
Abstract
Controversy exists regarding the timing and outcome of surgery for lumbar degenerative disease (LDD) associated with foot drop. In this work, we report the results of a retrospective observational study from our center. We had a sample size of 26 patients with a minimum follow-up of 6 months. Of the 26 patients, 88% improved, with complete recovery observed in 61%. Thus, our data support the view that there is good recovery from operative management of foot drop secondary to LDD. Adjusting for preoperative strength, preoperative duration of weakness was a significant predictor of extent of recovery (odds ratio = 0.93; 95% confidence interval 0.88 to 0.98; p = 0.019). The model explained 50% of the variance in outcome in this study.
Antigravity weakness of the tibialis anterior muscle, commonly known as a foot drop, is a common debilitating condition secondary to lumbar nerve root deficiency, and one of the causes is compression or inflammation due to stenosis (either from bone spurs, ligamentum flavum, facet cysts, or a herniated disc). Controversy exists regarding the appropriate management of this condition with equal proponents of surgical and nonsurgical treatment. The indication, timing, and benefit of surgery for foot drop remain debatable. In lack of a randomized controlled trial (RCT), the current literature that decribes the management of these patients is based on small observational case series. These studies have indicated that age, pathology, level of neural involvement, and duration and severity of foot drop are possible predictors of outcome. But there is a lack of consensus among the findings of these studies.
In this article, we report the results of a retrospective analysis of surgically managed foot drop cases in our institution with a view to assess the two clinically important areas—the extent of recovery of muscular weakness and the factors influencing outcome after surgical decompression—thereby adding to the current body of evidence. 1 , 2 , 3 , 4
Materials and Methods
This is a retrospective cohort study whereby all patients who underwent surgery for foot drop between January 2004 and December 2007 at the Neurosurgical Department of a single teaching hospital in the United Kingdom were included. Cases were identified using theater logbooks and electronic operative database. Case notes, radiological reports, and operative findings were reviewed for all patients. Demographic details, pathology, level of neural involvement, presence of radicular symptoms, bowel or bladder involvement, size of the herniated disc reported as per the magnetic resonance scan and operation notes, preoperative duration of foot drop or tibialis anterior weakness reported by the patient, preoperative tibialis anterior strength defined as per the Medical Research Council (MRC) Scale, and change in muscle strength postoperatively and at last follow-up were recorded. For purpose of inclusion in the study, foot drop was defined as weakness of tibialis anterior of MRC grade 3 or less. In case of any discrepancy in documentation of muscle strength, the one recorded by the senior member of the team was selected.
Cases with causes other than lumbar degenerative disease as well as those with follow-up less than 6 months were excluded from the analysis.
The extent of recovery was evaluated by comparing the difference between preoperative muscle weakness and muscular strength at the last follow-up. This was analyzed as complete recovery, some improvement, no change, and deterioration, for purpose of analysis. The preoperative duration of symptoms was divided into <4 weeks, 4 to 6 weeks and >6 weeks as these times have been reported to influence outcome in previous studies.
Logistic regression was undertaken to assess the influence of severity and duration of preoperative weakness on muscle recovery. Statistical analysis was performed using SPSS version 14.
Results
A total of 36 cases were identified from operative database, of which 26 met the inclusion criteria. Of these, there were 15 men and 11 women. The average age at presentation was 48 years (range 20 to 74 years). Twenty-three patients had surgery for prolapsed intervertebral disc, and three patients had surgery for lateral recess stenosis. L4–5 was the operated level in 21 (82%) patients, with L5–S1 implicated in five. None of the patients had two-level disease involvement. Eighty percent of the patients with disc prolapse had a moderate-sized disc (i.e., occupying 25 to 50% of canal diameter. Seventy percent of patients had duration of symptoms of less than 4 weeks (range 0 to 23); of these, nine presented acutely. All patients had radicular symptoms. The left side was involved in 14 patients, the right side in 11, and one patient had bilateral sciatica. Four patients had symptoms of cauda equina compression at presentation. The decision to operate was made because of neurological deficit with radicular pain in all patients after an informed discussion regarding alternative treatment. The distribution of preoperative severity and duration of foot drop is demonstrated in Fig. 1. Microdiscectomy with or without laminectomy was undertaken, achieving a satisfactory decompression in all cases as per the operation note.
