
Abstract
Earlier reports regarding secular trends of migraine are conflicting, and there is a lack of long-term follow-up studies of other headache syndromes among adults. The aim of the present study was to assess any changes in the prevalence of the major headache types in a large adult population. With an 11-year interval, all inhabitants aged ≥20 years (n = 92,566 and 94,194) in the Norwegian county of Nord-Trøndelag were invited to participate in two cross-sectional surveys. Attendance rates were 56% and 42%. The age-adjusted 1-year prevalences, according to the diagnostic criteria of the International Headache Society, sex-ratios and attack frequencies were assessed. The migraine prevalence increased from 12.1% to 13.2% (P < 0.001), but the sex ratio did not change. The prevalence of non-migrainous headache overall decreased (26.0% vs 24.2%; P < 0.001). The prevalences of ‘headache suffering’ (37.4%), chronic daily headache (2.5%) and medication overuse headache (1.0%) remained stable. Apart from a small increase of migraine, headache prevalences remained essentially stable among adults in a Norwegian county during an 11-year period.
Introduction
Headache disorders constitute the largest cluster of neurological diseases, thus causing wide-spread suffering and large costs for society (1,2). Those with disabling migraine or chronic daily headache (CDH) are in need of good healthcare (3). In order to estimate service requirements, it is exceptionally important to monitor any changes in the prevalence of the most common headache disorders.
The general view is that the occurrence of migraine remains stable, but the data are somewhat conflicting. All studies in children and adolescents indicate an increase (4–7). Among adults in the US, there have been reports of an augmentation both in the prevalence of self-reported migraine (8) and in the incidence of medically recognised migraine (9,10). This could, however, not be confirmed in the form of a true prevalence increase in a population-based follow-up study applying strict diagnostic criteria (11). During a 6-year period, a marked increase in the prevalence of migraine was found among Hong Kong Chinese aged 15 years or older (7). In follow-up studies of adults during a 10-year period in France and young adults during a 12-year period in Glostrup in Denmark, the migraine prevalence remained stable (12,13), although in the latter case, there was a significant increase in the proportion of subjects with frequent migraine. Taken together, these reports raised questions that needed to be studied further.
Only three studies have analysed long-term changes in other headaches than migraine, mainly among children and young adults (5,7,13). There is thus a gap in the knowledge concerning secular trends of all headaches combined among adults. Furthermore, there are no data available with regard to long-term changes in the prevalence of CDH or medication overuse headache (MOH), both of them being important burdens for society.
The present survey is a replicate of the ‘head-HUNT’ study, a large cross-sectional survey performed in 1995–1997 where all inhabitants in a single county in Norway were invited to participate (14). We have explored the prevalences and frequencies by age and gender of all the major headache syndromes according to case definitions based on the International Headache Society (IHS) criteria (15,16) and determined any changes over an 11-year period.
Materials and methods
Study populations
Nord-Trøndelag is one of 19 Norwegian counties, and is located in the middle part of the country. The population is scattered but ethnically quite homogeneous and consists mainly of Caucasians. The Nord-Trøndelag Health Survey (‘Helseundersøkelsen i Nord-Trøndelag’; HUNT) is a longitudinal cohort study inviting all adult inhabitants of the area to participate. Since 1995, the HUNT survey includes a section on headache disorders, the ‘head-HUNT’ questionnaire (17). This is a report of the second ‘head-HUNT’ survey, comparing it to the first one performed 11 years earlier.
The first head-HUNT study sample (HUNT 2)
Between 1995 and 1997, all inhabitants ≥20 years old in Nord-Trøndelag were invited to participate in HUNT 2, the second cross-sectional analysis of HUNT. Out of 92,566 invited individuals, 64,560 (70%) answered the first questionnaire (Q1) that was enclosed with the invitation letter, and participated in a brief medical examination, at which they were given a second questionnaire (Q2) to be filled in and returned from home. The two questionnaires included more than 200 health-related items, and the Q2 included 13 headache questions, mainly designed to determine whether the person suffered from headache or not, and whether he or she fulfilled the migraine criteria of the International Headache Society (IHS) (15). The screening question was ‘Have you suffered from headache during the last year?’, and only individuals who answered ‘yes’ were asked to fill in the other headache questions. A total of 51,383 subjects (56% of the invited) answered the screening question and completed the headache questionnaire in Q2, and these constituted the first ‘head-HUNT’ study sample. Among participants, the mean age was 49.9 years, 53.9% were women, 76.8% were working, and 28.0% daily smokers. Details regarding non-participants were described previously (14).
