
Abstract
The level of agreement between different sources of information, i.e. questionnaires, interviews and diaries, was evaluated in a sample of 129 schoolchildren, 69 girls and 60 boys, ranging in age from 7 to 17 years. Headache diagnoses and headache features showed high agreement between questionnaires and subsequent interviews. The concordance between questionnaires and interviews for headache diagnoses increased, and the number of unclassified headaches decreased, when the International Headache Society (IHS) duration criterion was excluded. When comparing headache frequency reported in questionnaires and interviews with diary recordings, the agreement was low and the frequency higher in the diaries. Overall, the agreement between questionnaires, interviews and diaries was not related to age or gender. The questionnaire may serve as a valid source of information in studies of headache in schoolchildren. Prospective recordings in diaries provide additional information, in particular of low-intensity headache. In children, the IHS duration criterion should be modified or excluded.
Introduction
In epidemiological studies on the prevalence of headache, results vary not only due to differences between study populations, but also because different methods and diagnostic criteria have been used (1, 2). To improve the reliability of headache diagnoses, the International Headache Society (IHS) classification was introduced in 1988 (3). The IHS classification defines criteria for primary headaches such as migraine and tension-type headache, in addition to secondary headaches (i.e. headache attributable to infection or other diseases). The headache duration and the number of episodes needed to fulfil a certain diagnosis are also specified. These criteria were primarily developed for adults but have been modified for children and adolescents by shortening the duration criterion for migraine without aura.
The IHS criteria are fairly reliable when diagnosing headache in adults (4), but their applicability in children has been questioned (5–8). Several authors have suggested a further shortening of the minimum duration for migraine in children (5, 6, 9–14), or even to exclude this criterion (8, 15). Furthermore, a modification to the IHS criteria has also been suggested for adults (16).
Another source of unreliability in headache diagnosis is the variation of information obtained from the individual (2, 17). In particular, children younger than 9 years of age may have difficulties in recalling and describing headache features (10), and the information is usually based on parents’ reports. In a study involving children aged 10–15 years, discrepancies were found between children's and parents’ interview reports of headache features (18). However, in other studies, acceptable correlations have been found between children's and parents’ reports in interviews (19), questionnaires (20, 21) and diaries (22).
The reliability of information based on questionnaires has been debated (23–25), and the validity has been assessed by comparing diagnoses based on questionnaires with those based on interviews (21, 23, 25–27). To increase the reliability of information concerning headache in children, the use of other methods such as semistructured interviews and diaries has been recommended (2, 28, 29). In population-based (29, 30) and clinical studies (19, 20), information on headache intensity, duration and frequency in diaries has been compared with information obtained from either questionnaires or interviews. In these studies there was variation in the level of agreement regarding information derived from diaries vs. information received via questionnaires or interviews.
Only a few studies in adults deal with the level of agreement between questionnaire and interview information in relation to headache symptoms (23, 31), and to our knowledge this issue has not been investigated in children.
The objectives of this investigation were to estimate: (i) the level of agreement between different sources of information, i.e. questionnaires, interviews and diaries, concerning headache in children; (ii) whether the agreement was related to age or gender of the child.
Materials and methods
The original material consisted of 1850 schoolchildren participating in a questionnaire study on headache at the end of 1997. A random sample of 131 children, stratified according to gender, age and preliminary headache diagnosis, was selected for subsequent interviews.
Interviews were held between 5 and 18 months (median 12 months) after the initial survey. Because headache symptoms could have changed after this time, children and parents were asked to fill out a second questionnaire at home a few days before the interview. This questionnaire was not assessed until after the interviews.
Two children were excluded; one did not answer the questionnaire and the other was found to have secondary headache due to orthostatism. Thus, the final sample consisted of 129 children, 69 (53%) girls and 60 (47%) boys, aged 7–17 years (mean 12 and median 12). According to the second questionnaire, 80 (62%) children had recurrent, primary headache and 49 (38%) had either no headache or secondary headache. At the time of the interview, children suffering from primary headache had done so for an average of 3.8 years.
