
Abstract
A 26-year-old man with Marfan's syndrome had postural headache. Brain MRI with gadolinium showed diffuse pachymeningeal enhancement. MRI myelography revealed bilateral multiple large meningeal diverticula at sacral nerve roots level. He was suspected to have spontaneous intracranial hypotension syndrome. Eight days later headache improved with bed rest and hydration. One month after the onset he was asymptomatic and 3 months later brain MRI showed no evidence of diffuse pachymeningeal enhancement. The 1-year follow-up revealed no neurological abnormalities. The intracranial hypotension syndrome likely resulted from a CSF leak from one of the meningeal diverticula. In conclusion patients with spinal meningeal diverticula (frequently seen in Marfan's syndrome) might be at increased risk of developing CSF leaks, possibly secondary to Valsalva maneuver or minor unrecognizedtrauma.
Introduction
Marfan's syndrome is an inherited disorder of connective tissue, transmitted as an autosomal dominant trait, resulting in muscle-skeletal, ocular, and cardiovascular abnormalities. Marfan's syndrome is not generally associated to a specific type of headache. Recently, however, postural headache and spinal meningeal abnormalities have been described in two patients with Marfan's syndrome and in patients with connective tissue disorders (1–4). We present a case of a patient with Marfan's syndrome and spinal meningeal diverticula suffering from postural headache. We suggest a possible pathophysiological mechanism of postural headache.
Case report
A 26-year-old-man was admitted to the hospital because of throbbing frontal headache started 10 days earlier, soon after vomiting during a migraine attack. The headache was resistant to any analgesic medication and started within 15 min by standing up and improved or disappeared 30 min after lying down.
