
Abstract
The objective of this study was to study the prevalence, characteristics and predisposing factors of tension-type headache in children. An unselected population-based questionnaire study was carried out in 1409 Finnish schoolchildren aged 12 years. Of them, 1135 (81%) returned an acceptably completed questionnaire. The prevalence of episodic tension-type headache in children was 12% (138 of 1135). Children with episodic tension-type headache also often reported characteristics of pain typical for migraine. Children with frequent and persistent episodic tension-type headache reported stabbing and severe occipital pain, phonophobia and abdominal pain significantly more often than children with infrequent episodic tension-type headache. Neck-shoulder symptoms, symptoms of depression and oromandibular dysfunction were each independently associated with episodic tension-type headache. The father's occupation of a lower-level white-collar worker put the child at a four-fold risk for episodic tension-type headache. We conclude that episodic tension-type headache is as common as migraine in children. It can be associated with depression, oromandibular dysfunction and muscular stress. Especially children with frequent and persistent episodic tension-type headache report characteristics of pain typical for migraine.
Introduction
Tension-type headache is a common problem in adults (1, 2). On the other hand, about 35% of children and adolescents attending headache clinics also report tension-type headache according to the criteria of the International Headache Society (IHS) (3–5). Although several population-based studies have been published on the occurrence of migraine in children, few population-based epidemiological studies have been reported on childhood tension-type headache (6).
Muscular stress, oromandibular dysfunction, depression, psychosocial mechanisms and drug overuse are assumed causative factors of adult tension-type headache (5). The association of these factors with childhood tension-type headache is unknown. It is, however, known that all chronic headaches are associated with depression, especially in girls (7). In a clinic-based study (8), tension-type headache was associated with psychosocial factors, such as a higher rate of broken homes and fewer peer relations.
We investigated in children the prevalence and characteristics of tension-type headache and its predisposing factors, including the association of neck-shoulder symptoms, symptoms of oromandibular dysfunction and depression. It was hypothesized that tension-type headache is a common complaint and associated with neck-shoulder symptoms, symptoms of oromandibular dysfunction and depression in children. It was also expected that the characteristics of tension-type headache differ from those of migraine, but these differences are not specific.
Subjects and methods
Study design
The present study was based on an unselected population-based cohort of 12-year-old children. In early 1998, a structured questionnaire on headache and its predisposing factors was sent to all 1409 children in the sixth form of 35 primary schools in the City of Turku, South-western Finland. Teachers delivered the questionnaire to the children, who filled it in at home together with their parent(s). Of the children, 1135 (81%) returned the questionnaire acceptably completed.
The questionnaires were sent to both 33 schools for Finnish-speaking children and two schools for Swedish-speaking children. Finnish and Swedish are the two official languages of Finland. One of Swedish schools did not comply, and the participation rates of the other Swedish school and the Steiner school were low (52% and 20%, respectively). These three schools accounted for 121 pupils (9%). The participation rate was 86% among Finnish-speaking children in municipal primary schools. No differences in sex distribution were found between participants and non-participants.
IHS criteria (5) were used for the definition of different types of headache. The children were asked about the frequency of various headache features and associated symptoms as follows: ‘Has your headache been associated with the following symptoms and headache characteristics, and if it has, how often during the preceding 6 months?’ (Reply options: every time/at least every second time/less than every second time/sometimes/never.) If a child reported an associated symptom or headache feature every time/at least every second time, this criterion was considered fulfilled.
We compared the following variables for children with episodic tension-type headache and children with no headache: socio-economic variables, familial occurrence of headache, neck-shoulder symptoms, symptoms of oromandibular dysfunction, and depressive symptoms.
The socio-economic variables included questions about the parents' basic and vocational education and socio-economic status (9), and possible unemployment (no/yes) or economic problems (no/yes). Familial occurrence of migraine, diagnosed by a doctor, and other types of headache that were disturbing daily activities were regarded as familial occurrence of headache.
Neck-shoulder symptoms were evaluated as follows. Children were asked about the occurrence and frequency of neck-shoulder pain during the previous 6 months or occurrence of muscle tenderness in the neck-shoulder region during daily activities.
Oromandibular dysfunction was determined according to the IHS criteria (5) as three or more of the following features: temporomandibular joint noise on jaw movements; limited jaw movements; pain on jaw function; locking of jaw on opening; clenching of teeth; gnashing of teeth (bruxism); or other oral parafunction such as tongue, lips or cheek biting or pressing. Symptoms of oromandibular dysfunction included at least one of the above features.
