
Abstract
The aim of the study was to assess the prevalence of headache with special attention to tension-type headache (TTH) in a rural area in northern Tanzania. A door-to-door study was performed using a standardized and validated questionnaire. A total of 7412 participants were screened. The total headache prevalence during the past year was 12.1%; the overall 1-year prevalence of TTH was 7%; 5% reported episodic TTH and 0.4% chronic TTH. Borderline cases (International Headache Society code 2.3) were described in 1.6%. The prevalence of headache was highest in the 41-50-year-old group in women and in the 61+ age group in men. This is the first account of the prevalence of TTH in a rural Tanzanian population, and shows that headache in general and, more specifically, TTH are prevalent disorders that deserve attention. However, the prevalence of primary headache seems to be lower than in Western countries.
Introduction
Headache is one of the most frequent and widespread symptoms and, according to the World Health Organization (WHO), among the world's top 20 most disabling medical disorders (1), thus constituting a major health problem. Although tension-type headache (TTH) is the most common headache disorder and is associated with a large socioeconomic impact (2–4), only few studies have focused on its epidemiology (5).
More than 90% of the African population is estimated to live in rural areas with limited access to health facilities. Poor awareness among affected people and lack of knowledge among healthcare providers render headache a still underestimated, underrecognized and undertreated ailment in developing countries (2). In order to provide appropriate healthcare for the rural population, accurate information from community-based epidemiological studies is crucial.
Few population-based studies exist for developing countries, where limited funding together with the low profile of headache disorders compared with other diseases prevent the systematic collection of information (2, 5). Hence, information on prevalence rates of headache in the African population is still scarce. In industrialized countries, substantial data on headache have been compiled (5). However, observed results vary widely, mainly due to differences in classification and case definition, study methodology and population samples (6) as well as the influence of sociodemographic and psycho-social factors (4).
The introduction of the International Headache Society (IHS) criteria has led to explicit diagnostic criteria for all headache disorders and new opportunities for valid epidemiological headache research (7, 8). However, only few headache studies in Africa have used the IHS criteria for classification (9, 10). Often they have been limited to small and narrowly defined samples, such as students or clinical cases (11–13). Consequently, comparing these results with those of studies conducted in developed countries is questionable. Thus, the application of stringent, internationally valid diagnostic criteria is mandatory for epidemiological studies on headache. The aim of this epidemiological study was to investigate the overall prevalence of headache and, in particular, that of TTH in a rural African population applying the criteria of the IHS (7, 8).
Subjects and methods
Study site
The study was conducted within the catchment area of the Haydom Lutheran Hospital (HLH), which is situated in a remote rural area in northern Tanzania, Mbulu district, 300 km southwest of Arusha. The hospital serves a population of > 300 000. The total immediate catchment area of the hospital comprises 268 120 people and the total greater reference area is extrapolated to 1795 632 people.
Sampling procedure
The nearer catchment area of HLH, comprising the two districts closest to the hospital, was chosen as study area. It contains approximately 41 937 inhabitants and 6577 households (14). As the study area has a low migration rate and is not greatly different from other communities in the region, the characteristics of the sample were deemed representative of the entire catchment area (15). The study cross-sectional, using multistage cluster sampling, which has previously been shown to be the appropriate approach to obtain an acceptable sample size in our study area (16). The well-structured administrative system of Tanzania facilitated the sampling procedure. In detail, villages were chosen by distance from HLH, subvillages and 10-cells (= cluster) were selected by simple random sampling. A 10-cell is composed of at least 10 households under the leadership of a 10-cell leader. All people within one 10-cell were interviewed.
Survey and operational instruments
Between December 2003 and June 2004 a door-to-door survey was carried out using a pretested questionnaire in order to identify people with a history of headache. The team consisted of a neurologist, three last-year medical students and three well-trained secondary school graduates as interpreters. Verbal informed consent of each head of household and all eligible individuals was obtained and information about the objective of the study and its voluntary character was given. After collection of demographic details of the family, the following screening questions regarding headache were put to the head of household:
‘Have you or your family member got a headache at present?’
