
Abstract
Background
Decreased level of consciousness is a rare neurological manifestation of spontaneous intracranial hypotension (SIH), which typically presents with orthostatic headache. The optimal management of this uncommon presentation remains uncertain.
Methods
We analyzed the presentation, management and outcome of two patients in our institution and reviewed 22 patients reported in the literature with SIH and decreased level of consciousness, defined as any decrease in the patient’s Glasgow Coma Scale score.
Results
There were 20 male and four female patients (M:F ratio of 5:1) with an average age of 52 years (range 37 to 68 years). There was a variable time interval of up to many months between the initial presentation of SIH and changes in the level of consciousness. An epidural autologous blood patch was eventually successful in 79% of the patients, although up to three trials were necessary in seven of these patients. Intrathecal saline infusion used as a temporizing measure resulted in excellent response within hours in five out of six patients who received this treatment. Drainage of the subdural collection either did not result in any sustained improvement or resulted in clinical deterioration in 12 out of 12 patients who received this treatment.
Conclusions
In the absence of a clinical trial because of the rarity of this entity, the treatment of SIH complicated by decreased level of consciousness remained controversial in the past. However, current collective experience supports early treatment of patients with SIH and decreased level of consciousness with one or more epidural blood patches. Fibrin glue and surgical duroplasty are the next steps in the management of patients in whom epidural blood patches fail. Drainage of the subdural collections may be detrimental.
Introduction
Spontaneous intracranial hypotension (SIH) classically presents with postural, orthostatic headache. While supportive management with bed rest, hydration, analgesics and caffeine is often tried in patients with milder symptoms, the mainstay of treatment is the spinal epidural autologous blood patch (EBP) (1). The EBP is not only therapeutic but also diagnostic for this condition (2). According to the diagnostic criteria for SIH, the response to EBP should be evident within three days; however, multiple blood patches may be necessary (3).
SIH can rarely be associated with more serious neurological complications such as decreased level of consciousness (4–24). The natural course and the optimal management of patients with SIH and decreased level of consciousness are less certain. Published data on this entity are limited to case reports (4–24). We report two patients with SIH and decreased level of consciousness along with a review of all previously reported patients. The results of this review provide additional information on the management of patients with SIH and decreased level of consciousness.
Case report
Patient 1
A 43-year-old man was transferred from a peripheral hospital with a two-week history of postural headache. There was no immediate history of trauma. However, he had fallen from a ladder one year prior to the event. Neurological examination was unremarkable. Magnetic resonance imaging (MRI) of the brain showed sagging of the brain with displacement of the cerebellar tonsils below the level of the foramen magnum, bilateral subdural fluid collections, diffuse post-gadolinium pachymeningeal enhancement and pituitary hyperemia (Figure 1). A computed tomography (CT) venogram was negative for venous obstruction or thrombosis. These findings were consistent with SIH. A lumbar EBP was performed. He had some improvement but not complete resolution of his headache and was discharged home.
Magnetic resonance imaging (MRI) findings in Patient 1. A, sagittal T1 image shows sagging of the brain resulting in displacement of the cerebellar tonsils below the level of the foramen magnum (dashed line). B, axial T2 image shows bilateral subdural fluid collections (arrowheads). C, post-gadolinium coronal T1 image shows pachymeningeal enhancement (arrows) and pituitary hyperemia (double-arrow). Subdural fluid collections (arrowheads) can again be seen in this image.
Shortly after discharge, he experienced a recurrence of headache associated with nausea and vomiting and returned to the peripheral hospital. A second lumbar EBP was performed without immediate improvement and he was discharged home with a scheduled six-day outpatient neurology follow-up.
At follow-up, he was noted to be drowsy and confused. He continued to experience headache, nausea and vomiting and was transferred to our hospital. A CT myelogram suggested a cerebrospinal fluid (CSF) leak in the C1-T7 region, but was not able to narrow the site of the leak. An EBP at the C7-T1 level resulted in transient improvement of the headache followed by further decline in his level of consciousness.
Drainage of the bilateral subdural collections was considered as there was no response to three EBPs. A left parietal burr hole was placed and a drain was inserted that resulted in improvement in the level of consciousness. However, the improvement was transient and his level of consciousness again declined over the next few days. A mild, right-sided weakness and an episode of abnormal right arm movements were noted three to four days after the neurosurgical drainage, which was clinically diagnosed as seizure and was treated with phenytoin. In the meantime, he also developed fever and tachycardia and was empirically treated with vancomycin and ceftazidime and the subdural drain was removed.
