
Abstract
The aim of this study was to determine whether scalp tenderness and photophobia, two well-recognized symptoms of migraine, develop during the motion sickness induced by optokinetic stimulation. To investigate whether motion sickness has a general influence on pain perception, pain was also assessed in the fingertips. After optokinetic stimulation, nausea increased more and headache persisted longer in 21 migraine sufferers than in 15 non-headache controls. Scalp tenderness increased during optokinetic stimulation in nauseated subjects, and pain in the fingertips increased more and photophobia persisted longer in migraine sufferers than controls. These findings suggest that the disturbance responsible for nausea also sensitizes trigeminal nociceptive neurones or releases inhibitory controls on their discharge. A low nausea threshold and a propensity for sensitization to develop rapidly in nociceptive pathways may increase susceptibility to migraine.
Introduction
Migraine sufferers appear to be more susceptible than most other people to motion sickness. For example, over 50% of migraine patients surveyed by Kayan and Hood (1) reported a history of motion sickness compared with only 20% of tension headache sufferers. Motion sickness is also strongly linked with migraine in children (2–4) and university students (5).
Damage caused by episodic ischaemia of the labyrinth during attacks of migraine might increase susceptibility to motion sickness (6). In support of this view, vestibular disturbances are common in migraine sufferers, particularly when attacks are accompanied by vertebrobasilar symptoms (1, 7, 8). However, other mechanisms may also increase susceptibility to motion sickness. Migraine is associated with recurrent abdominal pain in childhood (9) and susceptibility to motion sickness and migraine greatly increases the likelihood of vomiting after a mild head injury (10). In addition, apomorphine provokes nausea and vomiting more readily in adult migraine sufferers than controls (11). Taken together, these findings suggest that a low threshold for nausea and vomiting contributes to the migraine predisposition and might also increase susceptibility to motion sickness.
Motion sickness results from a sensory conflict or ‘neural mismatch’ between the visual system and the vestibular and proprioceptive modalities (12, 13). In air and sea sickness, symptoms develop when sensations of movement do not match visual input. Symptoms of motion sickness also develop during optokinetic stimulation when the visual perception of movement does not match vestibular and proprioceptive sensations (e.g. while watching wide-screen movies) (14). Recognition of a mismatch activates the brain stem nuclei that mediate gastrointestinal disturbances and other symptoms of motion sickness. Apart from nausea, motion sickness is associated with upper abdominal sensations, sleepiness, apathy, dizziness and headache, that is, many of the symptoms of migraine. Thus, motion sickness and migraine may share a final common pathway, possibly involving the brain stem nuclei that mediate symptoms in these two conditions.
The main aim of the present study was to look for further parallels between the symptoms of motion sickness and those of migraine. In particular, the aim was to determine whether scalp tenderness and photophobia, two well-recognized symptoms of migraine, develop during the motion sickness induced by optokinetic stimulation. As the vestibular apparatus is not actively stimulated by the optokinetic procedure, vestibulocochlear dysfunction could not be responsible for symptoms of motion sickness during optokinetic stimulation. Instead, any difference between migraine sufferers and controls would be consistent with activation of the final common pathway responsible for symptoms that develop in motion sickness and migraine.
The second aim was to investigate whether motion sickness has a general influence on pain perception. Burstein et al. (15, 16) reported that cutaneous allodynia sometimes spread beyond the area of referred pain during attacks of migraine to include the upper limbs. They postulated that central sensitization could spread from second order trigeminal neurones in the brain stem to third order nociceptive neurones in the thalamus. Alternatively, allodynia extending beyond the area of referred pain could result from failure of central pain-modulating mechanisms. Even during the headache-free interval, modulation of nociceptive visceral signals may be disrupted in migraine sufferers. For example, Nicolodi et al. (17) reported that venous distension and injection of hypertonic saline into the antecubital vein provoked pain more readily in migraine sufferers than controls. Therefore, it was hypothesized that sensitivity to pain in the fingertips would increase after optokinetic stimulation in migraine sufferers.