‘In your (his/her) life, have you or your family member ever had a headache?’
‘Did you (he/she) have a headache in the previous year?’
Subsequently, all headache sufferers identified by the screening were questioned in detail in a face-to-face interview. In order to minimize recall bias, the in-depth questionnaire was done only in subjects who had suffered from headaches within the previous year. Prior to the main study, a pilot study was carried out to test the overall methods in a village with features similar to the study area. This population was later excluded from analysis.
Diagnostic criteria and case definition
The questionnaire and diagnoses were based on the IHS criteria, which offer standardized and structured methods for taking a medical history in patients with headache (7, 8). In addition, the questionnaire was adjusted to that used in a study carried out in 1999 in southern Tanzania (10).
The term ‘screen-positive’ was applied to an individual who had had a headache in the year preceding the day of the interview, which was not due to other causes or illnesses. People who were screen-positive for headache completed an in-depth questionnaire by means of which detailed questions about clinical characteristics and specific headache features were asked. Subjects were diagnosed in accordance with the most frequent type of headache experienced in the previous year. TTH was diagnosed in those individuals meeting IHS criteria for episodic tension-type headache (ETTH), chronic tension-type headache (CTTH), and headache of the tension-type not fulfilling the above criteria (7, 8).
Ethical considerations
After approval by the Ethics Committee of the National Institute of Medical Research and permission from the Tanzania Commission for Science and Technology in Dar es Salaam, research permits of the regional administrations and district councils were sought and granted. Written informed consent was obtained from the community leaders as well as from the village, subvillage and 10-cell leaders.
Statistical analysis