The second head-HUNT study sample (HUNT 3)
The third Nord-Trøndelag Health Study (HUNT 3) is a replication of HUNT 2. All inhabitants aged 13 years or more in Nord-Trøndelag were invited to participate in the third Nord-Trøndelag Health Survey between October 2006 and June 2008. The Q2 included a total of 14 headache questions that were designed to determine whether the person suffered from headache, and fulfilled the ICHD-II criteria for migraine or tension-type headache (TTH) (16). The flow of adult participants (aged 20 years or more) through the study is described in Figure 1 (the young HUNT study in adolescents will be reported separately). Among the 39,690 participants in the second ‘head-HUNT’, the mean age was 54.1 years, 56.0% were women, 74.8% were working, and 17.7% daily smokers.
Flow of participants through the different steps of the HUNT 3 headache survey.
Ethics
The HUNT 2 and HUNT 3 surveys were approved by the Regional Committee for Ethics in Medical Research and the Norwegian Data Inspectorate.
Headache diagnoses
Headache sufferers were asked to report how their headaches usually were regarding pain intensity, attack duration, and accompanying symptoms. To reduce the risk of misunderstanding, all questions were made as clear and simple as possible. Regarding attack duration, the participants were not explicitly instructed to report the duration of untreated attacks, partly because some individuals always use attack medication for their headaches. In another part of the Q2, the individuals were also asked to state the consumption of analgesics and over-the-counter (OTC) drugs during the last month, allowing a tentative diagnosis of medication overuse headache (MOH).
Year 1999 diagnostic criteria
Diagnostic sets of criteria for the diagnosis of migraine based on information in the questionnaire

Year 2010 diagnostic criteria
The Q2 questionnaire in HUNT 3 included a question about pain intensity, which enables the report of definite migraine, probable migraine, and tension type headache (TTH) according to the present ICHD-II criteria (16). These diagnoses are mutually exclusive. Since it was not specifically asked for untreated headache attacks in Q2, the ICHD-II criteria for migraine are slightly modified so that also a duration of less than 4 h is accepted (Table 1). For migraine with aura, only visual disturbance is included in the criteria set. The TTH diagnosis trumps probable migraine, i.e. patients fulfilling both are classified only as TTH. Frequent headache is defined as headache occurring 1–14 days per month, and chronic daily headache (CDH) is defined as >14 days per month. Owing to an alteration of the Q2 question on medication use between HUNT 2 and HUNT 3, the definition of medication overuse used in the analysis of HUNT 3 data was ‘OTC-medication use for headache ≥4 days/week during the last month’. MOH was defined as CDH with medication overuse.
Validity and reliability of the headache diagnoses
The relative merits of the year 1999 criteria were evaluated previous to the analyses of the first ‘head-HUNT’ survey (17). The chance-corrected agreement (kappa) for headache suffering in the Q2 questionnaire of HUNT 2 was 0.57. The positive and negative predictive values for ‘liberal’ migraine were 84% and 78%, respectively, and the kappa value was 0.59. For non-migrainous headache, positive and negative predictive values were 68% and 76%, respectively, and the kappa value was 0.43. For frequent headache (headache >6 days per month), and CDH (headache >14 days per month), the kappa values were 0.50, and 0.44, respectively.
The validity of the year 2010 criteria were reported recently (18). For the questionnaire-based status as headache sufferer, a sensitivity of 88%, a specificity of 86%, and a kappa value of 0.70 were found for the Q2 questionnaire of HUNT 3. A sensitivity of 51%, a specificity of 95%, and a kappa value of 0.50 were found for ‘restrictive’ migraine. Asking whether individuals had suffered from headache during the last year yielded high positive predictive value and high specificity for identifying individuals with ‘restrictive’ migraine ≥1 day/month (19). Therefore, the validity of ‘restrictive’ migraine and TTH ≥1 day/month was investigated. A sensitivity of 58% (migraine) and 96% (TTH), a specificity of 91% and 69%, and kappa values of 0.54 and 0.44 were then found, respectively. The specificity for migraine with aura was 95%. CDH, chronic TTH, and MOH were diagnosed with a specificity of ≥99%, and kappa values of ≥0.73 (18). The ‘liberal’ migraine criteria were also evaluated in the present HUNT 3 population. A sensitivity of 49%, a specificity of 96%, and a kappa value of 0.51 were found (18).