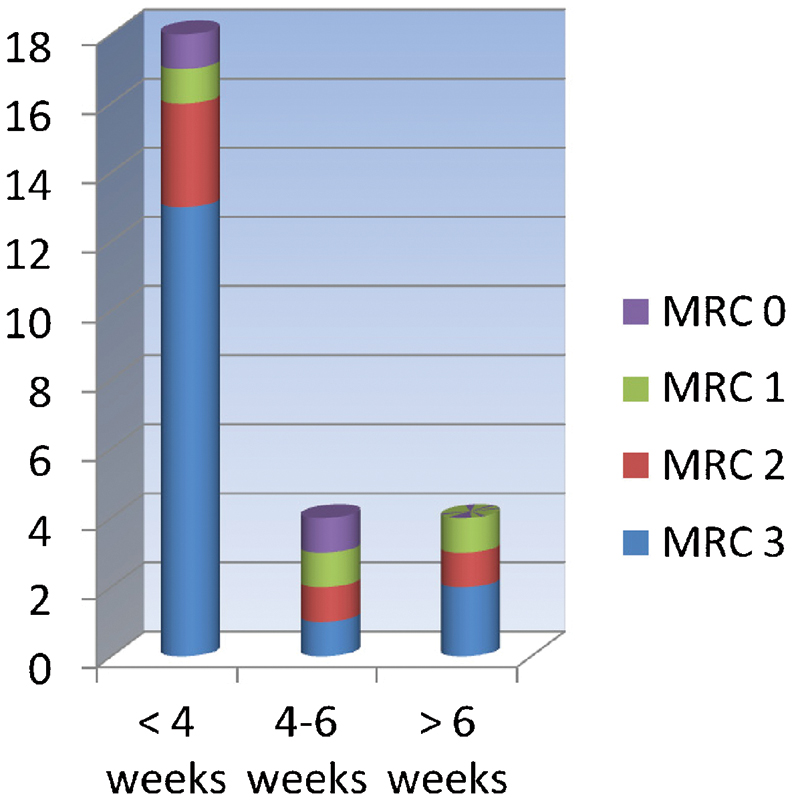
Preoperative duration and severity of foot drop.
Postoperatively, 16 (61%) patients made a complete recovery, 7 (27%) patients were improved, and 3 (12%) patients remained unchanged (Fig. 2). No patient had worsening of muscle weakness after the surgery. As there were only two patients above the age of 65 years and three patients with lumbar canal stenosis, analysis for age and pathology as prognostic factors was not possible. However, it was noted that all patients with lumbar canal stenosis in this study made a complete recovery.
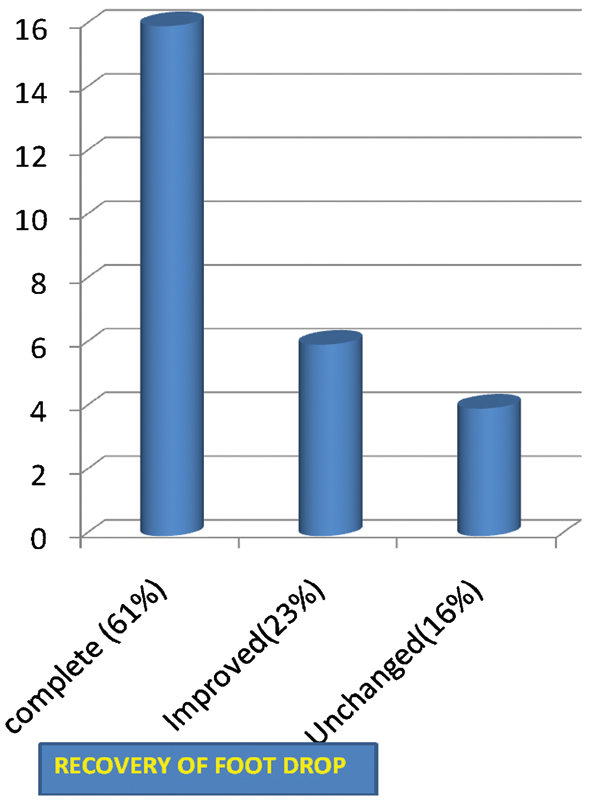
Recovery of foot drop.
