
Abstract
In this follow-up study in children and adolescents with recurrent headaches classified as migrainous disorder (IHS 1.7) and headache of the tension-type not fulfilling the criteria (IHS 2.3), 28.6% were headache-free and 71.4% still had headaches 2-5 years after the first examination. The majority remained in the same one-digit IHS diagnosis, whereas 20% changed from migraine to tension-type headache or vice versa. The number of IHS criteria fulfilled increased significantly from the first to the second examination. The reason for diagnosing IHS 1.7 and IHS 2.3 most often was a short headache duration or headache characteristics not meeting the criteria. By reducing the minimum headache duration to 1 h, 11 of 58 patients could be diagnosed as migraine without aura. There was a remarkable overlap in the diagnostic criteria for migraine without aura and tension-type headache. In IHS 1.7 and IHS 2.3 this overlap exceeded 80%, with a trend to decrease at the second examination.
Keywords
Introduction
The International Headache Society (IHS) classification (1) differentiates at the two-digit level seven subtypes of migraine and three subtypes of tension-type headache (TTH). The diagnostic criteria are identical for all age groups with the exception of the duration of migraine without aura which is 2–48 h in subjects < 15 years of age and 4–72 h in the others. Headache attacks which do not quite meet the operational diagnostic criteria for any of the forms of migraine are classified as migrainous disorder (IHS 1.7). Similarly, headache which does not quite meet the criteria for any of the forms of TTH is classified as headache of the tension-type not fulfilling the criteria (IHS 2.3).
Regarding the prevalence of IHS 1.7 and IHS 2.3 in children and adolescents, only few data are available. A clinic-based study (2) found IHS 1.7 in 20.5% and IHS 2.3 in 9.1% of 437 patients referred for recurrent headache. In an epidemiological study including 96 children with headaches disturbing their daily activities, 15% had IHS 1.7 and another 15% had IHS 2.3 (3). In the general population, the prevalence of ‘migraine-like’ headache (defined by the authors as headaches lasting < 2 h but otherwise fulfilling the IHS criteria) was 0.7% compared with a prevalence of 10.6% in definite migraine (4).
The diagnosis of IHS 1.7 and IHS 2.3, i.e. the lack of fulfilment of the criteria for definite migraine or TTH, is due to a short headache duration in the majority of patients (2). In addition, bilateral pain in migraine or unilateral pain with aggravation by physical activity in TTH may also be responsible for diagnosing IHS 1.7 and IHS 2.3, respectively (2). Apart from these factors, the overlap of the symptoms of migraine and TTH may cause further diagnostic difficulties. This overlap is based (i) on the complementary definition of several IHS criteria for migraine and TTH (e.g. unilateral vs. bilateral pain location), (ii) on the fact that two of four complementary headache characteristics must be fulfilled for diagnosing migraine (without aura) and (episodic or chronic) TTH, respectively, and (iii) on associated symptoms common to both headache types. As one can expect, a previous study (5) has shown that the overlap is largest in IHS 1.7 and IHS 2.3.
Up to now there are only cross-sectional, but no longitudinal data on IHS 1.7 and IHS 2.3 in children and adolescents. Therefore, we were interested in performing a follow-up study in order to elucidate the development of the headache diagnoses and headache features in these patients. In addition, we wanted to investigate the percentages of IHS criteria fulfilled and not fulfilled and we wanted to quantify the overlap of the IHS criteria for migraine (without aura) and TTH.
Patients and methods
In a previous study, we examined the applicability of the IHS criteria in 437 consecutive children and adolescents referred to a headache centre (2). For the present follow-up examination, we selected all patients classified initially as IHS 1.7 or IHS 2.3 and we invited them to the clinic 1–5 years after the first interview (mean 2.0 ± 1.2 years). Those who did not respond to the invitation were interviewed by telephone. The interview was based on the same questionnaire as used in the previous study (2). Briefly, this questionnaire covered the biographic data, the duration of the headache history, the frequency and duration of the headache as well as the location, quality and intensity of pain, the influence of physical activity, the occurrence of nausea, vomiting, photo- and phonophobia and the occurrence and duration of neurological symptoms. The questionnaire was completed by the physician based on the child's report or on the parent's report, if she or he contradicted the child.