For statistical analysis data were transferred from Excel into
Results
Study population
The study population comprised 7412 people and 1192 households. This corresponds to 18.1% of all households and 17.7% of all inhabitants in the study area. None of the households refused to cooperate. More than 90% of the households depended on subsistence farming. Almost half of the study population was found to be illiterate (46.7%). The population structure analysis revealed a gender ratio of 1.01:1 (Fig. 1). The mean age was 20.7 ± 18.5 years. The majority (60.5%) of the study population was aged < 20 years, reflecting the typical structure of a developing country (Fig. 1). Ninety-one participants (1.2%) did not know their age.
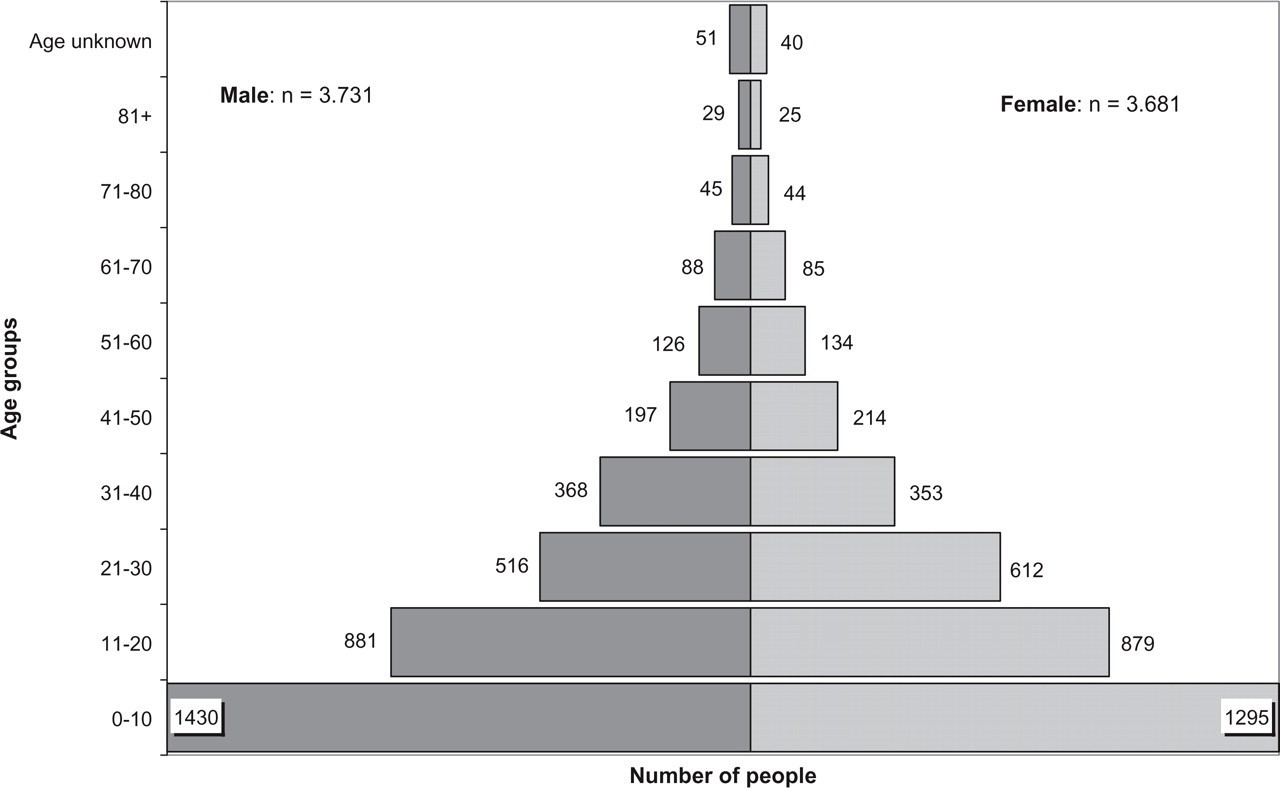
Distribution of the study population by age and gender (northern Tanzania, 2003/2004).
Overall headache
A total of 1404 of the study population stated that they had suffered from headaches in their lifetimes, corresponding to 18.9% (1404/7412; male 13.6%, 509/3731; female 24.3%, 895/3681). When patients who had experienced headache exclusively related to a concomitant medical condition were excluded, the remaining lifetime prevalence of overall primary headache was 13.5% (1004/7412; male 9.8%, 366/3731; female 17.3%, 638/3681).
The 1-year prevalence rate of overall primary headache was 12.1% (895/7412; 95% CI 11.3, 12.8). After age adjustment to the WHO population, the 1-year prevalence rate was 17.5%. The 1-year prevalence of headache was significantly higher in female [15.8% (583/3681); 95% CI 14.7, 17.1] compared with male subjects [8.4% (312/3731); 95% CI 7.5, 9.3], resulting in a male : female ratio of 1:1.9 (P < 0.001). The age- and gender-specific distribution of all headaches is shown in Fig. 2. The peak age-specific 1-year prevalence rate for all individuals and for women was found in the fifth decade with 26.5% (109/411; 95% CI 22.3, 31.1) and 35% (75/214; 95% CI 28.7, 41.8), respectively. In men, those aged ≥ 61 years showed the highest prevalence rate with 19.8% (32/162; 95% CI 13.9, 26.7).