All patients who recovered completely had a preoperative weakness of tibialis anterior for less than 4 weeks. Sixteen of 18 patients with symptoms for less than 4 weeks made a complete recovery, although those with longer duration fared worse. The mean duration of symptoms in patients making complete recovery was 1.1 weeks; in those with some improvement, it was 5.6 weeks; and in those with no improvement, it was 18.3 weeks (Fig. 3). We found greater preoperative muscle strength more likely to be associated with improved outcome (Fig. 4). However, patients with severe weakness of a shorter duration could make a good recovery.
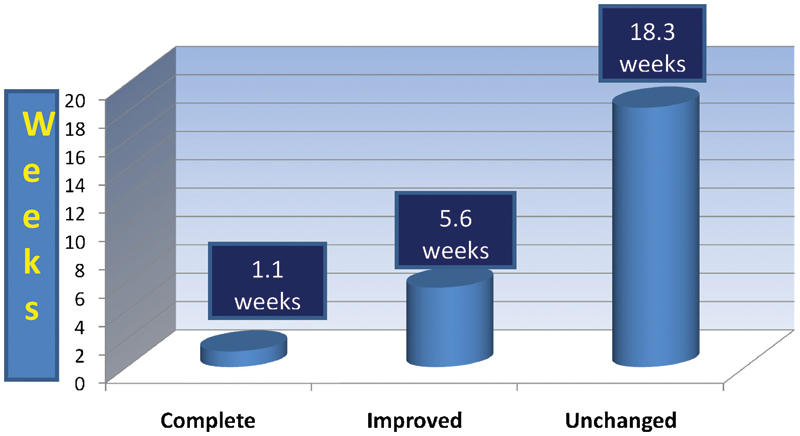
Duration of foot drop.
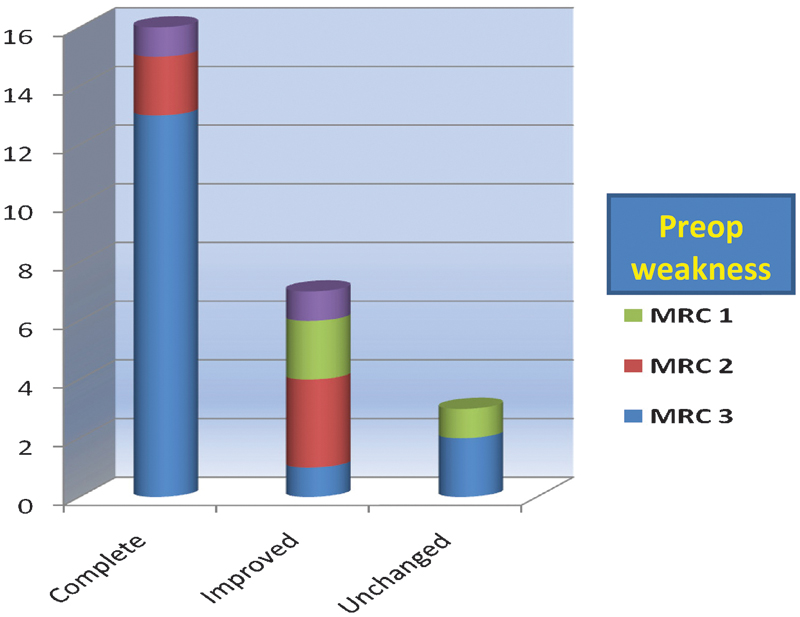
Postoperative recovery of foot drop.
Adjusting for preoperative strength, preoperative duration of weakness was a significant predictor of extent of recovery (Table 1; odds ratio = 0.93; 95% confidence interval = 0.88 to 0.98; p = 0.019), and the model explained 50% of the variance in outcome.
Factors Predicting Postoperative Recovery of Tibialis Anterior Strength at 6 Months

R2 = 0.49. OR, odds ratio; Std. Err., standard error; CI, confidence interval.
Recovery of tibialis anterior strength at 6 months.