Statistical analysis
For the various headache categories, prevalences in men and women were estimated separately by age decade. The overall prevalence was age-adjusted, using the age distributions of all inhabitants aged ≥20 years in Nord-Trøndelag County in 1995 (HUNT 2) and 2006 (HUNT 3) as the standard populations. The sex ratio for each headache category was calculated using the age-adjusted prevalence for women divided by the age-adjusted prevalence for men.
The ‘head-HUNT’ samples were partly overlapping (one half of participants, n = 26,060, in the first survey also participated in the second). Prevalences in the two surveys were, therefore, compared using a two-step strategy. First, adjusted prevalences in the two surveys were compared with the chi-squared test. If significant differences (P < 0.05) were found, the adjusted prevalences were compared in a second step by using a logistic mixed effects model with patient-ID as random effect and HUNT-number (i.e. HUNT 2 or HUNT 3) and age-category as fixed effects. Consistently, this confirmed the results from the first step. For the comparison of participants and non-participants, the independent samples t-test was chosen for continuous (age) and the chi-squared test for categorical variables. Two-tailed estimations of significance were used, and the level of significance was set at P < 0.05.
Data analysis was performed with the Predictive Analytics SoftWare (PASW) Statistics v17.0 by SPSS Inc., an IBM Company (Chicago, IL, USA).
Results
All headaches combined
As demonstrated by Table 2A,2B, there were no significant differences between HUNT 2 and HUNT 3 regarding the prevalence of all headaches combined (37.7% vs 37.4%; P = 0.36) or the prevalence of CDH (2.4% vs 2.5%; P = 0.33). The prevalence of CDH was higher among women than in men for all age groups, with a peak between 30 and 39 years, and was lowest among those 70–79 years old (Figure 2C).
(A) One-year prevalence (%) of ‘restrictive’ migraine by age categories in HUNT 3. (B) One-year prevalence (%) of TTH by age categories in HUNT 3. (C) One-year prevalence (%) of CDH by age categories in HUNT 3. Headache suffering, self-considered migraine, ‘liberal’ migraine and non-migrainous headache in HUNT 2 and HUNT 3 according to the year 1999 criteria Prevalences and sex-ratios are adjusted. *Frequent headache is defined as headache occurring >6 days per month.

Migraine
HUNT 2 versus HUNT 3
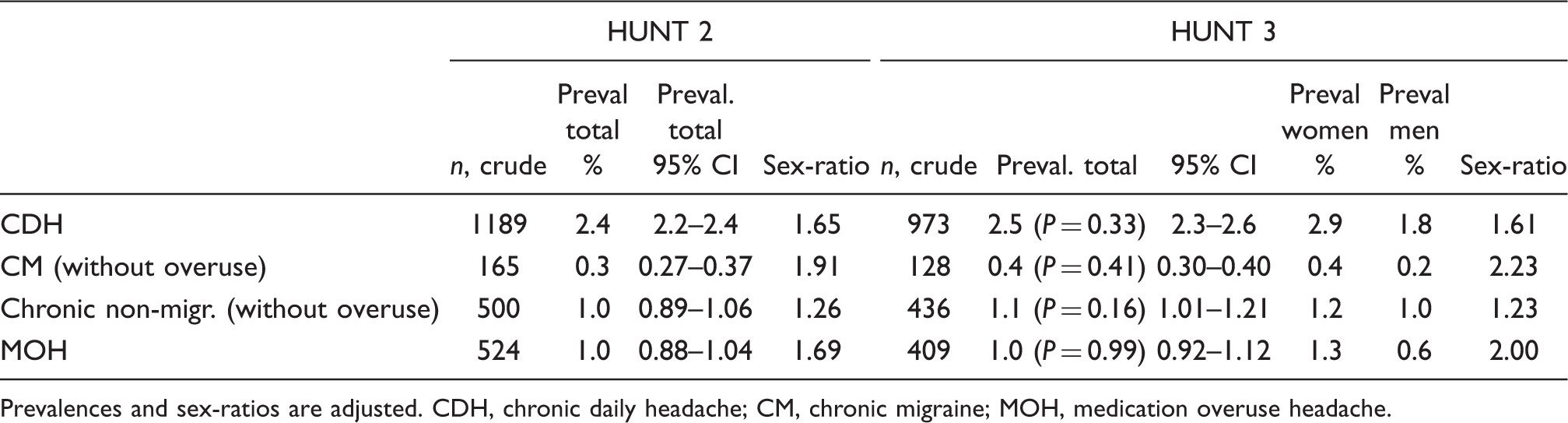
No significant difference was found regarding self-considered migraine between HUNT 2 and HUNT 3 (8.3% vs 8.0%; P = 0.10; Table 2A). However, when applying the ‘liberal’ migraine criteria, a higher prevalence was found in HUNT 3 than in HUNT 2 (13.2% vs 12.1%; P < 0.001). In HUNT 3, 3.9% women and 1.5% men (adjusted total 3.1%) had migraine occurring >6 days per month, and a total of 0.4% had chronic migraine (CM; Table 2B) according to the year 1999 criteria, which were not significantly different from HUNT 2 (P = 0.08 and P = 0.41, respectively).