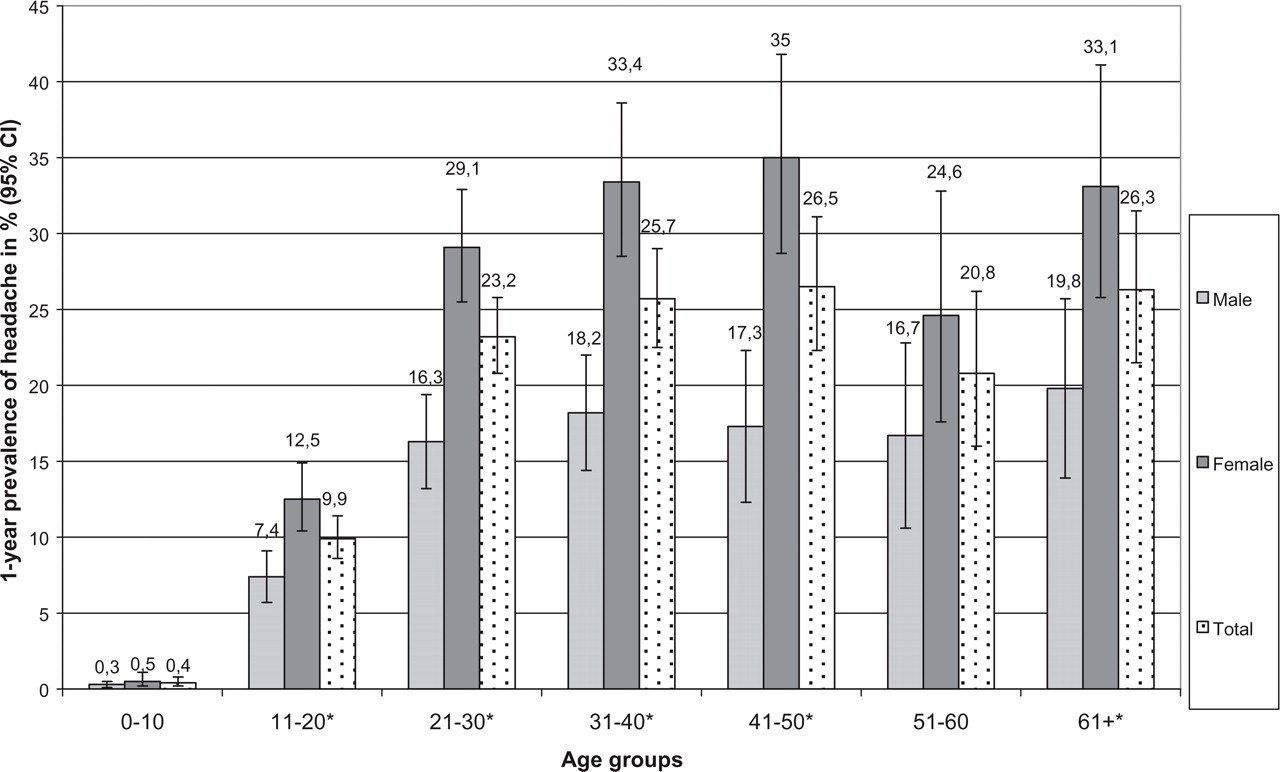
One-year prevalence of overall primary headaches by age and gender with 95% confidence interval in 2003/2004 in a rural area of northern Tanzania. ∗P < 0.01 (male : female ratio).
Tension-type headache
Five hundred and twenty-one headache sufferers met the case definitions of TTH, resulting in a 1-year TTH prevalence of 7% (521/7412, 95% CI 6.5, 7.6; age-adjusted rate 10.4%); 5.3% (196/3731; 95% CI 4.6, 6) in men compared with 8.8% (325/3681; 95% CI 7.9, 9.8) in women. Women outnumbered men with a gender ratio of 1:1.7 (P < 0.001). ETTH made up 5% (374/7412; 95% CI 4.5, 5.5; age-adjusted rate 7.1%), CTTH 0.4% (27/7412; 95% CI 0.2, 0.5; age-adjusted rate 0.5%) and TTH, according to IHS 2.3, 1.6% (120/7412; 95% CI 1.3, 1.9; age-adjusted rate 2.8%).
The mean age of patients with TTH was 36 ± 18.3 years. The age- and gender-specific distribution of TTH is shown in Fig. 3. The prevalence rates of TTH increased continuously until the fifth life decade (15.3%; 63/412; 95% CI 12, 19.2). The peak age-specific 1-year prevalence rate of 18.7% (59/316; 95% CI 14.5, 23.4) occurred in people > 60 years old in both genders, in men being 15.4% (25/162; 95% CI 10.2, 21.9) and in women 22.1% (34/154; 95% CI 15.8, 29.5). The female preponderance was significant in the second and fourth decades of life (P < 0.01).