We established the diagnoses according to the criteria of the IHS and recorded the number of patients who (i) remained in the same IHS one-digit and two-digit diagnoses, (ii) evolved into definite migraine or TTH, (iii) changed the one-digit diagnostic group, or (iv) had no headaches at all. We compared the headache characteristics and associated symptoms at the first and second examination. In addition, we investigated which diagnostic criteria were fulfilled at the first and second examination (A, minimum number of headache attacks/episodes; B, headache duration; C, headache characteristics; D, associated symptoms). Criterion E (exclusion of an organic cause of the headache) was not considered, since it was fulfilled by all patients. Finally, we compared the fulfilment of the IHS criteria for migraine without aura (IHS 1.1) and episodic TTH (IHS 2.1) in IHS 1.7 and IHS 2.3. To estimate the diagnostic overlap we calculated indices using the following formulae: overlap index for IHS (1, 1.1, 1.7) and IHS 2.1 = 1/number of IHS 1.1 criteria fulfilled/number of IHS 2.1 criteria fulfilled; overlap index for IHS (2, 2.1, 2.3) and IHS 1.1 = 1/number of IHS 2.1 criteria fulfilled/number of IHS 1.1 criteria fulfilled.
For statistical analyses we used SPSS for Windows 8.0 software. χ2 tests were used for comparing categorial variables and t-tests for continuous variables. P < 0.05 was considered statistically significant.
Results
Patient characteristics, time since onset, and frequency of headaches
Out of 124 patients, initially classified as IHS 1.7 and IHS 2.3, respectively, 84 (67.7%) were available for follow up. Forty-eight subjects (57.1%) were male and 36 (42.9%) were female. At the time of the first examination, the mean age of the 84 patients was 10.2 ± 2.7 years (4–17 years), the time since the onset of headache was 2.4 ± 2.0 years (1 week to 9 years) and the headache frequency was 2.4 ± 2.5 per month (once a year to every second day).
At follow up 2–5 years after the first examination, 24 patients (28.6%) were entirely headache-free for at least 12 months and 60 (71.4%) still had headaches. In the latter, the mean headache frequency decreased to 1.1 ± 1.5 per month (one per year to seven per month; P < 0.001).
Diagnoses
The initial diagnoses and the diagnoses at follow up are summarized in Table 1. Among the patients initially classified as IHS 1.7, 39.7% had the same diagnosis, 13.8% evolved into migraine without aura, 20.6% changed to TTH, and 25.9% were headache-free. Among the patients initially classified as IHS 2.3, 19.2% remained in the same diagnostic group, 27.0% evolved into definite TTH, 19.2% changed to migraine and 34.6% were headache-free. Looking at the patients still suffering from headaches, 32 (53.3%) remained in the ‘not fulfilling all criteria’ group. At the first examination, one patient had episodic tension-type headache in addition to IHS 1.7 and one patient had migraine without aura in addition to IHS 2.3. At follow up, another patient had episodic tension-type headache in addition to migraine without aura.