Questionnaires
In the questionnaires, children were initially asked whether they had experienced headache during or prior to the last year. Children with no headache or only in association with infections or other diseases (i.e. secondary headache) were asked to stop filling out the form after the initial questions. The others were asked additional questions about different headache symptoms covering the IHS criteria, including frequency, intensity and duration of headache, family history, age of onset and whether they had received any treatment or had experienced more than one type of headache.
The questionnaire was previously tested in two samples of schoolchildren (n = 266 and n = 170), and interviews were held with 35 children from the first sample. The agreement between questionnaires and interviews for the diagnoses of migraine, tension-type headache and unclassified headache was good (85.3%), as was the agreement between interview diagnoses (IHS) and diagnoses (intuitive) set by clinicians on the interview responses (88.6%) (unpublished data). In the first version of the questionnaire, answers could be given separately for two types of headaches. However, this format led to some confusion for the children and parents when they were responding. Although 14% of them stated that they had more than one headache type, only 9.5% of the children filled out the questionnaire for each of the different headache types. When the questionnaire answers were analysed and the headache diagnoses set, only 1.6% of the sample actually received two different diagnoses. Therefore, in the version of the questionnaire used in the present study, we abandoned the approach using separate response alternatives for the different headache types.
Interviews
Face to face interviews and clinical examinations were conducted by one of the authors (K.L.). For children younger than 9 years, the parents supplemented the interview information when needed. For teenagers, parents only participated in the first part of the interview concerning headache symptoms and medical history.
The interviews were semistructured with similar questions to the questionnaires, with the following exceptions: (i) in the questionnaire, children were asked whether their headaches were unilateral or not, while during the interview they were asked for the localization of the headache; (ii) the duration of headache was estimated in intervals in the questionnaire, whereas during interviews, children and parents answered with a numeric value (minutes, hours and days); (iii) in the questionnaire, questions concerning phonophobia, photophobia and aggravation by physical activity were answered by ‘Yes’ or ‘No’, but during interviews graded into: ‘None’, ‘Slight’, ‘Quite a lot’ and ‘A lot’.
Diaries
All 129 children were asked to keep a headache diary for 3 weeks following the interview. This diary had been used in earlier epidemiological and treatment studies of headache in children and adolescents (20, 22, 29, 32–34).
Children recorded all headache episodes (including secondary headaches) in the diary and the intensity of each episode was estimated on a 0–5 rating scale (0, ‘No headache’; 1, ‘Slight headache, notable only when paid attention to’; 2, ‘Mild headache that can be ignored’; 3, ‘Headache that cannot be ignored, but activities can be continued’; 4, ‘Severe headache disturbing concentration’; 5, ‘Severe incapacitating headache’). A mean value of the intensity levels was calculated for each subject.
The IHS criteria were applied for establishing a diagnosis of migraine or tension-type headache. All other headache types, including migrainous disorders (IHS 1.7) and tension-type headache not fulfilling the criteria (IHS 2.3) were denoted as being unclassified headache. The diagnosis based on information received from questionnaires was compared with corresponding diagnosis made on the basis of information received via interview. In cases where two headache types were reported in the interview, agreement was considered when one of the interview-based diagnoses was similar to the questionnaire-based diagnosis. Comparisons were also made between single headache features in questionnaires and interviews. Finally, the number of headache episodes and their mean intensity (0–5) reported in the diaries during the 3-week period following the interview were compared with the frequency and intensity (mild, moderate, severe) of headache reported in the questionnaires and interviews.
Statistical analysis
Agreement between the variables in the questionnaires and the interviews was estimated by using Cohen's κ coefficient (35) and percentage agreement. (Cohen's κ coefficient corresponds to the following levels of agreement: 0–0.20, ‘slight’; 0.21–0.40, ‘fair’; 0.41–0.60, ‘moderate’; 0.61–0.80, ‘good’; 0.81–1.00, ‘excellent’.) When the response alternatives in the questionnaires and interviews had different scales, correlations were estimated by Spearman's rank correlation coefficient (ρ).