The patient’s level of consciousness continued to decline. He became comatose with a Glasgow Coma Score (GCS) of 4. A repeat MRI showed increased bilateral subdural collections. Bilateral surgical drainage of the subdural collections resulted in another episode of transient improvement in the level of consciousness. A repeat CT myelogram only slightly improved the localization of the CSF leak to between C5 to T1 levels. Ultimately, an exploratory upper thoracic laminectomy was performed and an area of CSF leak was identified and repaired at the T1-3 level followed with further glue duroplasty. Postoperatively, the patient significantly improved, regained consciousness and was eventually discharged home. Neurological examination at discharge revealed that he was alert and oriented to time, place and person. He had mild upper motor neuron right-sided weakness, but was able to transfer unassisted and ambulated with one-person assistance.
Patient 2
A 47-year-old woman presented with acute decreased level of consciousness during a session of hemodialysis. Examination revealed stable vital signs, but she was drowsy and only able to follow simple commands. Her speech was incomprehensible. The remainder of the examination was normal.
Nineteen months prior to the presentation, she had experienced a generalized seizure that had been treated with phenytoin. Gadolinium-enhanced MRI of brain at the time had been consistent with SIH (Figure 2A–2D). Treatment for SIH had not been offered and the findings had been regarded as unrelated to the patient’s clinical picture. Unfortunately, a history of headache or lack thereof was not recorded at that time.
Magnetic resonance imaging (MRI) findings in Patient 2, obtained at the time of initial presentation with seizure (A–D), at the time of presentation with decreased level of consciousness (E and F) and one day after a lumbar autologous blood patch (G and H). A, sagittal T1 image shows sagging of the brain resulting in displacement of the cerebellar tonsils below the level of the foramen magnum (dashed line). B, post-gadolinium coronal T1 image shows pachymeningeal enhancement (arrows) and pituitary hyperemia (double-arrow). C, post-gadolinium axial T1 image shows pachymeningeal enhancement (arrows). Lateral ventricles are notably small in size. D, gradient-echo axial image is unremarkable. E, sagittal T1 image shows further displacement of the cerebellar tonsils below the level of the foramen magnum (dashed line). F, extensive intracerebral venous engorgement can be seen on a gradient-echo axial image. The difference is remarkable compared to the earlier image (D), despite the difference in image qualities. G, improvement in the displacement of the cerebellar tonsils below the level of the foramen magnum (dashed line) on sagittal T1 image. H, improvement in the intracerebral venous engorgement on a gradient-echo axial image.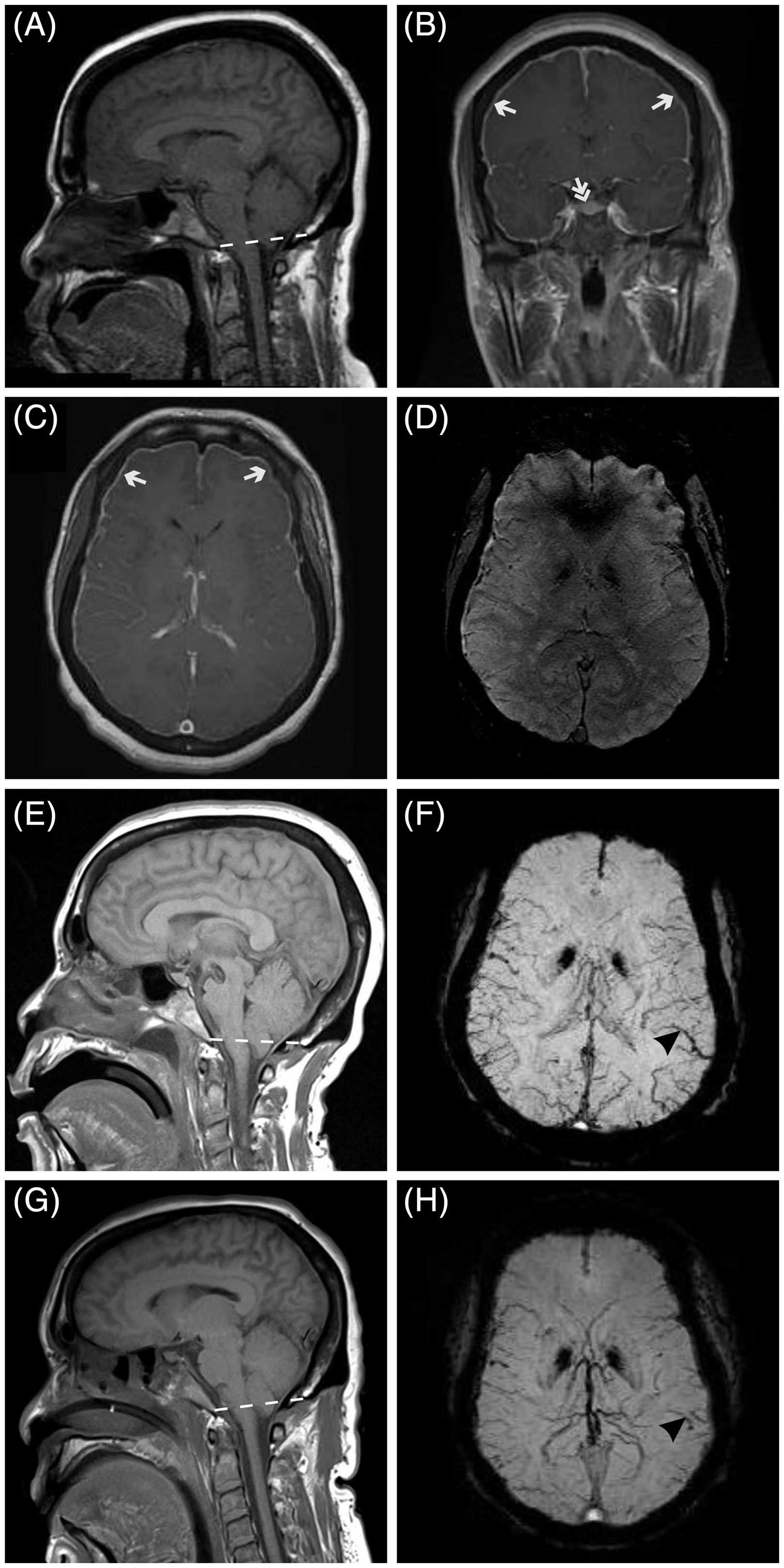
Initial screening blood work was unchanged from her baseline. Over the next few hours, she continued to decline to a GCS of 6 and was intubated. A repeat MRI of the brain showed further displacement of the cerebellar tonsils below the level of the foramen magnum as well as diffuse intracerebral venous engorgement and mild bilateral subdural collections that were not present on the initial scan (Figure 2E and 2F). Repeated electroencephalograms (EEGs) showed non-specific diffuse slowing with no focal or generalized epileptiform discharges.