Diagnosis at follow up in 84 patients initially classified as migrainous disorder and headache of the tension-type not fulfilling the criteria
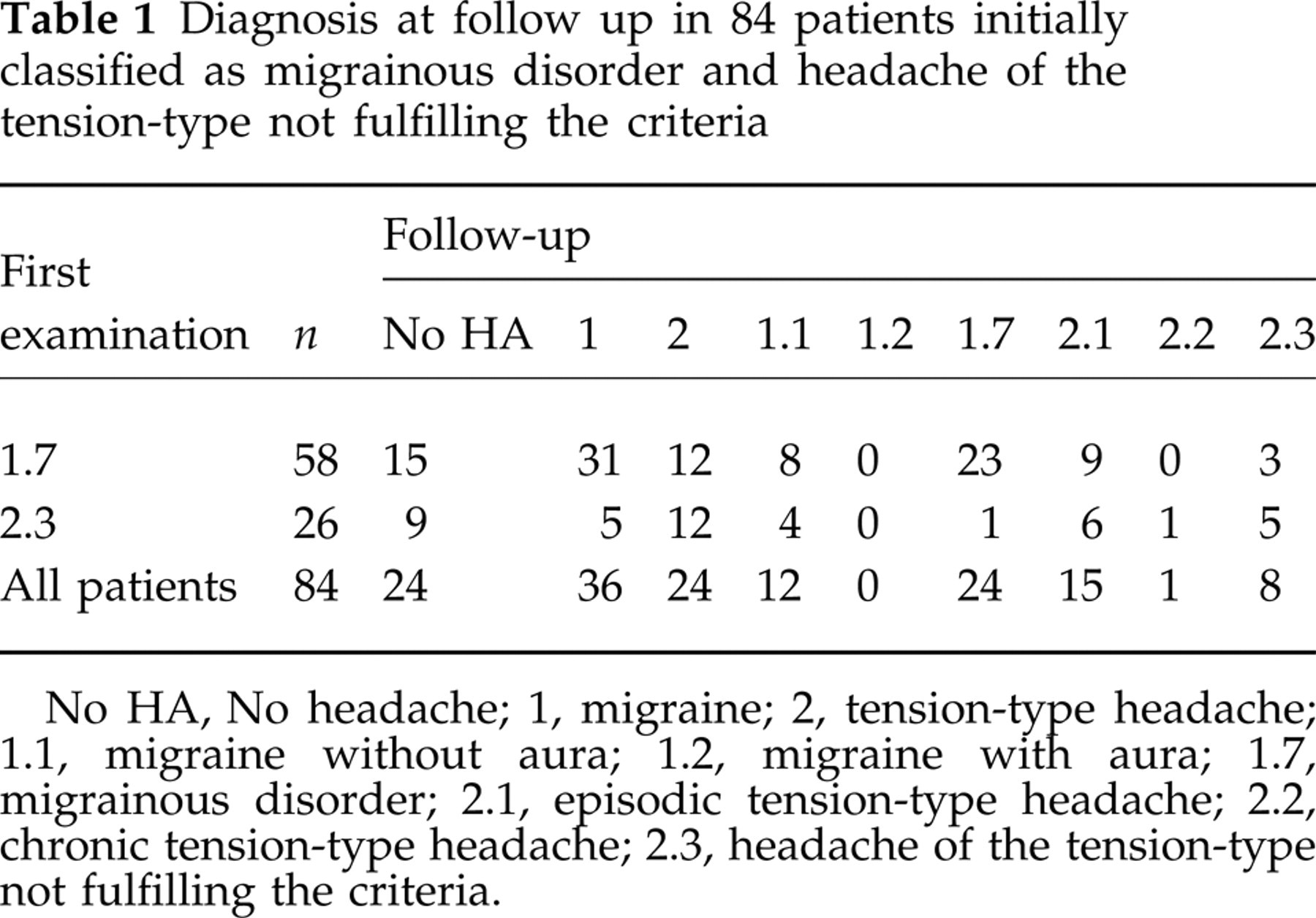
No HA, No headache; 1, migraine; 2, tension-type headache; 1.1, migraine without aura; 1.2, migraine with aura; 1.7, migrainous disorder; 2.1, episodic tension-type headache; 2.2, chronic tension-type headache; 2.3, headache of the tension-type not fulfilling the criteria.
Headache features
At the first examination a typical headache attack in patients diagnosed IHS 1.7 lasted 2.9 ± 3.4 h. At follow up the mean headache duration increased to 5.6 ± 7.9 h and this increase was statistically significant (P = 0.045). The headache duration in IHS 2.3 increased from 3.0 ± 3.3 h to 5.1 ± 4.6 h, which was not statistically significant.