DSM IV criteria (10) for depression were used to detect major depression and depressive symptoms. Major depression was determined as at least five criterion features occurring almost every day for 2 weeks with depressed mood or loss of interest or pleasure as at least one symptom. The features of depression were: depressed mood, loss of interest or pleasure, weight loss or gain, or poor or increased appetite, insomnia or hypersomnia, psychomotor agitation or retardation, fatigue or loss of energy, feelings of worthlessness or excessive guilt, diminished ability to concentrate or indecisiveness, and recurrent thoughts of death or a suicide attempt. A child was considered to have depressive symptoms if he or she reported at least two of the above features.
Pain characteristics and accompanying symptoms were also compared between children with episodic tension-type headache and those with migraine. In addition, differences in pain characteristics and accompanying symptoms were studied between children with frequent and persistent (≥one/week for at least 6 months) episodic tension-type headache and those with infrequent episodic tension-type headache.
Statistical analysis
Student's two sample t-test, Pearson's χ2 test and Fisher's exact two-tailed test, when appropriate, were used for comparison of characteristics among the different types of headache and differences between tension-type headache and no headache with regard to socio-economic variables, familial occurrence of headache, neck-shoulder symptoms, symptoms of oromandibular dysfunction and depressive symptoms.
Stepwise logistic regression analysis was carried out to find out which symptoms (neck-shoulder, oromandibular or depressive) were independently associated with the occurrence of tension-type headache. The explanatory variables were dichotomized as follows: depression (0–1 symptoms/≥2 symptoms), oromandibular dysfunction (no symptoms/≥1 symptom), and neck-shoulder symptoms (<1/month neck-shoulder pain and no muscle tenderness in the neck-shoulder region during daily activities/neck-shoulder pain ≥1/month or muscle tenderness in the neck-shoulder region sometimes or often during daily activities).
Odds ratios (OR) with 95% confidence intervals (95% CI) were calculated using the formula based on normal approximation: CI=exp ((b±1.96 SE (b)), where b is the estimate of the coefficient in the logistic model and SE (b) its standard error.
The statistical computation was performed using BMDP90 statistical software (version 7; BMDP Statistical Software Inc., Los Angeles, CA, USA) (11).
A P-value of <0.05 was used as the cut-off point of significance.
The study design was approved by the Joint Ethics Committee of the University of Turku Medical School and the Turku University Central Hospital.
Results
Prevalence of different types of headache
The prevalence of episodic tension-type headache in the children was 12.2% and that of migraine 13.6% (Table 1). In addition to these groups, approximately 20% of the children did not fulfil all IHS criteria (5) for migraine or for tension-type headache. No children fulfilled the IHS criteria (5) for chronic tension-type headache. However, 1.6% of all children (18 of 1135) reported occurrence of headache at least during 15 days a month for at least 6 months. In addition, 15.2% of children with episodic tension-type headache (21 of 138) had a history of weekly headache episodes for at least 6 months. Twelve percent (136 of 1135) reported only secondary headaches (post-traumatic headache in 17 children, refractive errors in 27 children and headache associated with non-cephalic infection or disorders of sinuses or teeth in 92 children). Thirty-six percent of the participants had had no headache.
Prevalence of different types of headache in children according to IHS criteria (1988)

Characteristics of episodic tension-type headache
The mean age at onset of tension-type headache was 7.4 years (Table 2). Tension-type headache occurred equally often in boys and girls.
Characteristics of episodic tension-type headache in comparison with migraine in children

∗ P-value of statistical difference between groups.
The children had had headache episodes twice a month on average, and the median duration of the episodes was 1.5 h. The frequency and duration of tension-type headache episodes were lower and their pain intensity milder than in migraine.
Drug administration in episodic tension-type headache
The frequency of drug administration was lower in episodic tension-type headache than in migraine (Table 2). Most children with tension-type headache (85%) had taken headache medication, but only 12% of them had taken medication every time they had headache. The most common drug for tension-type headache was ibuprofen (52%).
