
Abstract
The objective of this study was to estimate the 1-year prevalence of the following categories of headache; migraine, non-migrainous headache, frequent headache (> 6 days/month), and chronic headache (> 14 days/month). Between 1995 and 1997, all 92 566 inhabitants 20 years and older in Nord-Trøndelag county in Norway were invited to a comprehensive health study. Out of 64 560 participants, a total of 51 383 subjects (80%) completed a headache questionnaire. The overall age-adjusted 1-year prevalence of headache was 38% (46% in women and 30% in men). The prevalence of migraine was 12% (16% in women and 8% in men), and for non-migrainous headache 26% (30% in women and 22% in men). For frequent headache (> 6 days per month) and for chronic headache (> 14 days per month), the prevalence was 8% and 2%, respectively. Women had a higher prevalence than men in all age groups and for all headache categories. Prevalence peaked in the fourth decade of life for both men and women, except for ‘frequent non-migrainous headache’, which was nearly constant across all age groups in both genders. In accordance with findings in other western countries, we found that headache suffering, including migraine, was highly prevalent, especially in younger women.
Keywords
Introduction
Headache is a common discomfort (1–4), but our understanding of the epidemiology of headache disorders is incomplete. The study of headache epidemiology can address a number of important questions, e.g. the variation in the occurrence and severity of headache in the population, and the relationship between headache and other medical disorders. These studies may provide clues to abortive treatments, preventive strategies, or to the pathophysiology of headache (5).
The present study is the headache part of a large general health study in which all adult inhabitants in a single county in Norway were invited to participate. Problems related to sampling methods could therefore be avoided. Since the study included a wide spectrum of health-related variables, it is possible not only to describe the prevalence of headache, but also to relate headache to many other factors. The aim of the present study was, however, to describe the 1-year prevalence of migraine, non-migrainous headache, frequent headache (> 6 days/month), and chronic headache (> 14 days/month). This is the first study in Norway using recent diagnostic criteria (6, 7) to estimate the prevalence of chronic headache and migraine. The study, which includes a large number of participants over a wide age range, represents the cross-section of a planned longitudinal cohort study of headache disorders.
Materials and methods
Between 1995 and 1997, all inhabitants ≥ 20 years old in Nord-Trøndelag County in Norway were invited to participate in the Nord-Trøndelag Health Survey (‘Helseundersøkelsen i Nord-Trøndelag’=HUNT). Nord-Trøndelag is one of 19 Norwegian counties, and is located in the middle part of the country. The population is scattered, and no city has more than 21 000 inhabitants.
In Fig. 1, the population samples that participated in the different parts of the study are shown. Out of 92 566 invited individuals, 64 560 (70%) answered the first questionnaire (Q1) that was enclosed with the invitation letter, and participated in a brief medical examination, at which they were given a second questionnaire (Q2) to be filled in and returned from home. The two questionnaires included more than 200 health-related items, and the Q2 included 13 headache questions, mainly designed to determine whether the person suffered from headache or not, and whether he or she fulfilled the migraine criteria of the International Headache Society (IHS) (6). A total of 51 383 subjects (80% of the participants) completed the headache questions in Q2, and these constituted the ‘head-HUNT’ study.

Diagram of the population according to type of participation.
A total of 41 183 invited persons who did not answer the headache questions in Q2 were defined as non-participants. Among those, 28 006 did not answer Q1 (‘complete non-participants’). In this group, information about age, gender and marital status was available from the Norwegian Central Person Registry (Fig. 1). A total of 13 177 attended the screening but answered only the first questionnaire (Q1), including questions about education, employment status and general health status (‘partial non-participants’).
Organization and ethics
The survey was carried out by the National Health Screening Service in co-operation with the National Institute of Public Health, Nord-Trøndelag County, and the Norwegian University of Science and Technology (NTNU) in Trondheim. The study was approved by the Regional Committee for Ethics in Medical Research and the Norwegian Data Inspectorate.
Headache diagnoses
Subjects who answered ‘yes’ to the question ‘Have you suffered from headache during the last 12 months?’ were classified as headache sufferers. Frequent headache was defined as headache occurring > 6 days, and chronic headache > 14 days per month. For migraine, we used the diagnostic criteria of the IHS (6) with some modifications. Based on data from the headache questions in Q2, the diagnoses of migraine with or without aura were made according to three different sets of criteria: (i) most restrictive; (ii) medium restrictive; and (iii) liberal (Table 1). Headache not fulfilling the liberal set of migraine criteria was defined as non-migrainous headache.