Method
Subjects
The migraine sample consisted of 21 women aged between 18 and 50 years (mean age 27 ± 10 years) who met International Headache Society criteria (18) for migraine with aura (seven subjects) or migraine without aura (14 subjects). Headaches recurred, on average, at least once per month. Eight subjects took ergotamine or sumatriptan to relieve their attacks, whereas the remainder took only analgesic medication. Six subjects had experienced a migraine within the past week. However, only one subject had taken ergotamine during this period and none of the 21 subjects took migraine medication prophylactically. The control group consisted of 15 women aged between 18 and 38 years (mean age 26 ± 7 years) who did not suffer from migraine and who only rarely experienced other forms of mild headache. Three of these women reported a history of migraine in one of their first-degree relatives. However, a family history of migraine was not an exclusionary criterion for controls because a similar history was obtained in only 15 of the 21 migraine sufferers.
Subjects were recruited by advertisement from students and staff of Murdoch University and were paid $10 for participating. Each gave their informed consent for the procedures, which were approved by the local ethics committee.
Procedure
Scalp tenderness
Scalp tenderness was assessed using an algometer with a 2-mm diameter hemispherical probe tip. To induce sensations of mild to moderate pain, the probe tip was applied to each side of the forehead at four pressures (85 gm, 170 gm, 255 gm and 340 gm). Pressure was applied for 5 s to discrete sites 1–4 cm above the eyebrow and 1–4 cm from the midline. The order of stimulation (in terms of site and pressure) varied randomly within and between subjects from one test to the next. After each stimulus, the subject rated pain intensity verbally on a scale ranging from 0 (not painful) to 10 (extremely painful). The experimenter recorded this rating and then applied the next stimulus.
Pain elsewhere
The same procedure was used to assess pain sensations in the fingertips. The probe tip of the algometer was applied close to the join between the fingernail and fingertip on each finger of each hand (excluding the thumb) at one of four pressures (85 gm, 170 gm, 255 gm and 340 gm; stimulus duration 5 s). The order of stimulation (in terms of fingertip and pressure) varied randomly within and between subjects from one test to the next.
Photophobia
Before investigating sensitivity to light, the subject adapted to darkness in a small room for several minutes. She was then asked to look at the light emitted from a 50-watt halogen globe positioned 40 cm in front of her eyes. The power supply of the globe was regulated to produce an illumination of 1000 lux for 2 s (measured at the position of the subject's eyes by a Gossen Profisix lightmeter with a Profilux attachment). The subject rated glare from 0 (no glare) to 10 (the most dazzling light she had ever seen), and pain from 0 (not painful) to 10 (extremely painful). The light was presented three times at 30-s intervals.
Optokinetic stimulation
To induce symptoms of motion sickness, the subject sat on a stationary chair with her head and shoulders inside a drum 50 cm in diameter, 70 cm in height and painted internally with 24 pairs of vertical black and white stripes (19). The drum revolved 10 times per min for 15 min, or until the subject thought that she was about to vomit. In susceptible subjects, the moving stripes appeared to slow down or stop during drum rotation whereas the stationary chair the subject was sitting on appeared to spin. The mismatch between the visual illusion of movement and opposing vestibular and proprioceptive sensations induced motion sickness. Immediately after the optokinetic stimulation, the subject rated symptoms of motion sickness (dizziness, nausea, body warmth, sweating and headache) on scales where 0 corresponded to ‘none’ and 10 to ‘extreme’. Residual symptoms of motion sickness were rated 30 min later.
Test sequence
Scalp tenderness, photophobia and sensitivity to mechanical stimulation of the fingertips were assessed before and shortly after optokinetic stimulation, and after 30 min of recovery from optokinetic stimulation. Photophobia was assessed before scalp tenderness and pain sensations in the fingertips on 50% of occasions. In addition, pain sensations were assessed in the fingertips before pressure was applied to the forehead on 50% of occasions.
Reliability of repeated pain assessments
Pain sensitivity was assessed on another occasion in 16 migraine sufferers and 12 controls. On this occasion, scalp tenderness, photophobia, and sensitivity to mechanical stimulation of the fingertips were assessed three times at 30-min intervals, in the absence of optokinetic stimulation. In seven cases this session preceded the session that included optokinetic stimulation.