One-year prevalence of tension-type headache by age and gender with 95% confidence interval in 2003/2004 in a rural area of northern Tanzania. ∗P < 0.01 (male : female ratio).
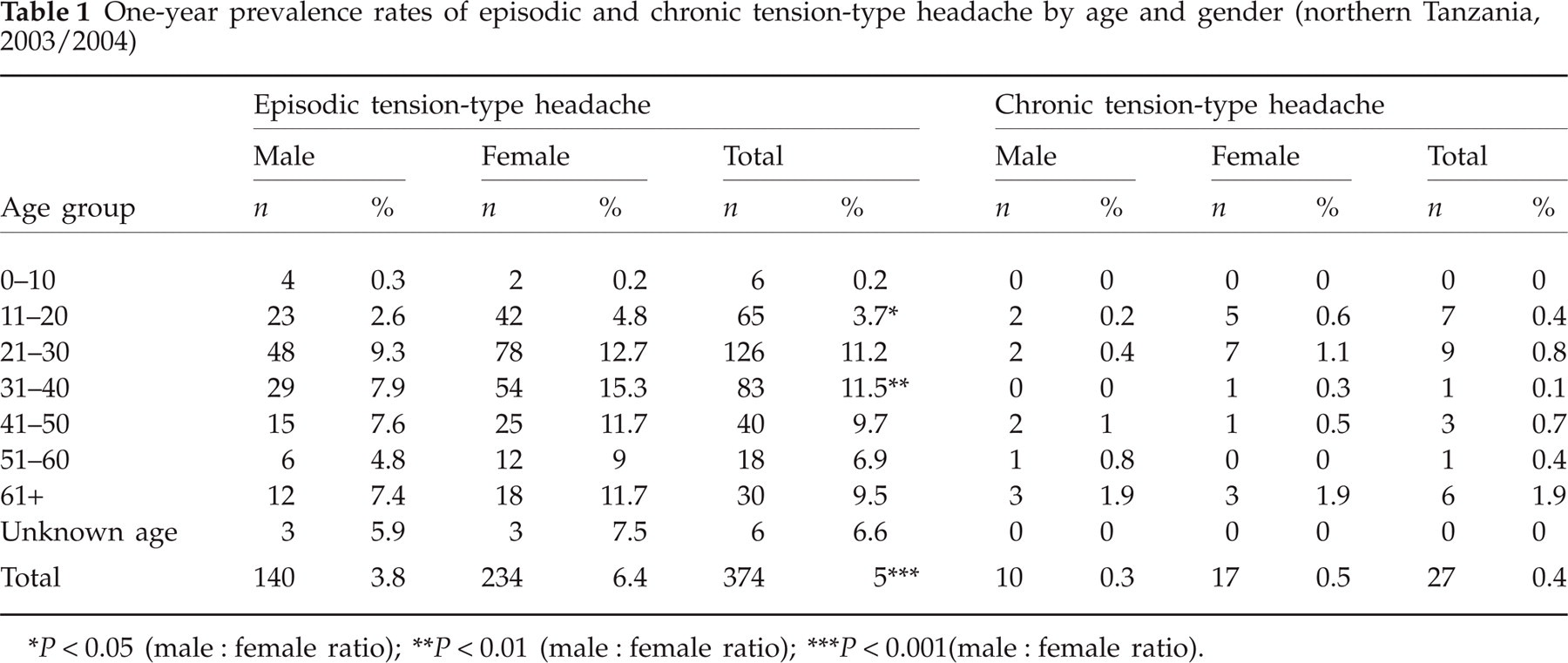
Episodic tension-type headache (Table 1)
Men were affected by ETTH in 3.8% of cases (140/3731; 95% CI 3.2, 4.4) and women in 6.4% (234/3681; 95% CI 5.6, 7.2) with a male : female ratio of 1:1.7 (P < 0.001). Contrary to overall TTH, the peak age-specific 1-year prevalence rate of ETTH was found in the fourth decade of life with 11.5% (83/721; 95% CI 9.3, 14.1); the same was seen in women with 15.3% (54/353; 95% CI 11.7, 19.5). In men, a maximum of ETTH cases was seen in the third decade, with a prevalence rate of 9.3% (48/516; 95% CI 7.0, 12.2). The female preponderance was significant in the second (P < 0.05) and fourth decades of life (P < 0.005).