A lumbar EBP was eventually performed. An angiogram performed in search of the cause of the diffuse intracerebral venous engorgement showed normal superior vena cava pressure. A non-enhanced MRI of the brain obtained one day after the lumbar blood patch showed mild improvements in both the displacement of the cerebellar tonsils below the level of the foramen magnum and the intracerebral venous engorgement (Figure 2G and 2H). Six days after the lumbar EBP the patient was awake and was extubated. A CT scan of the brain showed opening of the lateral ventricles. The patient was discharged home four days later.
Review of cases in the literature
A PubMed search using the keywords “spontaneous intracranial hypotension” or “intracranial hypotension” and either of the keywords “coma”, “decreased level of consciousness”, “subdural hematoma”, “subdural hygroma”, “subdural effusion”, “subdural fluid collection”, “seizure”, “cerebral herniation”, “brain herniation”, “intracranial sinus thrombosis”, “cerebral venous sinus thrombosis” or “venous thrombosis” retrieved 244 articles. These articles included case reports and literature reviews. The retrieved case reports were reviewed and patients satisfying the following criteria were selected:
1. Satisfying the criteria for SIH according to the second edition of the International Classification of Headache Disorders (2) or the criteria proposed by Schievink and colleagues (3); 2. Any described alteration of level of consciousness.
Presenting clinical features of patients with decreased level of consciousness and spontaneous intracranial hypotension.

aInferred from the description in the published report. bDecreased LOC is defined as any decrease in the GCS score. LOC: loss of consciousness; GCS: Glasgow Coma Score; CN: cranial nerve.
Response to treatment in patients with decreased level of consciousness and spontaneous intracranial hypotension. Case numbers correspond to those in Table 1.

EBP: epidural blood patch; IV: intravenous.
Discussion
The review of 22 patients reported in the literature along with our two patients revealed several important pieces of information on the presentation, management and outcome of SIH. While these findings need to be confirmed in a prospective randomized clinical trial, there are several lessons to be learned from this series of patients.
The presenting clinical features of patients with SIH and decreased level of consciousness revealed unexpected findings. Most surprisingly, there was a variable time interval of up to many months between the initial presentation of SIH and changes in the level of consciousness. At least two of these patients had a non-postural headache. These findings raise the question of whether patients with SIH require early management with EBP regardless of focal neurological findings or altered level of consciousness. Unfortunately, there are scarce data on this question. In one case series of 18 patients with intracranial hypotension and delayed diagnosis and treatment of four days to 13 years, there were no patients with decreased levels of consciousness (25). However, cognitive impairment and other neurological deficits were commonly seen among these patients (25). On the other hand, complications of EBP are rare and generally benign (26). While a larger prospective study is clearly required for adequately answering this question, we would advocate an earlier approach to management of SIH to prevent potential serious neurological complications.