Tables 2 and 3 summarize the prevalence of the headache features and show statistically significant changes regarding the quality of headache and the type of associated symptoms. Compared with the first examination the prevalence of pulsating headache, photo- and phonophobia increased, whereas that of nausea and vomiting decreased at follow up.
Headache characteristics in 84 patients initially classified as migrainous disorder and headache of the tension-type not fulfilling the criteria; comparison of first examination and follow up

Headache-free patients (n = 24) were not included.
P values < 0.05 were considered statistically significant.
Associated symptoms in 84 patients initially classified as migrainous disorder and headache of the tension-type not fulfilling the criteria; comparison of first examination and follow up
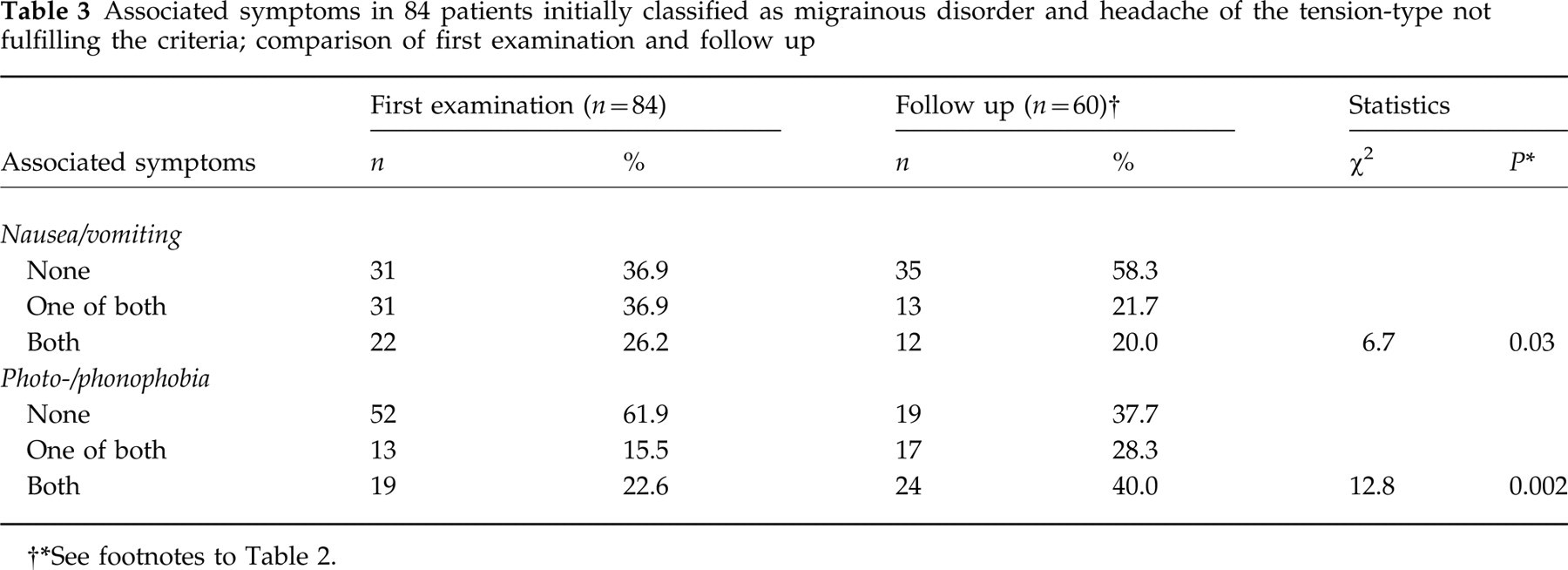
See footnotes to Table 2.