The patient was diagnosed with Marfan's syndrome at the age of 15 years; his parents were not related and a great-grandfather from the mother side showed a marfanoid habitus. At 18 years of age he underwent to aortic valve replacement for aortic valvular insufficiency and coronary-aortic bypass for right coronary artery occlusion; at that time he was put on oral anticoagulant therapy (INR range 3–4.5).
At the age of 20 years he started to complain of migraine with aura. The patient's migraine meets the IHS diagnostic criteria; the aura was consisting of transient visual symptoms (scintillating scotoma on the right side of the visual field) lasting about 15 min followed by left temporo-parietal moderate to severe headache lasting about 24 h associated with neurovegetative symptoms. At the age of 24 years he had spontaneous pneumothorax treated with apical lung resection.
On examination he showed a typical marfanoid habitus with tall stature (195 cm), arachnodactyly, pectus excavatum, joint hyperextensibylity. There were no neurological abnormalities. Blood examination was normal except for INR 4.02 (the patient was on anticoagulant therapy).
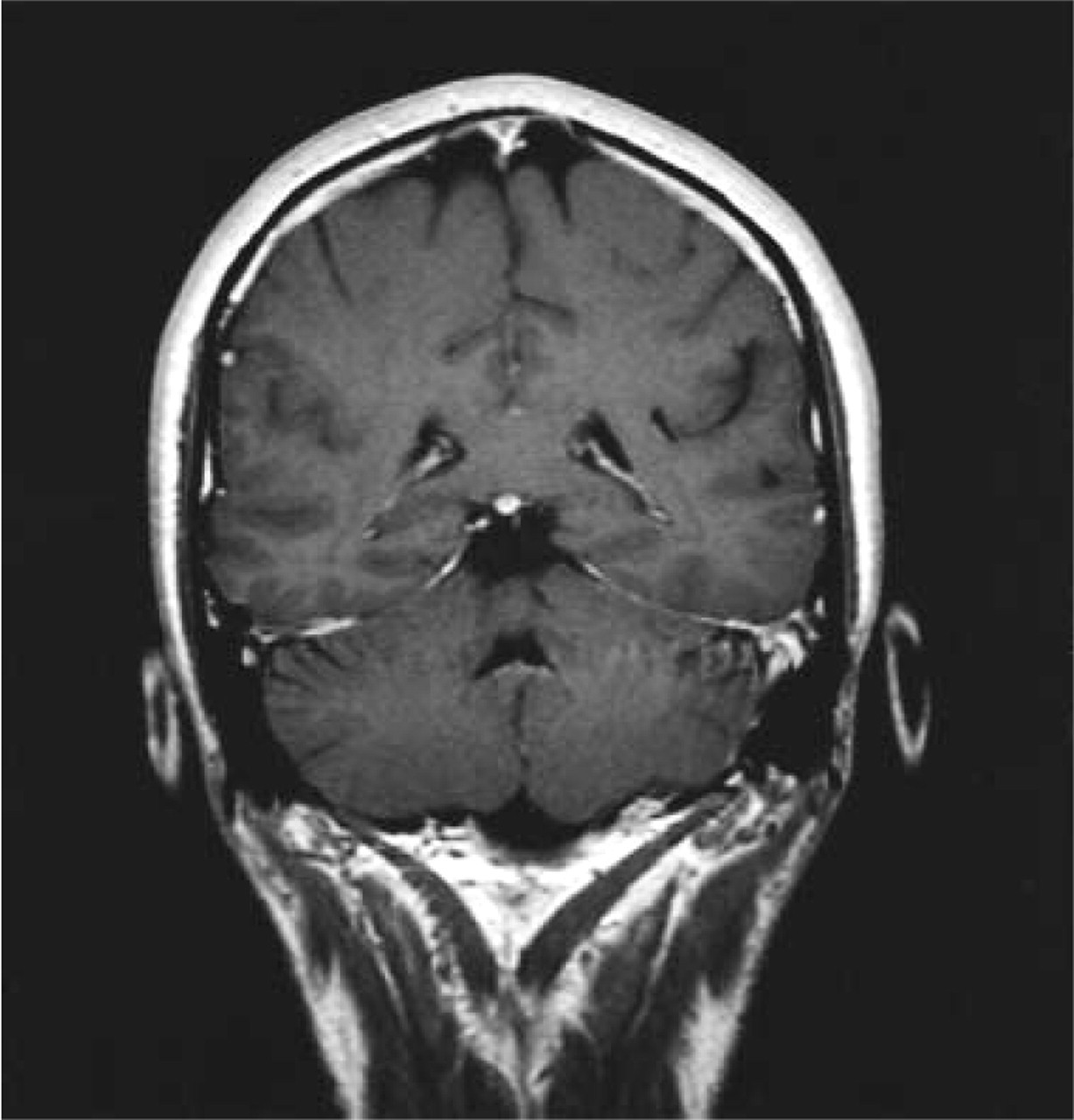
Brain CT scan was normal. Brain MRI with gadolinium showed diffuse pachymeningeal enhancement mostly supratentorial (Fig. 1). MRI myelography, performed using 3-D reconstruction from gradient echo T2-weighted sequence, showed bilateral multiple large meningeal diverticula at sacral nerve roots level (S1-S2) (Fig. 2).

MRI with gadolinium T1-weighted sequence, coronal section, shows diffuse pachymeningeal enhancement.
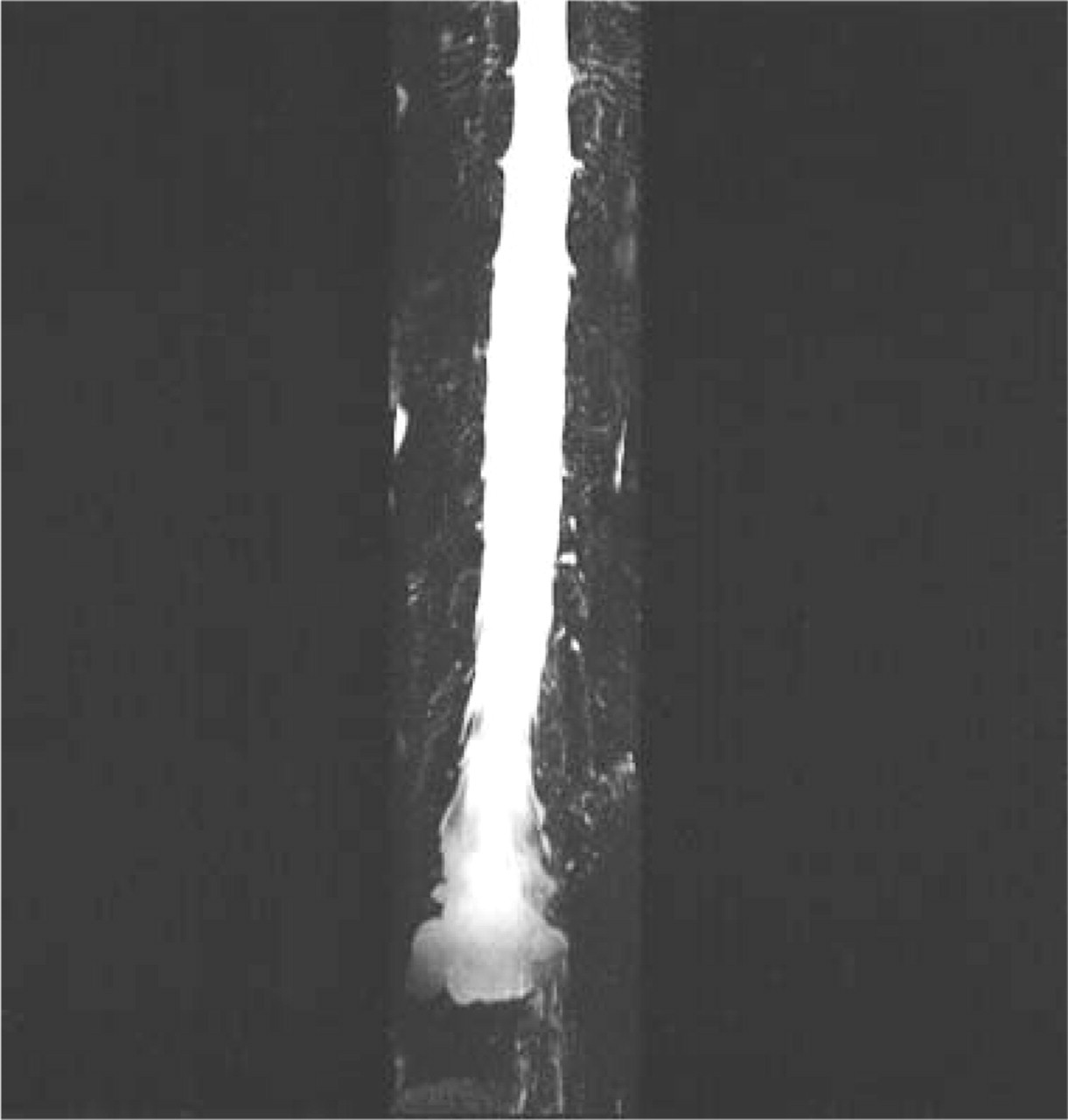
MRI myelography sequences, coronal section, shows dural sac enlargement at the sacral level with large meningeal diverticula at S1-S2 level.