Statistical approach
As preliminary analyses indicated that findings did not differ between subjects with or without a history of migraine aura, migraine sufferers formed a single category in subsequent analyses. Symptoms of motion sickness (dizziness, nausea, body warmth, sweating and headache) were compared between migraine sufferers and controls in a multivariate analysis of variance with one repeated measures factor (immediately after optokinetic stimulation vs. 30 min later). Ratings of scalp tenderness and pain sensations in the fingertips were averaged over the four application pressures to minimize floor and ceiling effects. Changes in these scores and in mean ratings of glare and light-induced pain were investigated in 2 × 3 [group (migraine, control) × block (before optokinetic stimulation, after optokinetic stimulation, 30 min later)] analyses of variance. The multivariate solution was used for the repeated measures factor. Rating changes over repeated assessments, and in relation to the intensity of nausea and headache after optokinetic stimulation, were investigated in similar analyses.
Results
Symptoms of motion sickness
Two of the 15 controls and five of the 21 migraine sufferers withdrew from the optokinetic drum before the full 15 min of stimulation because they thought that they were about to vomit (difference between groups not significant). In combination, symptoms of motion sickness did not differ consistently between migraine sufferers and controls (multivariate F(5,30)=1.16, not significant). Nevertheless, nausea was greater in migraine sufferers (F(1,34)=5.95, P < 0.05) (Fig. 1). Symptoms subsided during the 30-min recovery period (multivariate F(5,30)=35.6, P < 0.001).


Ratings of tenderness in response to mechanical stimulation of the forehead in (a) migraine sufferers (▪) and controls (□), and (b) subjects who were mildly (□) or severely nauseated (▪) after optokinetic stimulation.
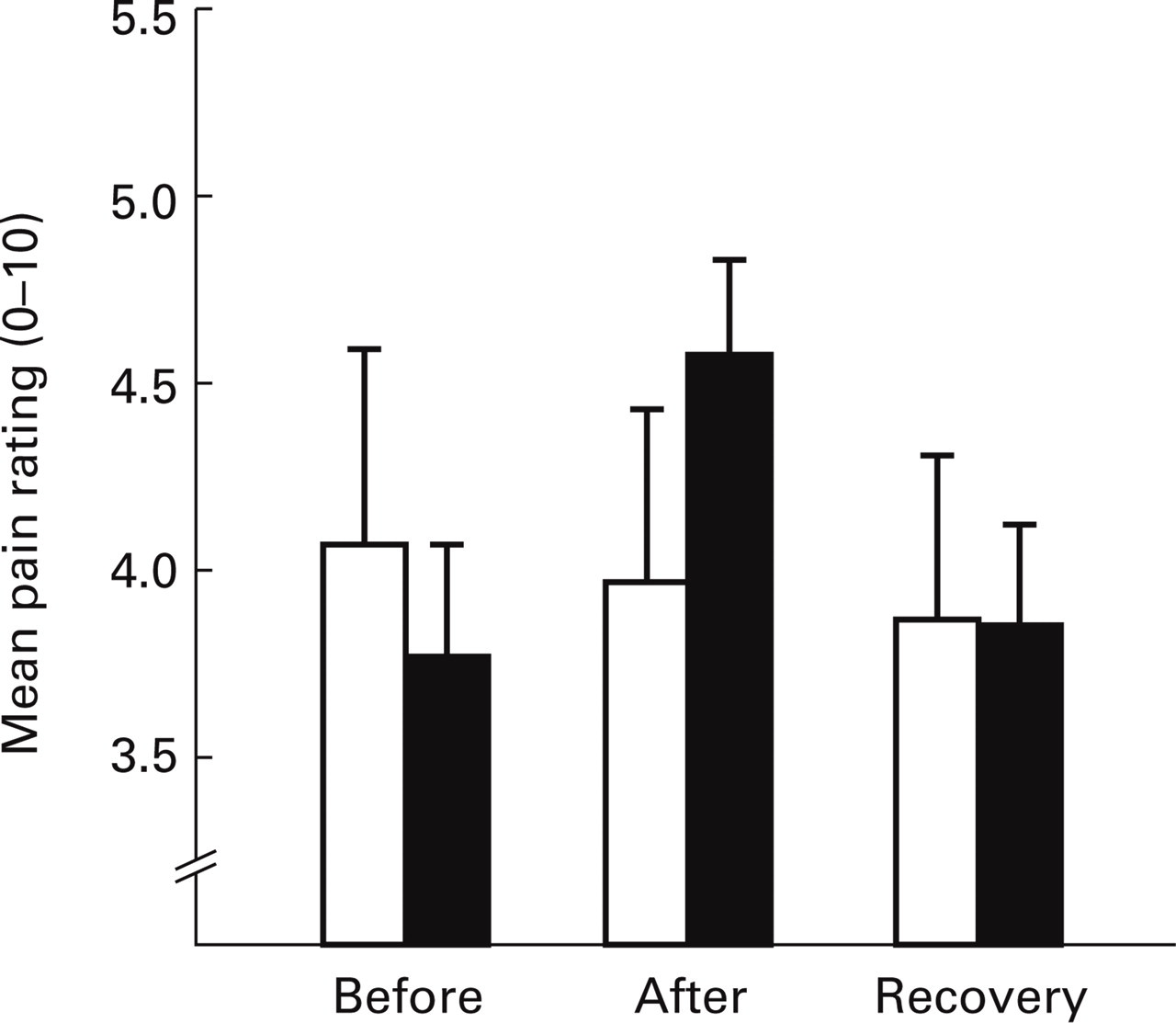
Pain ratings in response to mechanical stimulation of the fingertips in migraine sufferers (▪) and controls (□).
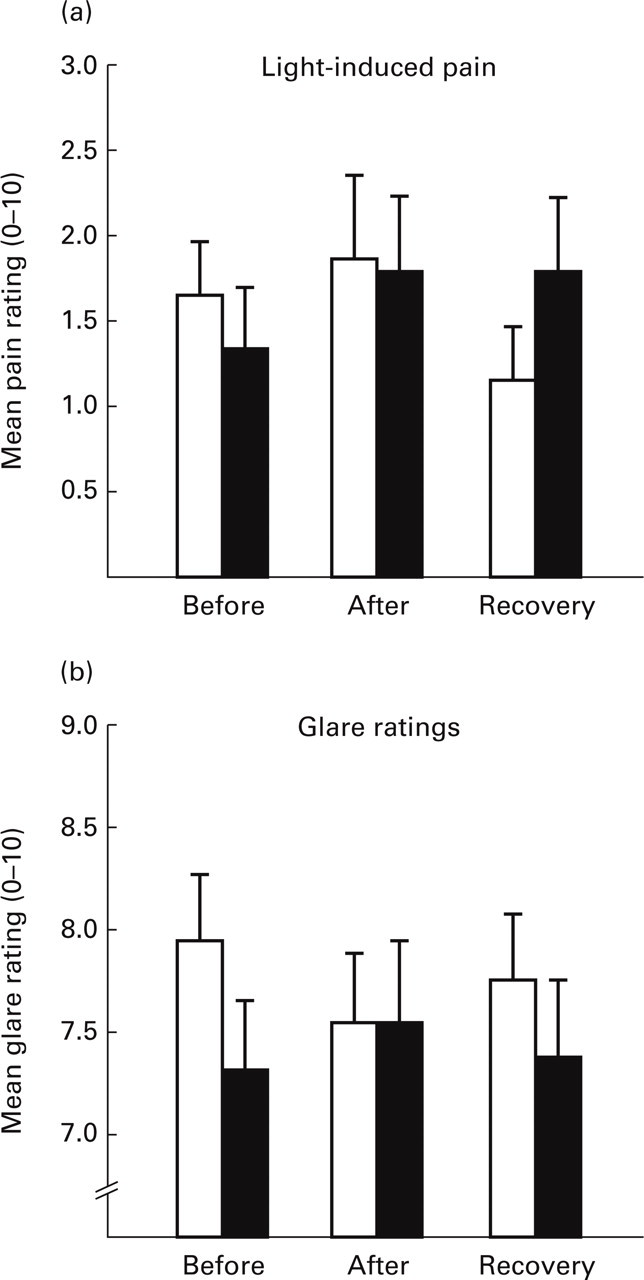
Ratings of (a) light-induced pain and (b) glare in migraine (▪) sufferers and controls (□).