Diagnostic criteria
The percentages of IHS criteria fulfilled increased from the first examination to the follow up. As shown in Table 4, the numbers of subjects fulfilling the minimum number of headache attacks or episodes, the headache duration and the headache characteristics were significantly higher at the second examination than at the first one. In contrast, the number of subjects fulfilling the associated symptoms remained unchanged.
International Headache Society (HIS) criteria for migraine and tension-type headache: number and percentage of criteria fulfilled and not fulfilled at the first examination and at follow up

See footnotes to Table 2.
Including 10 and two patients, respectively, not fulfilling criteria B and C (headache duration and characteristics).
Including two patients and one patient, respectively, not fulfilling criteria B and D (headache duration and associated symptoms).
P< 0.05 was considered statistically significant.
In conflict with the strict definition of the IHS criteria, 11 patients classified as IHS 1.7 did not fulfil two criteria of migraine and two patients classified as IHS 2.3 did not fulfil two criteria of TTH at the first examination. In IHS 1.7, all of these patients had attacks lasting < 2 h, 10 did not meet the headache characteristics and one did not fulfil the associated symptoms. However, 10 patients had nausea and/or vomiting and nine had moderate or severe pain intensity. (In addition, history, physical and neurological examination did not suggest an underlying organic disorder in any of these patients.) Accordingly, we diagnosed IHS 1.7, even though eight of the 11 patients would have fulfilled the IHS 2.3 criteria. The usefulness of this decision was confirmed at follow up: six of the patients remained IHS 1.7 (fulfilling all criteria but duration) and two evolved into migraine without aura; another two patients were entirely headache-free, and one patient only changed to TTH. Of the two patients initially classified as IHS 2.3, one remained IHS 2.3 (with just one criterion not fulfilled) and the other one was headache-free.
Overlap
At the first examination in patients with IHS 1.7, 163 of 232 criteria (four criteria in 58 patients) were consistent with migraine without aura, and as much as 145 were consistent with episodic TTH. In patients with IHS 2.3, 76 of 104 criteria (four criteria in 26 patients) were consistent with episodic TTH, and 61 were consistent with migraine without aura. The overlap index—calculated by using the formulae given above—was highest in IHS 1.7 and IHS 2.3 and lowest in episodic tension-type headache and migraine without aura (Table 5). Parallel with the increase of IHS criteria fulfilled, the overlap index decreased in migraine from 0.89 to 0.78 and in TTH from 0.8 to 0.6 at follow up.
Diagnostic overlap of migraine and tension-type headache

Number of patients with different headache diagnoses fulfilling one, two, three or four of the four criteria of migraine without aura (IHS 1.1) and episodic tension-type headache (IHS 2.1). The overlap index was calculated following the formulae given in Patients and Methods.
Discussion
In this follow-up examination of children and adolescents with recurrent headaches classified as IHS 1.7 and IHS 2.3, 50% of the subjects stayed in the same one-digit IHS diagnosis, almost 30% became headache-free and 20% changed from migraine to TTH or vice versa. In the patients with persistent headaches, the headache features changed markedly and the number of patients fulfilling a certain IHS criterion increased in all criteria except the associated symptoms. The diagnostic overlap of the criteria of IHS 1.7 and IHS 2.3 was considerable and exceeded 80%, i.e. that a headache classified as IHS 1.7 fulfilled > 80% of the IHS 2.3 criteria and vice versa.
A change from migraine to TTH and vice versa was also described in two other studies (6, 7), reaching up to 28.6%. These studies however, included patients with definite migraine and TTH only. As yet there is no satisfactory explanation of this phenomenon and the discussion whether migraine and TTH are two ends of a continuum or two definitely separate entities is ongoing (8–10).