HUNT 3
The age-adjusted prevalence of ‘restrictive’ migraine in HUNT 3 was 12.0% (Table 2A). Out of these, the majority had migraine occurring 1–14 days per month, and the most common frequency was 1–6 days per month (Figure 3). The prevalence of ‘restrictive’ migraine was higher among women than in men for all age groups, with a peak between 30–39 years, and was lowest among those 80 years and older (Figure 2A). The sex ratio (total 1.4) peaked in the age group 30–39 years and among those with an attack frequency of 1–6 days per month (Figure 3). As demonstrated by Table 3, the adjusted 1-year prevalence was 5.8% for migraine with aura, 5.9% for probable migraine, and 0.5% for CM according to the year 2010 criteria. The women to men ratio of CM was 2.4 (Table 3 and Figure 3). Among those with self-considered migraine, 31% (n = 945) also considered themselves to have non-migrainous headaches.
Adjusted prevalences for ‘restrictive’ migraine and TTH separated upon four categories of headache frequency. Participants with medication overuse excluded. Chronic headache in HUNT 2 and HUNT 3 according to the year 1999 criteria Prevalences and sex-ratios are adjusted. CDH, chronic daily headache; CM, chronic migraine; MOH, medication overuse headache. Prevalences of headache in HUNT 3 according to the year 2010 criteria Prevalences and sex-ratios are adjusted. Comparison between participants (Part) and partial non-participants (PnP)


TTH and other non-migrainous headache
HUNT 2 versus HUNT 3
The age-adjusted prevalence of all non-migrainous headache in HUNT 3 was 24.2%, which was significantly lower (P < 0.001) compared to HUNT 2 (26.0%; Table 2A). The prevalence (4.1%; Table 2A) of non-migrainous headache occurring >6 days per month peaked between 30–39 years (4.8%), and was lowest among those 80 years and older (2.9%). A significant decrease from HUNT 2 (Table 2A) was observed for non-migrainous headache occurring >6 days per month (P < 0.001). In HUNT 3, the 1-year prevalence of chronic non-migrainous headache without medication overuse was 1.1% and did not differ significantly from HUNT 2 (Table 2B). Among those with non-migrainous headache, 65% (n = 5952) satisfied the ICHD-II criteria for TTH.
HUNT 3
The age-adjusted prevalence of TTH in HUNT 3 was 16.5% (Table 3). Out of these, most had frequent episodic TTH, and the most common frequency was 1–6 days per month (Table 3 and Figure 3). The prevalence of TTH was higher among women than in men for all age groups, with a peak between 30–39 years, and was lowest among those 80 years and older (Figure 2B). The women to men ratio for TTH was 1.1, and the sex ratio peaked in the age group 20–29 years (Figure 2B). For infrequent TTH, the women to men ratio was 0.9 (Table 3 and Figure 3). The adjusted 1-year prevalence of chronic TTH was 0.6% (Table 3 and Figure 3), and there was a reduction in the prevalence with advancing age from 0.8% in the age group 20–29 years to 0.4% among those 70 years and older.