Headache developed during optokinetic stimulation in 10 of 15 controls and 14 of 21 migraine sufferers. Most subjects described a dull ache across the forehead, in the temples or behind the eyes, but three migraine sufferers and one control reported that the headache was more intense on one side of the head. The headache was throbbing in three migraine sufferers and two controls (neither with a family history of migraine). Only one of the three controls with a family history of migraine reported any headache after optokinetic stimulation. This subject described a mild non-throbbing left-sided ache (rated 1 out of 10 in terms of intensity).
Headache ratings did not differ consistently between groups shortly after optokinetic stimulation. However, ratings were significantly greater in migraine sufferers than controls 30 min later (2.8 ± 0.5 vs. 1.1 ± 0.4, t(34)=2.25, P < 0.05). Headache straight after optokinetic stimulation was greatest in subjects who reported most light-induced pain at baseline (r(28)=0.57, P < 0.001) and after optokinetic stimulation (r(28)=0.53, P < 0.01), but was unrelated to ratings of glare, scalp tenderness or pain in the fingertips either before or after optokinetic stimulation.
Scalp tenderness
Ratings of scalp tenderness increased to a similar extent in migraine sufferers and controls after optokinetic stimulation, and returned towards baseline 30 min later (main effect for block, F(2,33)=11.87, P < 0.001) (Fig. 2a). Twenty-one subjects developed severe nausea (a rating of 6 or more) during optokinetic stimulation, whereas 15 subjects had no nausea or reported only mild nausea (a rating of 5 or less). As shown in Fig. 2(b), the increase in scalp tenderness after optokinetic stimulation was more pronounced in severely nauseated subjects than in those with mild nausea (nausea–block interaction, F(2,33)=5.40, P < 0.01). Scalp tenderness was unrelated to headache intensity. In the absence of optokinetic stimulation, ratings of scalp tenderness averaged 4.3 (mildly to moderately painful) and did not change significantly over three measurements repeated at 30-min intervals.
Pain sensations in the fingertips
Pain ratings increased in migraine sufferers but not in controls after optokinetic stimulation (group–block interaction, F(2,33)=5.36, P < 0.01) and returned towards baseline 30 min later (Fig. 3). The increase in pain ratings after optokinetic stimulation was unrelated to the intensity of nausea or headache. In the absence of optokinetic stimulation, pain ratings decreased from 4.3 to 3.9 over the three repeated measurements in both groups (main effect for block, F(2,25)=3.56, P < 0.05).
Photophobia
Light-induced pain increased slightly in both groups after optokinetic stimulation. During the 30-min recovery period, light-induced discomfort persisted in migraine sufferers but decreased in controls (group–block interaction, F(2,27) = 3.87, P < 0.05) (Fig. 4a). the increase in light-induced pain after optokinetic stimulation was unrelated to the intensity of nausea or headache. In the absence of optokinetic stimulation, ratings decreased from 1.6 to 1.2 when measurements were repeated three times (change over all three measurements, F(2,25)=2.79, P < 0.1; decrease from the first to the second measurement, F(1,26)=5.58, P < 0.05).
Glare ratings did not change in either group after optokinetic stimulation (Fig. 4b), or after repeated measurements in the absence of optokinetic stimulation (mean rating 7.1). Glare ratings were unrelated to the intensity of nausea or headache.
Discussion
Migraine sufferers generally have a low tolerance for bright light and loud noise (20–25), and a dull background headache persists between intermittent attacks of migraine in around 20% of patients who attend specialist treatment centres (26). These observations suggest that some of the disturbances responsible for symptoms of migraine persist subclinically and could increase the likelihood of recurrent attacks.