One-year prevalence rates of episodic and chronic tension-type headache by age and gender (northern Tanzania, 2003/2004)
P < 0.05 (male : female ratio);
P < 0.01 (male : female ratio);
P < 0.001(male : female ratio).
Chronic tension-type headache (Table 1)
CTTH was found in 0.3% (10/3731; 95% CI 0.1, 0.5) of the interviewed men and in 0.5% (17/3681; 95% CI 0.3, 0.7) of the women with a male : female ratio of 1:1.7. The majority of people with CTTH was found to be > 61 years old with a prevalence rate of 1.9% (6/316; 95% CI 0.7, 4.1); for both genders, the observed peak prevalence rate of 1.9% (in men 3/162, 95% CI 0.4, 5.3; in women 3/154, 95% CI 0.4, 5.6) was found in elderly people.
Tension-type headache according to IHS 2.3 (Table 2)
Of men 1.2% (46/3731; 95% CI 0.9, 1.6) and of women 2% (74/3681; 95% CI 1.6, 2.5) reported this type of headache. The male : female ratio was 1:1.7 (P < 0.01). In patients who suffered from TTH according to IHS 2.3, the highest prevalence rates were found in people aged ≥ 61 years. In this age group, the overall prevalence rate was 7.3% (23/316; 95% CI 4.7, 10.7); in men it was 6.2% (10/162; 95% CI 3, 11.1) and in women 8.4% (13/154; 95% CI 4.6, 14).
One-year prevalence rates of tension-type headache (TTH) according to International Headache Society (IHS) 2.3 by age and gender (northern Tanzania, 2003/2004)

P < 0.01 (male : female ratio).
Discussion
Little is known about headache in rural Africa, and even less about TTH (Table 3) (5). In Tanzania, three studies on headache have been performed. Two dealt with TTH, but in a preselected population (12, 13). Two community-based studies have been published with 1-year and 2-year headache prevalence rates of 23.1% in a rural southern Tanzanian population and 23.7% in an urban population of students and workers in Dar es Salaam, respectively (10, 13). Another community-based African study, conducted in a rural area of Ethiopia, reported a 1-year prevalence rate of 4.7% in participants aged ≥ 20 years (9). The frequency of headache in an urban Zimbabwean population was 20.2% (18). In Asian and South-American studies with comparable methods, the 1-year prevalence of headache of all types ranged from 28.5 to 78.8% (5). In European and North-American studies, 1-year prevalence rates of headache varied between 13.4 and 87.3% (5). Headache in general appears to be a highly prevalent disorder worldwide, but seems to be least common in Africa.
Prevalence of overall headache and tension-type headache in African studies (exclusive of studies on migraine only)

?, not published; —, not calculated; AHC, Ad Hoc Committee Criteria; IHS, International Headache Society; comm, community-based.
We found a preponderance of women suffering from headaches, an observation similar to that of other studies in Africa (9, 10, 13, 18) and other parts of the world (19–26). In our study, the age-specific peak prevalence rate of all types of headache was found in the fifth decade of life. This is in accordance with two studies (Tanzania (10) and Puerto Rico (21)), although other studies have shown peak prevalence rates at younger ages (18, 23, 24, 26–28).