Discussion
Similar studies have been performed before; however, recovery rates at different centers have varied after surgical procedure. One of the aims of this study was to derive recovery rates specific for a standard National Health Service setup and patient population. We found that in our study, the recovery rates were 88% with 61% or patients making a complete recovery. This was comparable to other studies where recovery rates between 61% and 84% have been reported. 5 , 6 , 7 , 8 , 9 , 10 , 11
The other aim of the study was identification of prognostic indicators. Although Girardi et al 6 identified no statistically significant prognosticators, Aono et al 8 and Postacchini et al 7 found an association between preoperative severity of weakness and duration of foot drop. Additionally, Guigui et al 10 found age < 65 years, diagnosis (stenosis versus herniated nucleus pulposus), monoradicular involvement, and duration < 6 weeks to be associated with better recovery; they did not identify any influence of severity of weakness on recovery. On the other hand, Iizuka et al 12 found diagnosis and strength to be associated with recovery but not duration.
One of the other reasons for differences observed in outcome lies in the pathogenesis of disease itself. Foot drop occurring secondary to acute compression is likely to benefit from decompressive surgery; inflammation of the affected nerve root will not. Reversal of foot drop depends on the time it takes for the nerve to recover once the irritant/compressive lesion has been dealt with. The perceived benefit from treatment also depends on patient factors as described in the recent study by Pearson et al. 13 Nevertheless, these factors should be common in all studies and patient populations.
One could identify other basic differences in the literature, possibly offering an explanation for the conflicting conclusions observed—the definition of foot drop, muscular paresis, and paralysis; the way in which muscle strength was measured; gradation of weakness; time intervals chosen; age groups and populations studied; and pathological diagnoses.
For this study, we collected data for all the variables enlisted above. We used the internationally accepted MRC grading for assessment of weakness and defined foot drop precisely as weakness ≤ MRC grade 3. We chose time interval <4, 4 to 6, and >6 weeks as these are relevant in clinical decision making and have previously been shown to be prognostically important. As clinically significant recovery of muscle strength has been reported up to 6 months postoperatively, we included only those patients where a minimum follow-up for this duration was available and considered the MRC score at last follow-up as against the one immediately postoperative. We chose 65 years as the cutoff age for comparison as per current evidence. However, as previously described, we had only two patients aged over 65 years, three with stenosis, and none with polyradicular involvement. As such for purposes of analysis, especially in view of small overall sample size, we decided to omit these factors. As a result, we concentrated on two issues: preoperative strength and duration of weakness.
Duration of weakness was a significant predictor for recovery in our data. From the literature, only Iizuka et al 7 did not find duration to be important, but it is important to note that in their study, patients were treated very rapidly, the duration of weakness for all patients with herniated nucleus pulposus was less than 6 weeks, and only three patients had duration between 4 and 6 weeks, thus offering a potential explanation for this discrepancy.
However, the duration of weakness predicted recovery adjusting for the level of motor weakness. This is important as ours as well as previous studies have reflected that preoperative strength influences outcome, and if this is not adjusted for, bias is likely. At the same time, the converse is not true. Especially, we did observe findings similar to Postacchini et al, 7 who found gradations of strength to be associated with extent of recovery in mild and moderate weakness, but patients with severe weakness could also make a complete recovery.
Conclusion
In accordance with literature, our data revealed a good recovery rate for operative management of foot drop secondary to lumbar degenerative disease. We found, adjusting for preoperative muscle strength, duration of preoperative weakness was significantly associated with extent of recovery. We admit, however, that the results of this study, as any other in current literature, have to be interpreted with caution as the small number of patients per study could potentially lead to over- and underestimation of the effect of a given variable or a combination of variables. Documentation of the outcome of unoperated cases would reduce such bias; because our current records only extend to operated cases, this was not possible.
With given constraints for conducting an RCT, we recommend meta-analysis of existing literature to provide for more informed decision making in this regard. Inclusion of historic controls and data reflecting outcomes of unoperated patients will form a valuable part of this meta-analysis. At our center, we are currently in process for organizing the same.
Disclosures
Deepti Bhargava, None
Priyank Sinha, None
Saurabh Odak, None
Atul Tyagi, None
Gerry Towns, None
Debasish Pal, None