Characteristics of pain and accompanying symptoms
Table 3 presents characteristics of pain and accompanying symptoms in episodic tension-type headache in comparison with migraine. The quality of pain was significantly more often ‘constant’ in children with episodic tension-type headache than in those with migraine. In bilateral location, no significant differences were found between these two groups. Among the accompanying symptoms, nausea, vomiting or anorexia were not associated with episodic tension-type headache. Photophobia, phonophobia and pain aggravation due to routine physical activity were significantly more often associated with migraine than episodic tension-type headache. However, 10–13% of children with episodic tension-type headache also reported these features.
Characteristics of pain and accompanying symptoms in childhood episodic tension-type headache and migraine

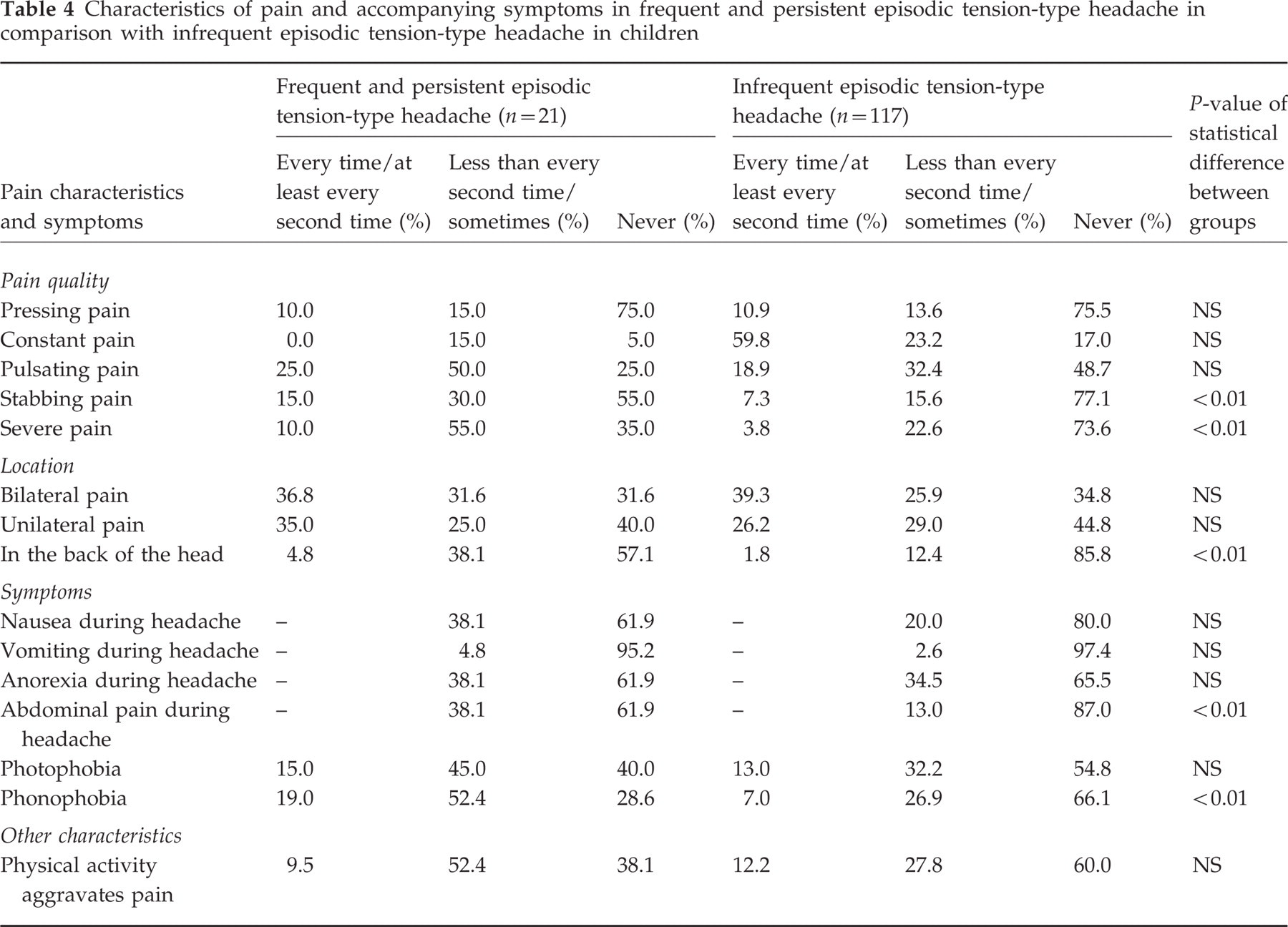
Table 4 presents characteristics of pain and accompanying symptoms in frequent and persistent episodic tension-type headache in comparison with infrequent episodic tension-type headache. Pain was stabbing or severe and located in the back of the head and increasing during the day significantly more often in children with frequent and persistent episodic tension-type headache than in those with infrequent episodic tension-type headache. Among the accompanying symptoms, phonophobia and abdominal pain were significantly more often associated with frequent and persistent episodic tension-type headache than with infrequent episodic tension-type headache. In the duration of headache episodes, no significant differences were found between the two headache groups (P=0.143).