Different sets of criteria for the diagnosis of migraine based on information in the questionnaire

Migraine with aura: identical to the criteria for migraine without aura, except: (i) headache attacks lasting ≤ 72 h and (ii) often visual disturbances prior to headache.
Validity and reliability of the headache diagnosis
The relative merits of these criteria have been evaluated in detail in a previous study (8). Briefly, the questionnaire-based headache diagnoses were compared with the diagnoses made in a clinical interview in 167 subjects. For migraine, using the liberal criteria set, the positive and negative predictive values were 84% and 78%, respectively, and the chance-corrected agreement (κ) was 0.59 (confidence interval (CI) 0.47–0.71), which is considered good. For non-migrainous headache, positive and negative predictive values were 68% and 76%, respectively, and there was a moderate agreement of 0.43 (0.29–0.57). For headache suffering, frequent headache (headache > 6 days per month), and chronic headache (headache > 14 days per month), the κ values were 0.57, 0.50, and 0.44, respectively (8), which indicate good to moderate agreement.
Statistical analysis
For the various headache categories, prevalence in men and women was estimated separately by age decade. The overall prevalence was age-adjusted, using the age distribution of all inhabitants aged ≥20 years in Nord-Trøndelag County as the standard population. For continuous variables, differences between means were tested with analyses of variance (one-way