To estimate whether the directions of disagreement were significantly different in questionnaires and interviews regarding headache characteristics, the McNemar test was used. The differences in proportions of concordant answers between children younger than 13 years and older children and between boys and girls were tested using z statistics.
Results
Questionnaire vs. interview information
In the questionnaire, 53 children (66%) reported a headache duration of < 2 h compared with 19 children (24%) during interviews (Fig. 1). Although longer headache duration was reported during interviews, the coefficient of correlation between questionnaire and interview reports was high (ρ= 0.66).

Headache duration as reported in questionnaires (□) and interviews (▪).
When strict IHS criteria were used (including a minimum duration of 2 h for migraine and 30 min for tension-type headache), agreement between the questionnaire- and interview-based diagnoses was fair (κ= 0.38, 55%). As presented in Table 1a, the proportion of headache not classified as migraine or tension-type headache (unclassified) was higher in the questionnaires (n = 42) than in the interviews (n = 12). This was because longer headache duration was reported in the interviews, leading to more headaches fulfilling the minimum criterion of duration for migraine and tension-type headache. When excluding the headache duration criterion (Table 1b), the agreement between questionnaire- and interview-based diagnoses was enhanced (κ= 0.71, 82.5%). As shown, this modification of the IHS criteria resulted in an increase of the proportion of migraine and tension-type headache diagnoses and an equally large decrease of unclassified headache. The increase was larger for migraine (n = 12 to n = 30) than for tension-type headache (n = 21 to n = 29) because there were fewer children with migraine than with tension-type headache who fulfilled the minimum duration criterion.
Agreement between questionnaires and interviews for International Headache Society diagnoses with the duration criterion

Agreement between questionnaires and interviews for International Headache Society diagnoses without duration criterion

Concordant diagnoses in questionnaires and interviews (diagonal) are in bold.
In the questionnaires, 25% of the children with primary headache reported having more than one headache type, whereas the corresponding figure in the interviews was 20%. However, only 12% fulfilled the IHS criteria for different headache diagnoses.