Characteristics of pain and accompanying symptoms in frequent and persistent episodic tension-type headache in comparison with infrequent episodic tension-type headache in children
Symptoms indicating possible causative factors
Thirty-eight percent of children with episodic tension-type headache and 25% of those with no headache reported neck-shoulder pain during the previous 6 months. In addition, muscle tenderness in the neck-shoulder region during daily activities was reported by 35% of children with episodic tension-type headache and by 21% of those with no headache.
Symptoms (≥1 symptom) of oromandibular dysfunction were reported by 27% of children with episodic tension-type headache and by 18% of those with no headache. The criteria of oromandibular dysfunction were fulfilled by 1.5% of children with episodic tension-type headache and by 0.5% of those with no headache.
Depressive symptoms (≥2 symptoms) were reported by 17% of children with episodic tension-type headache and in 6% of those with no headache. The criteria of major depression were fulfilled by 1.5% of children with episodic tension-type headache. Among children with no headache, none fulfilled those criteria.
Of children with episodic tension-type headache, 39% did not report neck-shoulder symptoms, symptoms of oromandibular dysfunction or depression in comparison with 63% of those with no headache.
Univariate analysis
In comparison between the tension-type headache group and the no headache group, the father's occupation of a lower-level white-collar worker placed the child at a four-fold risk for episodic tension-type headache (P<0.01; OR 4.2, 95% CI 1.9–9.4). Other socio-economic variables or familial occurrence of headache showed no difference between the two groups.
The occurrence of neck-shoulder symptoms (P<0.001; OR 2.0, 95% CI 1.3–2.9), depressive symptoms (P<0.001; OR 3.3, 95% CI 1.8–6.1) and symptoms of oromandibular dysfunction (P<0.001; OR 1.6, 95% CI 1.0–2.6) predicted occurrence of episodic tension-type headache.
As single symptoms of oromandibular dysfunction, biting of tongue, lips or cheek were the most distinctive features between children with episodic tension-type headache and those without headache (P<0.01; OR 2.5, 95% CI 1.2–5.1). As single depressive symptoms, sleep disturbances (P<0.01; OR 3.3, 95% CI 1.5–7.6) and depressed mood (P<0.05; OR 2.6, 95% CI 1.5–5.7) were the most distinctive features between children with episodic tension-type headache and those without headache.