In the present study, nausea increased more and headache persisted longer after optokinetic stimulation in migraine sufferers than controls. Scalp tenderness increased during optokinetic stimulation in nauseated subjects, and pain sensitivity in the fingertips increased more and light-induced pain persisted longer in migraine sufferers than controls. In sum, optokinetic stimulation provoked symptoms associated with migraine, particularly in subjects with a migraine predisposition.
Symptoms of motion sickness
Ratings of nausea were greater in migraine sufferers than controls after optokinetic stimulation. As the vestibular apparatus was not directly stimulated during the optokinetic procedure, this finding is unlikely to be due to vestibulocochlear dysfunction in migraine sufferers. The sensory conflict responsible for generating symptoms of motion sickness during optokinetic stimulation could arise in the vestibular nuclei, because vestibular neurones encode moving visual fields in the absence of rotation (27). However, vestibular neurone dysfunction is unlikely to be the source of increased nausea in migraine sufferers because other symptoms of motion sickness (dizziness, body warmth and sweating) did not differ between the two groups. As nausea precedes vomiting, it seems plausible that nausea is associated with the prodromal activation of neurones in the nucleus tractus solitarius that coordinate emesis (28); in addition, higher centres (e.g. the inferior frontal gyrus of the cerebral cortex) may bring sensations of gastrointestinal discomfort into conscious awareness (29). The present findings support the view that neurones involved in encoding gastrointestinal disturbances are more responsive than normal in migraine sufferers (10, 11).
Migraine and tension headache appear to form the extremes in a continuum of headache activity (30). In the middle of this continuum are patients who report a persistent low-grade or fluctuating headache associated sporadically with migrainous symptoms such as nausea and dizziness (30), thus resembling the headache that developed during optokinetic stimulation. A headache more closely resembling migraine appears to develop during sea sickness (31), presumably because the severity of the motion sickness intensifies the headache. Plasma levels of calcitonin gene-related peptide are elevated in a subgroup of chronic tension headache sufferers with throbbing headache both during episodes of headache and interictally (32), suggesting that this form of headache is related to migraine. Unfortunately, the incidence of throbbing headache was too low to establish whether symptoms of motion sickness in subjects with throbbing headaches differed from the symptom profile associated with constant, dull headaches.
Headache developed to the same extent in migraine sufferers and controls after optokinetic stimulation. However, the persistence of the headache in migraine sufferers suggests that a mechanism that suppresses head pain may not work efficiently in people with a migraine predisposition. Susceptibility to the headache induced by optokinetic stimulation in non-headache controls did not seem to depend on a family history of migraine, although the small number of subjects in this category obviously limits generalizations about this observation.
Scalp tenderness
Burstein et al. (33) postulated that central trigeminal neurones that receive convergent input from meningeal perivascular fibres and the facial skin become sensitized during migraine. Burstein et al. (15, 16) subsequently demonstrated that cutaneous allodynia to thermal and mechanical stimulation developed within and outside the area of referred pain during migraine attacks. In the present study, scalp tenderness developed acutely during motion sickness in association with nausea rather than headache. This raises the possibility that the disturbance responsible for nausea also sensitizes central trigeminal neurones, or releases inhibitory influences on trigeminal discharge.
Neurones in the medullary nuclei of the solitary tract respond to a range of inputs that elicit nausea and vomiting, including noxious gastric distension and administration of emetic drugs (34, 35). Some neurones in this region receive convergent signals from vestibular nuclei and gastrointestinal afferents, and could mediate motion sickness-related vomiting (28, 36). Importantly, subcutaneous injection of formalin into the vibrissal pad of awake rats and electrical stimulation of trigeminovascular afferents in the superior sagittal sinus of monkeys activates nuclei in the caudal part of the solitary tract (37, 38). Furthermore, axons project from the nucleus tractus solitarius towards the dorsal medullary raphe and the trigeminal nucleus caudalis in humans (39). Therefore, an anatomical substrate exists for reciprocal communication between the nucleus tractus solitarius and the trigeminal nuclei that mediate headache and facial pain. It is tempting to speculate that the increase in scalp tenderness in nauseated subjects during optokinetic stimulation was due to a direct excitatory influence of solitary tract nuclei on the trigeminal nucleus caudalis, or to a disruptive influence of solitary tract nuclei on pain modulating circuits in the medulla. If this is the case, activity in nuclei of the solitary tract may help to sensitize central trigeminal neurones which, in turn, mediate scalp tenderness and other symptoms of migraine. Additional mechanisms appear to maintain central sensitization because scalp tenderness persists for several days after attacks of migraine, when other symptoms have resolved (40).