After 8 days of bed rest and hydration, the postural headache improved and the patient was discharged. One month after the discharge the headache progressively resolved and 3 months after the onset the brain MRI was normal (Fig. 3) and the patient was asymptomatic.
MRI with gadolinium, T1-weighted sequence, coronal section, 3 months after the onset of the symptoms shows disappearance of diffuse pachymeningeal enhancement.
Discussion
Marfan's syndrome is due to a deficit of a connective tissue protein known as fibrillin, caused by genetic mutations in the coding of gene for fibrillin-1 at the long arm of the cromosome 15(15q) (3, 5, 6). The main neurological complications of Marfan's syndrome are meningoceles, dural cysts, learning disability and hyperactivity (7). Meningoceles, usually at the lumbosacral level and spinal meningeal diverticula or cysts are also well recognized (8, 9); it has been suggested that these defects develope secondary to the normal, continuous, pulsatile CSF pressure along with minor unrecognized trauma acting on a structurally weakened dura (10, 11).
Our patient was affected by Marfan's syndrome and postural headache associated with diffuse pachymeningeal enhancement at the brain MRI (12), that is typically observed in the spontaneous intracranial hypotension (SIH) (13–16).
SIH is characterized by postural headache, MRI pachymeningeal enhancement and low CSF pressure; it is usually caused by spinal spontaneous CSF leaks that can be sometimes demonstrated by CT myelography, by spine MRI or by radionuclide cisternography (17).
The aetiology of spontaneous CSF leak often remains unknown. In a minority of patients there is a history of trivial or minor trauma. The majority of spontaneous CSF leaks are at the spinal level. Some patients present structural spinal dural abnormalities including meningeal diverticula or dilation of nerve root sleeves. Spinal meningeal diverticula have been described in patients with Marfan's syndrome, neurofibromatosis type 1, autosomal dominant policystic kidney disease, familial osteosclerosis (1, 3).
Recently, abnormal or deficient fibrillin, elastin or both in dermal fibroblast cultures of patients diagnosed with spontaneous CSF leaks and connective tissue disorders have been described (3, 4).
The postural headache is probably caused by traction on pain-sensitive structures (in particular the 5th, 9th and 10th cranial nerve and the upper three cervical nerves) produced by downward sagging of the brain secondary to low CSF pressure (18). Another mechanism causing headache is the compensatory dilation of meningeal pain-sensitive blood vessels due to decrease in CSF volume accompanying intracranial hypotension (19). The pachymeningeal enhancement seen on brain MRI in SIH has been attributed to dural venous dilation secondary to a reduced CSF volume. Recently SIH has also been called liquoral hypovolemia syndrome because sometimes the CSF pressure is normal (20). It is likely that our patient was affected by a SIH, however, a lumbar puncture has not been performed because of the high bleeding risk (INR 4.02). In this case, the intracranial hypotension syndrome most likely resulted by a leak from one of the spinal meningeal diverticula. In a previously described case the MRI myelography showed a CSF leak (21). However in our patient the study did not detect the lesion. In our series of 12 patients affected by SIH, radionuclide cisternography was the most sensitive test (22).
In conclusion, we described a case of a patient with Marfan's syndrome and spinal meningeal diverticula presenting with postural headache, to our knowledge this is the third case reported in letterature (1, 2). The others two were women treated with epidural autologous blood patch that was not necessary in our patient.
The spinal meningeal diverticula are frequent in Marfan's syndrome and represent a risk factor for CSF leaks, often secondary to Valsalva maneuver (i.e. vomiting) or minor unrecognized trauma causing their rupture (1).
Patients presenting with Marfan's syndrome and postural headache should be suspected to have SIH. In these as well as in every patient presenting with postural headache looking for meningeal abnormalities and CSF leaks with appropriate neuroradiological investigation is advised.