Multivariate analysis
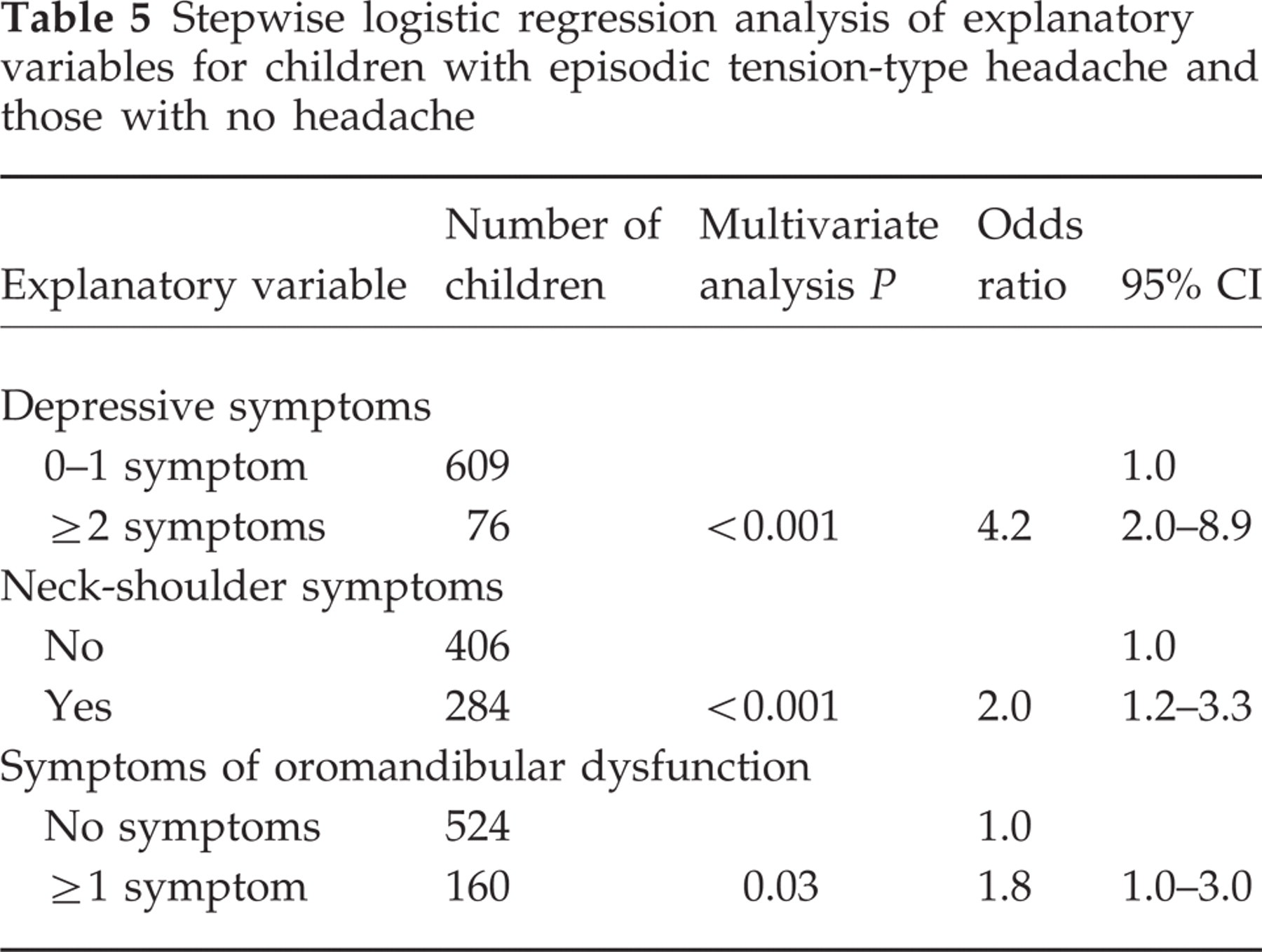
Table 5 shows the results of stepwise logistic regression analysis. The occurrence of episodic tension-type headache was independently predicted by depressive, neck-shoulder and oromandibular dysfunction symptoms.
Stepwise logistic regression analysis of explanatory variables for children with episodic tension-type headache and those with no headache
Discussion
To our knowledge, this is the first unselected population-based study of the occurrence and features of childhood tension-type headache according to IHS criteria. It is well known that tension-type headache is common not only in adults but also in children. We confirmed that episodic tension-type headache is as prevalent as migraine in prepubertal children.
Our results agree with those reported from a Swedish study (12). In a previous study from Brazil (6), the prevalence of tension-type headache was found to be as high as 73% in children aged 10–18 years. The difference in prevalence rates between the two Scandinavian studies and the study from Brazil may depend on cultural factors or the age of the children, but is probably related to the use of the IHS criteria. Using very strict criteria for tension-type headache, Abu-Arafeh and Russell (13) reported a prevalence of 0.5% for tension-type headache in children aged 5–15 years. Their subjects represented probably children with chronic tension-type headache.
The quality of pain was pressing more often in children with migraine than in those with tension-type headache, although this characteristic has been considered typical for tension-type headache. In addition, many children with tension-type headache also reported symptoms and characteristics of pain typical for migraine, such as unilateral pain, photophobia, phonophobia, pulsating pain and aggravation of pain due to routine physical activity. According to a population-based study by Rasmussen et al. (14), 10% of adults with tension-type headache have unilateral pain, 11% photophobia, 18% pulsating pain, 28% aggravation of pain due to routine physical activity, 18% anorexia and 4% nausea. Unilateral pain and phonophobia may be more typical of childhood tension-type headache than of tension-type headache in adults.