Pain in the fingertips
Sensitivity to pain in the fingertips increased in migraine sufferers but not controls after optokinetic stimulation and was unrelated to the intensity of nausea or headache. Burstein et al. (15, 16) speculated that sensitization could spread from trigeminal nuclei during attacks of migraine to involve nociceptive neurones in the thalamus. Alternatively, disruption to pain modulating systems (responsible, for example, for stress-induced analgesia or diffuse noxious inhibitory controls) could release inhibitory influences on pain sensations. The influence of pain modulating systems on hyperalgesia during motion sickness requires further investigation.
Photophobia
Painful stimulation of the face intensifies visual discomfort in migraine sufferers (21, 22). Conversely, bright light may increase scalp tenderness (22, 41) and usually aggravates headache. An escalating interaction between sensory stimulation and head pain could explain why bright lights, loud noise and strong smells can trigger attacks of migraine. In the present study, the strong association between light-induced pain at baseline and headache intensity after optokinetic stimulation suggests that the prior presence of photophobia increased the likelihood of headache.
In previous studies, photophobia persisted to some extent in migraine sufferers during the headache-free interval (20–25, 41). In the present study, however, ratings of glare and light-induced pain initially were similar in migraine sufferers and controls. Headache susceptibility on the day of investigation probably was lower in the present migraine sample than in studies where subjects were recruited from specialist treatment clinics, perhaps accounting for low ratings of light-induced pain at baseline. Nevertheless, the persistence of light-induced pain in migraine sufferers after optokinetic stimulation suggests that photophobia developed readily. In contrast to ratings of light-induced pain, glare ratings did not change after optokinetic stimulation and were similar in migraine sufferers and controls. Glare ratings do not increase during headache (20), implying that photophobia in migraine is linked more closely with pain processing than with other aspects of visual perception.
Implications for treatment of migraine
Various forms of sensory stimulation appear to interact with the sensitized trigeminal system during attacks of migraine to produce unpleasant sensations such as photophobia. As certain symptoms of migraine persist subclinically during the headache-free interval, trigeminal sensitization may also persist subclinically between attacks or develop rapidly to minor provocations. If so, treatments that reduce or prevent trigeminal sensitization should also reduce the frequency of recurrent attacks of migraine. As trigeminal stimulation increases light-induced pain (21, 22), photophobia might serve as a useful marker of trigeminal sensitization and current susceptibility to headache.
The susceptibility of migraine sufferers to nausea during optokinetic stimulation suggests that a persistent subclinical disturbance, presumably originating in brain stem nuclei, increases susceptibility to motion sickness and migraine. During migraine, antiemetics such as domperidone alleviate gastrointestinal disturbances and sensitivity to light and sound but are less effective at relieving headache than treatments such as sumatriptan (42). Nevertheless, when combined with paracetamol, domperidone appears to be as effective as orally administered sumatriptan in relieving headache and gastrointestinal symptoms (43). Unfortunately, side-effects currently limit the utility of employing antiemetics prophylactically (42). However, domperidone is more effective than placebo at preventing attacks of migraine if taken during the migraine prodrome (44, 45), suggesting that nausea develops early in the attack and initiates other symptoms.
Footnotes
Acknowledgements
This project was supported by the UK Migraine Trust and the National Health and Medical Research Council of Australia. I wish to thank Ms Ashley Frew for her assistance in data collection, and the subjects for tolerating the procedures.