For single headache features, the highest agreement between questionnaire and interview information was found for ‘vomiting’, ‘visual aura’, and ‘quality of headache’ (Table 2). In contrast, the lowest agreement was found for ‘phonophobia’, ‘photophobia’ and ‘unilateral headache’.
Agreement between questionnaire and interview information on headache features in schoolchildren
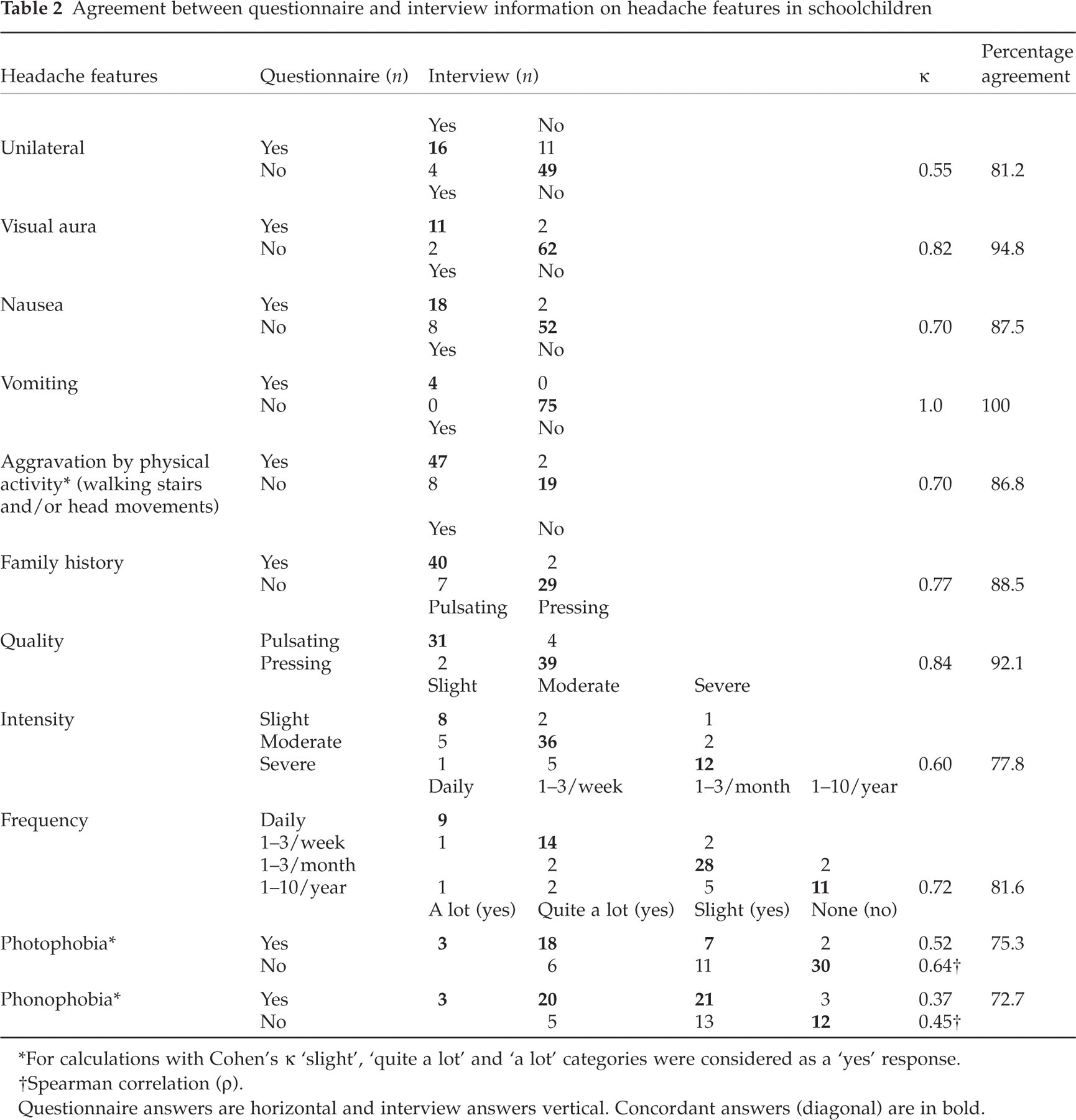
∗For calculations with Cohen's κ‘slight’, ‘quite a lot’ and ‘a lot’ categories were considered as a ‘yes’ response.
†Spearman correlation (ρ).
Questionnaire answers are horizontal and interview answers vertical. Concordant answers (diagonal) are in bold.
‘Phonophobia’ and ‘photophobia’ were more frequently reported in the interviews than in the questionnaires (P < 0.001). There was no significant over- or underreporting in the questionnaires compared with the interviews for any of the other headache features, as reflected by the results of the McNemar test. The response rate for the different headache features varied from 91% to 100%.
The agreement between questionnaires and interviews for headache diagnoses was similar for children younger than 13 years (κ= 0.72, 83.7%) and older children (κ= 0.69, 81.1%), with no significant differences between these age groups, in proportions of concordant diagnoses. Slightly better agreement was obtained for boys (κ= 0.84, 89.7%) than for girls (κ= 0.58, 75.6%), but the difference in proportions of concordant diagnoses was not significant. For headache features, the mean κ values for younger and older children (κ= 0.68 and 0.69 respectively) and for boys and girls (κ= 0.67 and 0.71, respectively) showed only minor differences. No significant differences relating to age were found in the proportions of concordant reports of headache features. For boys and girls, significant differences were obtained only for ‘phonophobia’ and ‘photophobia’ (P < 0.05). For ‘phonophobia’ the agreement was higher for boys than girls, whereas the opposite was found to be the case for ‘photophobia’.
Diary vs. questionnaire and interview information on headache frequency and intensity
A total of 85 children (66%), 46 girls and 39 boys, returned completed diaries. Children younger than 13 years returned diaries in a higher proportion than older children (71% vs. 59%) but no differences in response rate relating to gender and headache diagnoses were obtained. The agreement between the headache diary information and the two other assessment methods was poor, with κ coefficients for headache frequency ranging from 0.15 to 0.27, corresponding to a percent agreement of 55.3% and 61.2%, respectively. In the diaries, children reported a higher frequency of headache compared with questionnaires and interviews (Fig. 2).