Results
The age-adjusted prevalence of headache was 45.7% among women and 29.6% among men (total 37.7%). A total of 6209 subjects (11.6% age-adjusted) fulfilled the liberal criteria for migraine (15.6% for females and 7.5% for men) (Table 2). Out of these, 3539 individuals (9.4% women and 3.9% men) satisfied the medium restrictive criteria, of whom 1136 subjects (total 2.2%, 3.2% women and 1.0% men) fulfilled the most restrictive criteria. The age-adjusted prevalence of non-migrainous headache was 30.1% for women and 22.1% for men (Table 2).
Age- and sex-specific 1-year prevalence (%) and sex ratio∗ of headache, migraine (liberal criteria set) and non-migrainous headache
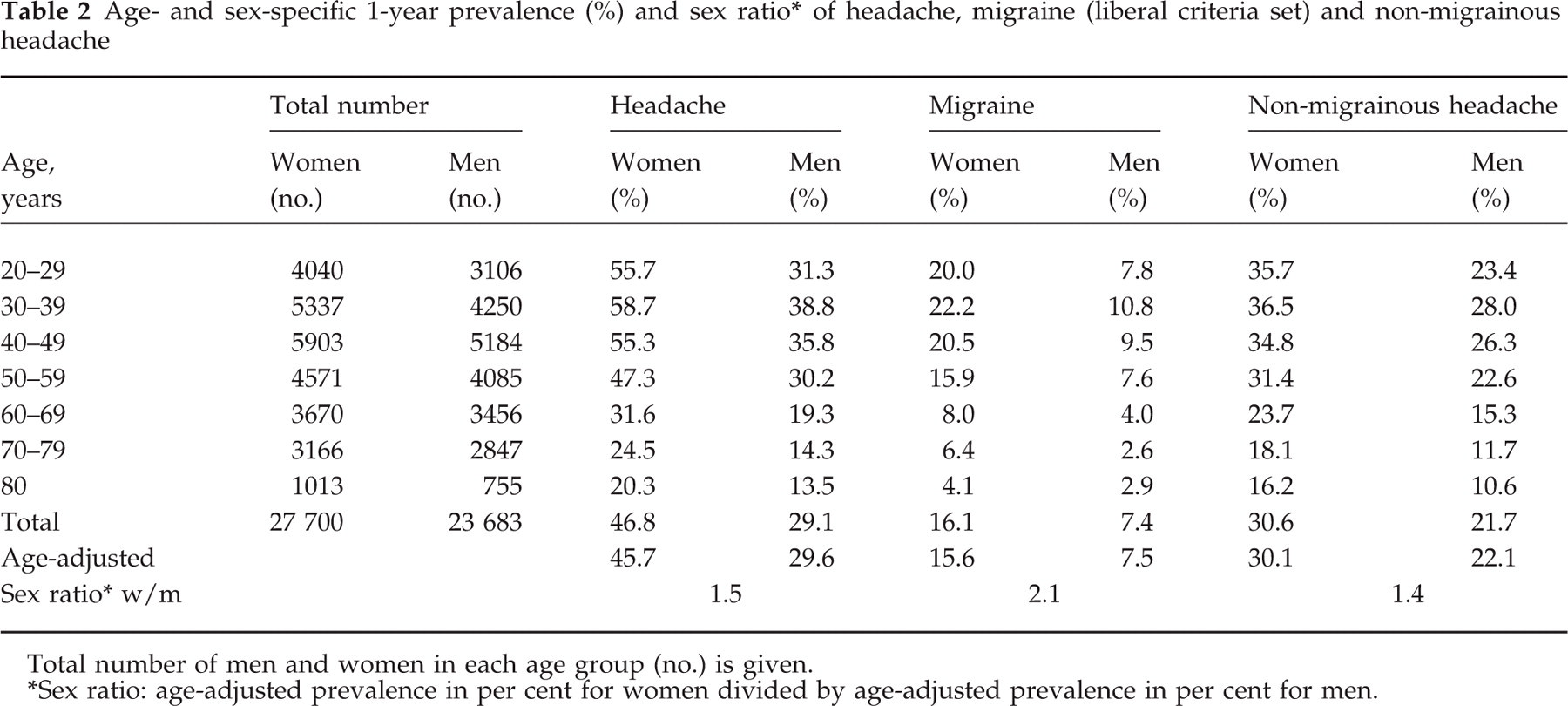
Total number of men and women in each age group (no.) is given.
Sex ratio: age-adjusted prevalence in per cent for women divided by age-adjusted prevalence in per cent for men.
The prevalence of migraine (Fig. 2) and non-migrainous headache was higher among women than in men for all age groups, with a peak between 30 and 39 years, and was lowest among those 80 years and older (Table 2).
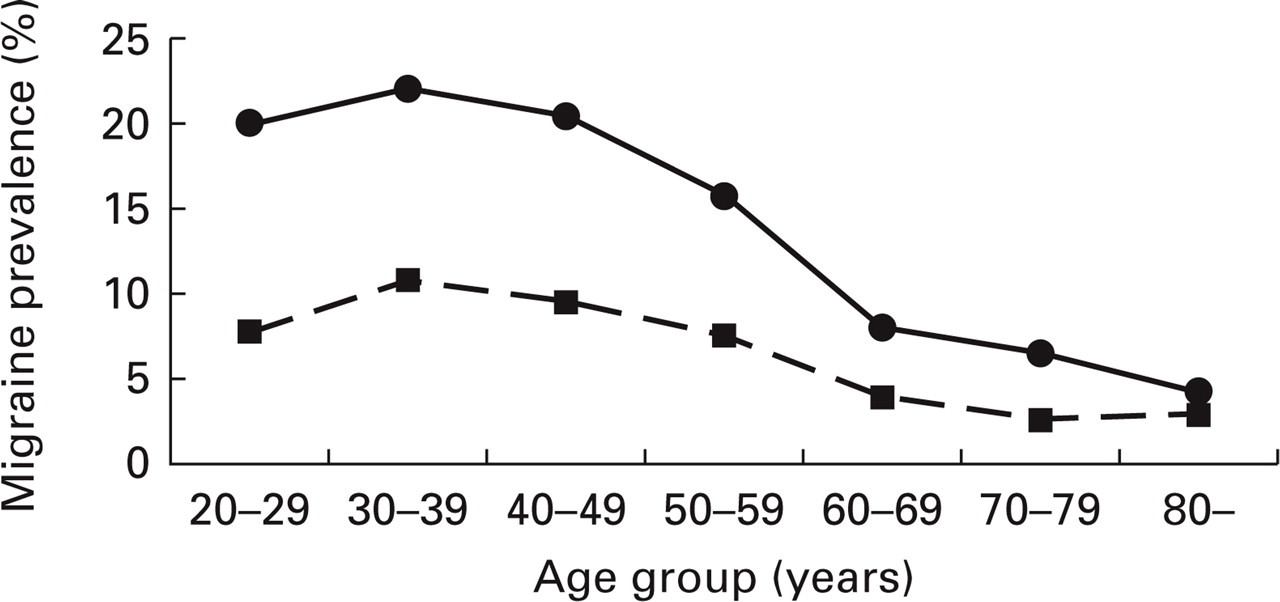
Gender- and age-specific prevalence of migraine (liberal criteria set). •, Women; ▪, men.