Spinal EBPs were generally successful. However, repeated EBPs were often required. Response to this treatment was often immediate but delays of up to 15 days between the treatment and the response were seen. Given that a response to EBP is considered diagnostic for SIH (2), it is not uncommon for the physician to consider an alternative diagnosis when the first EBP fails to provide sustained improvement. Repeating the EBP appears to be the most useful approach in these patients. If a temporizing measure is necessary, intrathecal saline infusion increases the intracranial pressure and provides rapid relief in addition to further confirming the diagnosis.
Drainage of the universally present subdural collection, commonly attempted as the second line of management, was not helpful in any of the patients reviewed here. This observation further asserts that the Monro-Kellie doctrine is the core principle explaining the alteration in level of consciousness in patients with intracranial hypotension (27). There are two main models to explain the pathophysiology of the neurological symptoms seen in these patients (28,29). One model explains the abnormalities seen in intracranial hypotension based on the Monro-Kellie doctrine (27,29). According to this doctrine, the total intracranial volume consisting of CSF, brain parenchyma and blood is constant. Any change in the volume of one component is compensated by an opposite change in the volume of the other component. In patients with intracranial hypotension, a loss in the volume of CSF is compensated by an increase in the volume of blood, in the form of venous engorgement, and brain, in the form of parenchymal swelling. This model easily explains the MRI abnormalities seen in patients with intracranial hypotension (29). The competing model states that the sagging of the brain in these patients results in a narrowing of the angle formed by the vein of Galen entering the straight sinus, which in turn causes stagnation in the venous drainage of the brain stem. According to this hypothesis, the resulting hypoxemia of the brain stem is responsible for the alteration in the level of consciousness in these patients (28). This hypothesis predicts that the removal of the subdural hematoma or hygroma would improve the vein of Galen-straight sinus angle and ultimately the patients’ clinical status by reducing the caudal displacement of the brain. The observation that patients deteriorated after removal of the subdural hematoma or hygroma further supports the Monro-Kellie doctrine as the principal mechanism explaining the alteration in level of consciousness in patients with intracranial hypotension. In other words, the subdural collection is likely a compensatory mechanism in parallel with rather than the cause of the venous engorgement. The two models are not mutually exclusive, however. An unfavorable angle between the vein of Galen and the straight sinus, demonstrated in previous studies (28), may partly contribute to the intracranial venous engorgement seen in these patients. The resulting venous engorgement is likely the final common pathway. In one study, MRI evidence of cerebral venous engorgement was found in all 23 patients with SIH (30). Cerebral venous engorgement was the first sign to disappear following successful treatment in this study. In another study, cerebral venous thrombosis was seen in about 2% of patients with SIH (31). Neurological symptoms and signs other than headache were present in 40% of these patients. The decreased level of consciousness in Patient 2 and her response to EBP coincided with the presence and resolution of cerebral venous engorgement seen on the MRI of the brain, respectively. There was no evidence of direct brain stem compression in this patient. This observation is in agreement with the hypothesis that venous stasis, rather than a direct compression of the brain stem, is the main mechanism for central nervous system (CNS) dysfunction in patients with intracranial hypotension.
Another surprising finding was the demographic distribution of the patients. While the age of patients with decreased level of consciousness was in accordance with previous literature on SIH, there was a higher male to female ratio of 5:1 compared to the reported male to female ratio of 1:2 (reviewed in 1). There was a 1:5 male to female ratio in a case series of patients with intracranial hypotension and delayed diagnosis and treatment (25). This may suggest that male gender is a risk factor for alteration in the level of consciousness in SIH. Whether this observation is merely a chance occurrence or a genuine risk factor that needs to be considered in the management of SIH is another question to be answered by a larger prospective study.
Conclusions
In the absence of a clinical trial because of the rarity of this entity, the treatment of SIH complicated by decreased level of consciousness remained controversial in the past. Based on the review of the published experience to date, it seems reasonable to treat patients with SIH early with EBPs to prevent potentially life-threatening neurological complications. Fibrin glue and surgical duroplasty are the next steps in the management of patients in whom EBPs fail. Furthermore, drainage of the subdural collections should be avoided as it can lead to deterioration in clinical condition.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Decreased level of consciousness is a rare and serious complication of spontaneous intracranial hypotension.
The appropriate treatment of such patients has been controversial in the past.
Based on the published experience to date, patients with spontaneous intracranial hypotension should be treated early with one or more epidural blood patches.
Fibrin glue and surgical duroplasty are the next steps in the management of patients in whom epidural blood patches fail.
Drainage of the subdural collections should be avoided as it can lead to deterioration in clinical condition.