Apart from changes in the diagnoses, another important finding was that almost 30% of the patients were headache-free for at least 1 year. The prognosis of childhood headache was examined in few studies only. Bille's epochal work covers a period of 40 years (11–13) and showed that 62% of juvenile migraineurs were free of migraine attacks for at least 2 years during puberty, but 60% had migraine again at the age of 30 and at the age of 50 half the patients still had migraine or had migraine again. Sillanpää contributed several epidemiological studies dealing with long-term follow-up examinations (14, 15). He found 22% headache-free after 7 years, with boys predominating. Three recent studies applied the IHS criteria: in a population-based 3-year follow up by Metsähonkala et al. (16) only 4.8% of the children were headache-free. In contrast, in two clinic-based studies Dooley et al. (6) and Guidetti & Galli (7) found 27% and 34%, respectively, free of headaches (but neither of the studies included IHS 1.7 and IHS 2.3). In addition, it is noteworthy that Guidetti & Galli (7) defined ‘headache-free’ as having headache attacks less than once a month over the last 2 years. Patients suffering from TTH had a higher chance to become headache-free than patients with migraine without aura (6, 7), similarly in our study more patients with IHS 2.3 got headache-free than patients with IHS 1.7, but this was not statistically significant.
Parallel with the changes in the headache diagnoses, we observed marked changes in headache features. Compared with the literature, an epidemiological study (14) showed an increasing frequency of migraine attacks in a 7-year follow up, whereas clinic-based studies (6, 7)—including our own study—revealed a decrease in headache frequency. This discrepancy could be explained by a selection bias in clinic-based studies, as many children are presented to a headache specialist at the time of particularly frequent headaches.
Reasons for diagnosing IHS 1.7 and 2.3 most often were a short duration of the headache attacks or headache characteristics not meeting the criteria. The minimum headache duration was a limitation for establishing the diagnoses of definite migraine and TTH in previous studies, too (2, 17–19). Accordingly, the reduction of the minimum migraine duration to 1 h was suggested (2, 17, 20), whereas a further reduction was found to reduce the specificity of the criteria (20). Changes of other criteria were discussed also (2, 19–23). Regarding the sensitivity of the pain characteristics in migraine without aura (IHS criterion C), the results are conflicting. One group (20) found a good sensitivity for all criteria and concluded that the criteria should remain unchanged, whereas others reported good sensitivity for intensity and aggravation by physical activity only (2, 17, 19). In the present study, most patients diagnosed as IHS 1.7 had moderate to severe intensity of their headache attacks. Therefore, the pain intensity seems to be the most important among the four pain characteristics of migraine without aura. In agreement with this, Rasmussen et al. (23) proposed a revision of the IHS criteria by establishing the headache intensity as a criterion of its own, both in migraine without aura and TTH. However, the sensitivity of the modified criteria was not higher than that of the current ones, i.e. none of the patients with IHS 1.7 and IHS 2.3 would have changed to definite migraine without aura or TTH by separating the intensity from the other headache characteristics.
Another diagnostic problem arises from the overlap of the symptoms of migraine and TTH. Often, migraine-like symptoms can be observed in patients with TTH and vice versa (2, 23). This overlap is most pronounced in IHS 1.7 and IHS 2.3 (5) and this could also be shown in the present study, which indicated that the overlap decreased in the course of time. Messinger et al. (5) assumed that this overlap is due to methodological problems of the IHS classification. They suggested that the overlap in diagnoses could be diminished if the headache symptoms, such as intensity, duration, quality, aggravation by physical activity, were not combined to build up one common criterion, but each symptom were treated as a separate criterion. However, the authors do not comment on the practicability of such modifications within the framework of the IHS classification.
In conclusion, in patients with IHS 1.7 and IHS 2.3 nearly 30% have a chance to become headache-free for at least 1 year within 2–5 years after their first presentation to a headache centre. Fifty percent remain in the same one-digit IHS diagnosis, whereas 20% change from the one-digit diagnosis migraine to TTH or vice versa. Establishing a definite diagnosis according to the IHS criteria in children and adolescents is impaired by criteria not fulfilled and by an overlap of the symptoms of migraine and TTH, especially in IHS 1.7 and IHS 2.3, but this restriction improves in the course of time.