The age-adjusted prevalence of frequent headache (> 6 days per month) was 9.6% in women and 5.2% in men (Table 3). A total of 1189 headache sufferers (2.4%) reported headache > 14 days per month in the past year (Table 3). Approximately one-third of those suffering from frequent or chronic headache also fulfilled the liberal criteria for migraine. Using proposed diagnostic criteria for chronic daily headache (CDH) (8), we found an even lower prevalence of 1.5%.
Age- and sex-specific 1-year prevalence (%) and sex ratio∗ of frequent headache (> 6 headache days/month), and chronic headache (> 14 headache days/month)

Total number of men and women in each age group (no.) is given.
Sex ratio: age-adjusted prevalence in percent for women divided by age-adjusted prevalence in per cent for men.
A total of 1424 headache sufferers (916 women and 508 men) did not report headache frequency.
The women-to-men ratio was higher for migraine than for non-migrainous headache (2.1 vs. 1.4). The sex ratio for migraine peaked in the age groups 20–29 (2.6) and 70–79 (2.5). The women-to-men ratio for non-migrainous headache was nearly identical in all age groups.
Headache was less prevalent among individuals older than 60 years, but in contrast to the other headache categories, the prevalence of frequent non-migrainous headache was nearly constant across age groups (Fig. 3).

Prevalence (%) of non-migrainous headache and frequent non-migrainous headache (> 6 headache days/month) by age groups. ○, Non-migrainous headache, women; ▪, non-migrainous headache, men; Δ, frequent non-migrainous headache, women; •, frequent non-migrainous headache, men.
Non-participants
More women (60%) than men (51%) participated in head-HUNT. Non-participation was highest among those ≥ 80 years old (32% participated). Among ‘complete non-participants’ (28 006 subjects), approximately 1000 subjects had died or moved out of the county before screening. Apart from that, this group was younger (mean age 45.3 years) than the participants (mean age 49.1 years), whereas the ‘partial non-participants’ were slightly older (mean age 50.7 years) (P < 0.0001). Judged by the general health questions, a higher proportion of participants reported good or very good health compared with ‘partial non-participants’ (72.8% vs. 67.6%, P < 0.0001). However, more specific questions about pain in the neck, shoulder, or back, revealed no significant differences between participants and ‘partial non-participants’.
Discussion
In the present study, the overall age-adjusted 1-year prevalence of headache sufferers was 38%. A review of the literature shows that the prevalence differs widely, from < 0% to > 90% (9). Some of this variation may be attributed to different phrasing of the headache question. By using an unrestricted phrase such as ‘have you had a headache?’, very high prevalence may be found. In Finland, this question yielded a 1-year prevalence of 77%, and in Denmark, lifetime prevalence of headache was > 90% (10, 11). In the present study, we asked ‘Have you suffered from headache during the last 12 months?’ and the prevalence came out between the 29% found in Greece (12) and the 41% found in San Marino (13), and both the latter studies used a phrasing very similar to ours. In addition, headache may be perceived differently between cultures, and this may influence the response to a headache questionnaire. For example, in a recent Japanese study, 36% of the subjects defined themselves as headache sufferers, but only 46% of migraine sufferers considered themselves as ‘headache sufferers’ (14).
Migraine
Our prevalence estimate of 12% was similar to findings in population-based studies in other western countries using the IHS criteria, such as Denmark (10%), France (12%), the USA (12%), and Canada (15%) (11, 15–17). In other cultures, such as Japan, Hong Kong and Chile, the estimates have been lower: 8%, 1%, and 7%, respectively (14, 18, 19). Stewart et al. reported that migraine in Asian–Americans was about half as prevalent as in Caucasians (20). The differences in migraine prevalence have been attributed to cultural, genetic, dietary, climatic, and methodological factors (20). One potential limitation of our study is the fact that we had used a somewhat modified version of the IHS criteria, since the liberal set of criteria (Table 1) included self-reported migraine. However, by using these liberal criteria we found good agreement between the questionnaire-based migraine diagnosis and the diagnosis made by clinical interview (8). Thus, we therefore preferred these criteria to estimate the 1-year prevalence of migraine.
By using the medium restrictive criteria for migraine, the prevalence was 6.7%. This is slightly below that reported in France (8.1%), using migraine criteria ‘strictly corresponding to IHS criteria’ (15). However, as demonstrated by Henry et al. (15), differences in the diagnostic criteria may explain much of the variation between different studies. Thus, by including ‘borderline’ migraine, the prevalence in France was 12.1%, and ‘definite and possible migraine’ grouped together had a prevalence of 22.6% (15). In addition, differences in age range and methodology (questionnaire, telephone interview and/or clinical interview) also explain variations in migraine prevalence (9).