Proportion of children with weekly headache as reported in questionnaires (□), interviews (▨) and diaries (▪).
Of those who had returned the diaries and did not report primary headache during the previous year in the questionnaire (n = 36), one-third reported headache occurring at least once during the 3 weeks of diary recordings. However, the majority had only a few episodes of low-intensity headache (median = 1 on the 0–5 scale). No significant correlation was found between mean intensity of the headache episodes in diaries and the intensity levels reported in questionnaires and interviews.
The agreement between reports in diaries and the two other assessment methods was not related to age or gender.
Discussion
In a sample of 129 schoolchildren, we investigated the agreement between different sources of information in the assessment of headache. Together with their parents, children answered a questionnaire a few days before an interview, and thereafter they recorded headache frequency and intensity in a diary for 3 weeks.
Overall, information from questionnaires and interviews showed high concordance. However, the concordance was low for headache frequency and intensity reported in questionnaires and interviews compared with prospective recordings in diaries.
With the use of strict IHS criteria, including a minimum duration of at least 2 h for migraine and 30 min for tension-type headache, the agreement between questionnaires and interviews for headache diagnoses was fair. This can be explained by a higher number of unclassified headaches in the questionnaires, mainly caused by the shorter headache duration reported, compared with the interviews. Consequently, when excluding the IHS duration criterion the agreement improved and the number of unclassified headaches diminished.
In accordance with our results, Mindell et al. (21) found good agreement between questionnaire and interview diagnoses in a clinical sample of 68 children with headache. They used the diagnostic criteria of the Ad Hoc Committee (36) for non-migrainous headache, and those proposed by Prensky and Sommer (37) for migraine. However, in a population-based study of 713 adults, Rasmussen et al. (23), using the IHS criteria, reported low agreement between questionnaire and interview diagnoses, although migraine attacks of short duration were included.
In the present study, the headache feature ‘vomiting’ showed perfect agreement between questionnaire and interview information. Although only four children with headache reported this symptom, the high agreement might be explained by the fact that vomiting is an obvious symptom for parents as well. Excellent agreement was also found for ‘visual aura’ and, somewhat unexpectedly, for ‘quality of headache’. Usually, it is difficult for young children and their parents to describe headache quality, and high proportions of missing responses have been reported (8, 38, 39). In our sample, almost all of the children (96%) and their parents were able to answer this question and the agreement was not related to age or gender of the child. Our results may depend on the children being asked about the most appropriate description of their headaches, given the alternatives ‘pulsating’ or ‘pressing quality’ in both questionnaires and interviews. The interviewer further clarified the response alternatives with gestures.
Although a longer duration was consistently reported in the interviews, estimates of headache duration in the questionnaires and interviews showed an acceptable rank-order correlation (ρ= 0.66). In children, information on duration of headache has been compared between diaries and either questionnaires or interviews (19, 20, 29, 30), but not between questionnaires and interviews. The results of these diary studies (discussed below) show that estimates of headache duration in children vary between different sources of information. This might reflect the natural variation in duration of different headache episodes. In addition, it is difficult for children and their parents to estimate how long the headache persists. Especially younger children may have difficulties telling when the headache started, and parents may be aware of their child's headache only when it is severe.
The largest variation between reports in questionnaires and interviews was obtained for ‘phonophobia’, and may partly be due to the use of different response alternatives in the questionnaires and interviews. Although response alternatives differed equally for ‘photophobia’ and ‘aggravation by physical activity’, the level of agreement was higher. It should be noted that several children, who reported no ‘phonophobia’, ‘photophobia’ or ‘aggravation by physical activity’ in the questionnaire, reported slight symptoms in the interview.