Data on the epidemiology of TTH are scant. Results do not compare well, as some studies, especially those from Africa, did not use the IHS criteria (Table 3). Three community-based African studies have published results on TTH (9, 13, 18). Matuja et al. found 35.8% of students and workers aged 20–40 years suffered from TTH (13). Haimanot et al. reported TTH in 1.7% of a rural population (9). Levy described features suggestive of TTH in 0.7% of an urban population, but subjects with rare episodes were not included (18). Matuja et al. and Levy classified TTH according to the Ad Hoc Committee criteria (13, 18). It is questionable whether reasonable comparison between the two classifications is possible. Haimanot et al., who used the IHS classification, only published CTTH (1.7%; (9)), which, however, was found to be more frequent than in our study (0.4%).
A few South-American and Asian studies have published prevalence rates of TTH (lifetime and 1-year prevalences) ranging from 12.9 to 66.2% (5). All studies applied IHS criteria for classification of TTH. In Europe and North America the following prevalence rates (lifetime and 1-year) for TTH were calculated: Finland 35% (29), Denmark 74% (3), Croatia 34.8% (30), Germany 38.3% (TTH, IHS 2.3: 0.3%; (31)) and USA 40.5% (ETTH 38.3%, CTTH 2.2%; (6)). It has to be taken into consideration that in Croatia (30) and Germany (31) lifetime prevalences were calculated. The prevalence rates of our study in northern Tanzania are much lower than those found in Europe and the USA (3, 6, 29–31) and Asia and South America (5). It has not been entirely explained why, in general, prevalence rates in Africa are low. Headaches may be perceived differently across cultures. Possibly villagers in an African rural setting may not easily recall vital information and events leading to a disease. This could be the consequence of higher pain thresholds, or the fact that headache is less noticed, especially milder forms of headache, compared with the threat of starvation and malaria among others. In addition, unacceptability in the family and community may be a cause for underreporting and low awareness of headache. The fact that the head of household was the main informant contributes to possible underestimation of headache occurrence. Furthermore, the threshold of recall probably varies with the severity and recency of the condition. Sociodemographic and socioeconomic risk factors such as education, income, marriage, etc. may account for the lower prevalence rates of headache. In summary, environmental factors, genetic differences or cultural diversity in the reporting of pain may explain the apparent difference in headache susceptibility in African and Western countries, and should be the topic of future research.
A preponderance of women suffering from TTH is consistent with findings of previously reported studies (6, 9, 11, 19, 20, 28–34) and does not seem to represent an African trait. Contrary to Rasmussen et al., who reports a decrease of prevalence rates with increasing age (3), we found the peak prevalence rate of overall TTH in people aged ≥ 61 years in both genders. A peak of TTH between 20 and 55 years has been reported in other studies (6, 20, 28–30, 32–35). In Saudi Arabia and Singapore more TTH was found in elderly people (19, 36). However, results of these studies refer to lifetime prevalence and could be explained as cumulative effect with increasing age. Stovner et al. reported that TTH is most prevalent in adults, i.e. covering at least age groups from 25 to 60 years (5). It seems that in Tanzanian rural communities TTH is a disease of elderly people. However, TTH could have been masked by more severe migraine in younger years, as migraine peaks in middle-age groups (37). If, in our study, ETTH and CTTH are regarded separately, a peak age-specific prevalence rate in patients with ETTH was found in the fourth decade (third decade in men and fourth decade in women), whereas the prevalence rate of CTTH increased with age. This tendency has been confirmed in several other studies (31, 33, 34) and may reflect the development of ETTH into a chronic form over a period of many years.
In conclusion, headache of all types is a common symptom in a rural population of Tanzania. Women are more affected than men. The prevalence increases with age in overall TTH as well as in CTTH and peaks in the fourth decade in ETTH. Prevalence rates are lower than those reported from other continents, but within published results of African studies. Variation in prevalence rates may partly be due to differences in methodology and definitions, as well as geographical, socioeconomic, dietary, cultural and racial factors.
Acknowledgements
Our especial thanks go to the population involved and to all our local helpers, without whom this study would not have been possible. A.S.W. was supported by The Centre for International Migration, Frankfurt, Germany.