The high number of children with primary headache who did not quite fulfil the IHS criteria for tension-type headache or migraine and the unspecific nature of the features of headache may indicate that many children in the general population have mixed headaches. The headaches of these children have features typical for both migraine and tension-type headache. It also indicates that the present way of classifying headaches involves problems which may be even more evident in children than in adults.
In the present study, 16% of children had migraine-type headache, not fulfilling IHS criteria, while only 4% of children had tension-type headache, not fulfilling IHS criteria. This may indicate differences in sensitivity and specificity of the IHS criteria for paediatric migraine and tension-type headache. It is possible that the IHS criteria for tension-type headache are more sensitive than the criteria for migraine in children.
In our study, no children had chronic tension-type headache. However, 15% of children with episodic tension-type headache had weekly headache episodes for at least 6 months. These frequent headaches had some typical features: migraine-type features such as phonophobia and severe or stabbing pain, predilection for occipital location and tendency to aggravate during the day. Children, like adults (15), with frequent episodic tension-type headache may be at increased risk of chronic tension-type headache.
IHS criteria include the most likely causative factors for tension-type headache (5). No population-based studies have been published on the occurrence of these factors in association with childhood tension-type headache. We found that children with episodic tension-type headache more often had neck-shoulder symptoms, depressive symptoms and symptoms of oromandibular dysfunction than children with no headache. However, none of these three factors could be found in one-third of children with episodic tension-type headache. In the present study, the occurrence of three factors was based on subjective reporting of symptoms, which does not necessarily agree with clinical diagnoses of depression, oromandibular dysfunction or pericranial muscular stress.
In adults, a population-based study has shown increased muscle tenderness, recorded by manual palpation, both in subjects with episodic tension-type headache and those with chronic tension-type headache compared with subjects without headache (16). In addition, the pathogenic importance of muscular factors in tension-type headache has been underlined in reports on spontaneous and induced headache (17, 18). To date, adult studies have not determined whether myofascial tenderness is primary or secondary to pain in tension-type headache (19). At least in some children, the pathophysiology of episodic tension-type headache is probably related to local pericranial muscular stress or pathological dysfunction of muscles. Our results support this. However, unexpectedly many children without headache also reported pain or tenderness in the neck-shoulder region.
In our questionnaire study, major depression occurred in 1.5% of children with episodic tension-type headache. The reported prevalence of major depression should be considered with caution. By contrast, 17% of children with episodic tension-type headache reported depressive symptoms, which was significantly more often than in children without headache. In adults, no association has been found between major depression or anxiety and episodic tension-type headache (20), whereas an association between depressive symptoms and tension-type headache has been reported (21). The connection of depressive symptoms with tension-type headache may be bidirectional. Depressive mood can provoke headache in a person susceptible to headache (7, 22) or vice versa.
In the present study, the symptoms of oromandibular dysfunction were associated with episodic tension-type headache. This association is a routine observation in adults (23). However, our results did not agree with those of an earlier study (24), suggesting that headache is also one of the main symptoms of oromandibular dysfunction in children.
The lower social stratum of the family (25), unemployment (26) and higher parental divorce rate (8, 27) have been related to a higher prevalence of headache in children. In the present study, the fathers of children with episodic tension-type headache were lower-level white-collar workers, not independent traders or employees, significantly more often than the fathers of children without headache. However, episodic tension-type headache in children was not associated with a higher rate of one-parent families, unemployment or economic problems in families. The impact of social stratum on headache is problematic. Because data on unemployment, divorce and social stratum are too rough measures for acute or chronic stress, the results of different studies may be confusing and inconsistent.
In the present study, some basic characteristics of childhood tension-type headache were determined. Episodic tension-type headache appeared to be less frequent, and the episodes were less intensive and shorter than migraine attacks. No evidence exists, but we suspect that episodic tension-type headache in a child appears to the parents as less dangerous and less disabling than migraine, and it may be more often ignored by the parents than migraine. Tension-type headache in adults also causes less functional impairment than migraine. However, the total negative impact on life may be as heavy as that caused by migraine, but is perhaps of a different type (28). In addition, some children with episodic tension-type headache may develop chronic tension-type headache by adulthood, and it is vitally important to recognize these children and intervene.
Footnotes
Acknowledgements
This study was supported by the Foundation for Paediatric Research, Finland.