of muscles attached to the C2 spinous process can reduce loss of lordosis of the cervical spine after laminoplasty. 20 , 21 , 22 We also reported that sagittal alignment of the cervical spine at 5 years after our C3–6 laminoplasty was more lordotic than before surgery. 5 In this follow-up study, muscle attachments to the C2 spinous process were preserved in all 20 patients. As a result, the mean C2–7 angle increased significantly from 13.8 degrees before surgery to 19.2 degrees at final follow-up, and no patient developed postoperative kyphosis according to our classification. The results in this study indicate that preservation of muscles attached to the C2 spinous process plays a significant role in maintaining cervical lordosis over a long period (8 to 10 years) after laminoplasty.
Our C3–6 laminoplasty preserving muscles attached to the C7 spinous process can significantly reduce frequency of postoperative axial neck pain in the short term, 2 , 3 , 4 and this was maintained for 5 years after surgery (the incidence of axial neck pain persisting for 5 years postoperatively was 3.2%). 5 A cadaveric study showed that C3–6 laminoplasty without dissection of muscles attached to the C7 spinous process preserves more muscles such as the trapezius and the rhomboideus minor and major than conventional C3–7 laminoplasty. 23 Clinically, the intensity of postoperative axial neck pain increases in the upright position and decreases in the supine position. Given this clinical characteristic, when these shoulder suspensory muscles are injured by surgical exposure of the C7 spinous process, downward displacement of the upper extremities in the upright position seems to induce axial neck pain. Similar results supporting this were recently reported. 9 In this long-term follow-up study, only 1 patient (5%) had aggravated axial neck pain at 1 year after surgery, and no patient complained of postoperative prolonged axial neck pain at final follow-up. We reported that 10 (30%) of the 33 patients who underwent C3–7 laminoplasty had severe or moderate axial neck pain persisting for 1 year after surgery. 3 There was a significant difference in the frequency of axial neck pain between our patients undergoing C3–7 laminoplasty and those who underwent C3–6 procedure in this study (10/33 versus 1/20, p < 0.05). We conclude that our C3–6 laminoplasty preserving muscles attached to the C7 spinous process significantly reduces the frequency of axial neck pain at 1 year postoperatively and that the frequency of prolonged axial neck pain was further reduced at an average of 9 years after surgery.
In conclusion, compared with surgical outcomes in our previous 5-year follow-up study, 5 this further follow-up prospective study showed that our C3–6 laminoplasty preserving muscles attached to the C2 and C7 spinous processes in patients with CSM maintained satisfactory long-term neurologic improvement with significantly reduced frequencies of prolonged postoperative axial neck pain and loss of C2–7 angle for 8 to 10 years after surgery.
Disclosures
Hironobu Sakaura, None
Noboru Hosono, None
Yoshihiro Mukai, None
Motoki Iwasaki, None
Hideki Yoshikawa, None