Only a few reports exist on the agreement between questionnaire and interview information for single headache features. Nikiforow (31), in a sample of 200 individuals over the age of 15, found disagreement between questionnaire and interview reports for ‘nausea’ and ‘vomiting’ when the symptoms occurred infrequently. However, for frequent symptoms, good agreement was found. The author also found good agreement for ‘family history’, ‘frequency’ and ‘intensity’ of headache. Rasmussen et al. (23), in 713 adults, reported disagreement between questionnaire and interview reports and a high number of missing values in the questionnaires for headache features such as ‘quality’, ‘nausea’, ‘vomiting’, ‘phonophobia’, ‘photophobia’ and ‘aggravation by physical activity’, but no significant differences for headache ‘duration’, ‘frequency’, ‘severity’ and ‘location’.
When headache frequency and intensity, reported retrospectively in questionnaires and interviews, were compared with prospective recordings in diaries kept for 3 weeks, the agreement was poor. In the diaries, children consistently reported headaches occurring more frequently than with the two other methods, and the estimates of intensity showed no significant correlation with questionnaire and interview information. However, these comparisons were limited by the fact that secondary headaches due to infection might have been included in the diaries. In addition, different measurements for headache intensity were used. Among the children, who considered themselves free from primary headache in questionnaires and interviews, one-third reported at least one headache episode during the 3 weeks of headache recording in diaries. However, the majority of these subjects reported an intensity level of 1, i.e. ‘slight headache, notable only when paid attention to’. The clinical importance of such slight headache may be questioned, and Richardson et al. (22) suggested that intensity levels of 0–2 in the diary should be considered as no headache.
The finding of discrepancy of headache information obtained from questionnaires or interviews compared with information from diaries is in line with other studies. For example, in a recent study of 181 schoolchildren aged 9–16 years, van den Brink et al. (29) found that the agreement of information on headache intensity, duration and frequency was low between questionnaires and diaries. However, diary recordings started 3 months after the questionnaire had been completed. In a population-based study of 145 children aged 11–13 years, Metsähonkala et al. (30) found good agreement between interview and diary information on headache frequency, although headache duration was reported to be significantly longer in the diary than in the interview. Similarly, Labbé et al. (20), in a clinical sample of 28 children aged 7–16 years with migraine, noted that interview data correlated to diary data for headache frequency but not for headache duration. In another clinical study of 53 children aged 8–16 years who were mainly suffering from migraine, Andrasik et al. (19) found longer duration, higher frequency and intensity levels of headache reported in interviews compared with diary recordings. However, after behavioural treatment less variation was observed.
The results of these studies may reflect the difficulties in comparing retrospective information from questionnaires and interviews with prospective recordings in diaries. The former methods have been used in most epidemiological surveys, whilst the latter have been used mainly in treatment outcome studies. Our results show that prospective recordings in diaries are valuable to capture more headache episodes, in particular those of low intensity levels, probably because of less recall errors. However, the higher headache frequency reported in the diaries may also be due to the fact that secondary headache might have been included, or to increased attention to the headache.
In this sample of schoolchildren, the agreement between different sources of headache information was not related to age or gender. These results are in accordance with those reported by Labbé et al. (20) and Andrasik et al. (19) showing no differences in the agreement between children's and parents’ reports relating to age or gender. Unexpectedly, Van den Brink et al. (29) found less recall bias among younger children than among older ones. In none of these studies, nor in the present study, were children younger than 7 years included.
We conclude that the questionnaire may serve as a valid source of information in studies of headache among schoolchildren. Prospective recordings in diaries are useful to estimate the frequency of headache, especially of low-intensity headache.
Further, in epidemiological research on headache in children, the minimum duration of headache is not suitable as an inclusion criterion for migraine and tension-type headache, since it leads to an unreasonably high proportion of subjects that cannot be classified into these diagnoses. It is therefore suggested that the IHS duration criterion should be modified or excluded, particularly in diagnosing migraine in childhood and adolescents.
Footnotes
Acknowledgements
The authors would like to express their deep gratitude to the late Bo Bille, who initiated this work and generously shared with us his great experience of children's headache in research and clinical practice. This work was supported by grants from Uppsala County Council, Uppsala University, Swedish Migraine Society and the following foundations: Gillbergska Stiftelsen, Claes Groschinskys Minnesfond and Stiftelsen Samariten.