In the present study, the prevalence of migraine in the 30–69 years age group was twice as high in women as in men. In contrast, the sex ratio in the American migraine study was higher (average 2.8), reaching a maximum between 39 and 43 years (3.3), and declining thereafter (16).
Non-migrainous headaches
For non-migrainous headache, we found a women-to-men ratio of approximately 1.4, which is higher than in San Marino (1.08) and slightly higher than in Denmark (1.28) (11, 13). Tension-type headache is probably the most frequent non-migrainous headache (11). In our validation study, 80% of non-migraineurs diagnosed with the Q2 suffered from tension-type headache (8). The questionnaire-based diagnosis of tension-type headache, however, corresponded poorly with the neurologist's diagnosis, and the prevalence estimate of tension-type headache should be evaluated with caution. Even if all subjects with non-migrainous headache suffered from the tension-type, the 1-year prevalence of 26% would be lower than the prevalence reported from the USA (41%) (21), and much lower than that reported in Denmark (75%) (11). The discrepancy may, at least partly, be due to different phrasing of the question on occurrence of headache. More subjects ‘have had a headache’ (Denmark) than ‘suffered from headache’ (present study).
Frequent headache
Few epidemiological studies have estimated the prevalence of headache occurring more than 6 days per month. For those who were 70 years and older, we found a prevalence of frequent headache of 5.9% in women and 4.3% in men. In a study from the USA, 11.3% women and 5.4% men in the age group 70 years and older answered ‘yes’ to the question ‘Do you have frequent headaches?’ (22). In our study, the prevalence of frequent non-migrainous headache was nearly constant across age groups for both genders. Most studies of headache in western countries have shown a reduction in prevalence with advancing age. In several studies, however, chronic tension-type headache has been reported to be more prevalent in older age groups (21, 23). In the present study, we found that many old individuals suffered from frequent non-migrainous headache. The reason is unclear, but in a future longitudinal follow-up study we may be able to clarify whether these old individuals have suffered from headache for many years, or whether they have developed headache recently.
The age-adjusted 1-year prevalence of chronic headache (> 14 days/month) in our study (2.3%) was lower than that reported from the USA (4.1%), Spain (4.7%), and among Chinese elderly (3.9%) (24–26). The Spanish study (25) used the diagnostic criteria of chronic daily headache (CDH) proposed by Silberstein et al. (7) (headache > 15 days/month and > 4 h/day), and by using these criteria we found an even lower prevalence of 1.5%. Our rather low prevalence may reflect that many headache patients did not define themselves as ‘sufferers’. More speculatively, the lower prevalence of chronic headache in Norway may, at least in part, be explained by less overuse of medication, since many patients with chronic headache appear to use analgesics or ergots to a high degree (27).
Can the results be generalized?
Since our estimates were based on data from 56% of the total adult population in Nord-Trøndelag, one may question to what degree the results can be generalized. To study headache was not the primary objective of the survey, and selective participation due to headache status seems unlikely. Further, the prevalence of pain in the neck, shoulder, and back did not differ between participants and those who only answered Q1 (partial non-responders). Previously, a high correlation has been found between headache and neck or shoulder pain (28). We may therefore assume that the results are fairly representative of all participants in the initial survey (Q1).
Whether the results also apply to those who did not respond to the invitation (‘complete non-participants’) is less certain. In the first Nord-Trøndelag Health Survey in 1984–86, non-participation was investigated in detail (29). In general, morbidity was higher among elderly non-participants than in participants, whereas it was similar in the younger age groups. In the present study, participation was lowest among those > 80 years old. Particular selection by health status is more likely among the elderly, and generalization of results should therefore be done with caution in this group.
In conclusion, we found that nearly four in 10 individuals in Nord-Trøndelag County had suffered from headache during the last year, and more than one in 10 had suffered from migraine. Headache was more frequent among women in all age groups, and the prevalence peaked in the fourth decade of life. The prevalence of frequent non-migrainous headache was remarkably stable across all age groups.
Footnotes
Acknowledgements
This study was partially financed by a research fellowship to K.H. from the Norwegian Research Council, and partly by Glaxo-Wellcome, Norway.