Medication overuse headache
The age-adjusted prevalence of MOH in HUNT 3 was 1.0%, which did not differ significantly from HUNT 2 (Table 2A). The prevalence peaked among those 30–49 years (1.3%), and was lowest among the youngest and the oldest (0.7%, 20–29 years and ≥70 years of age). MOH was more common among women than men (sex ratio 2.0) in all age groups except among those 80 years and older.
Non-participants
More women (47%) than men (37%) participated in the second ‘head-HUNT’. Participation was highest in the age group 50–79 years (55%), and lowest among those aged 20–29 years (22% participated) and those ≥80 years old (26% participated). Participants in HUNT 3 were more likely to be women (56% vs 49%; P < 0.001), had a higher mean age (54.1 vs 48.9 years; P < 0.001), and had slightly less often chronic pain lasting at least 6 months during the past year (39% vs 37%; P < 0.01) compared to the partial non-participants in HUNT 3 that had answered relevant questions in Q1 (94%; n = 10,487; Table 4). No data were available concerning the 43,355 persons who did not participate in HUNT 3 (complete non-participants). However, in the future, a non-participants study will be published.
Discussion
This is, so far, the largest replicate cross-sectional study using identical diagnostic criteria to investigate trends over time in the occurrence of migraine and other headaches. Overall, our results indicate that prevalences remain essentially stable among adults, with a small increase in the 1-year prevalence for migraine.
All headaches combined
Our findings of a 1-year prevalence of 38% for all headaches combined and 2.5% for CDH are somewhat lower than the means of earlier epidemiological studies in Europe, where current headache and CDH occurred in 53% and 4% of adults, respectively (20). This is most likely explained by the strict introductory screening question, which asks if the participant is ‘suffering’ from headache (19). Furthermore, it is well-known that those who answer ‘no’ to a screening question concerning headache may nevertheless suffer from headache, even migraine (21–23). This is illustrated by earlier studies which showed that 30–60% of the individuals who answered negatively to the direct question whether they had had headache or not, reported headache when asked to keep a headache diary (19,23). In the present survey, a considerable number of participants (n = 3876) who did not classify themselves as headache ‘sufferers’, nevertheless gave at least one positive answer to the headache questions. If these are counted, the 1-year prevalence of all headaches combined increases.
The proportion of schoolchildren in the city of Uppsala in Sweden who never suffered from headache was lower in 1997 than in 1955, indicating an increase in the general prevalence of headache (4). In contrast to this, we could not find a significant change during the 11 year period in the prevalence of all headaches combined among adults in Nord-Trøndelag. Nor was there a change in the prevalence of CDH.
Migraine
A stringent case definition of ‘restrictive’ migraine similar to that of the ICHD-II was employed in this study. The present criteria (Table 1) differed from the strict ICHD-II criteria in that this study did not consider the number of previous attacks experienced over the life-time, and that attacks with a duration below 4 h were included. The 1-year prevalence of ‘restrictive’ migraine (12.0%) found in the Nord-Trøndelag population was somewhat lower compared to findings from across the border in Sweden (13.2%) (24) and in other countries in Europe (mean 14.7%) (20,24). Certain factors may have led to underestimation or overestimation of migraine in this study. First, some individuals who denied headache suffering may have had migraine. A second potential source of error caused by the fact that we could only diagnose one headache type in each individual is that a diagnosis of migraine may be missed in the presence of non-migrainous headache that occurs proportionally more frequently and thereby overshadows migraine (25). This potential for misclassification is probably highest for individuals with only rare migraine attacks (26). Third, the rather low sensitivity (51%) of the HUNT 3 questionnaire for detecting ‘restrictive’ migraine may have contributed to lowering the prevalence figure. Finally, migraine-like headaches arising from organic disease could not be excluded. These cases are probably rare.
Also, the relatively low sensitivity (50%, and 95% specificity) of the questionnaire-based diagnosis of migraine with aura makes the instrument unsuitable for determining the prevalence in the population (18,26), and the finding that every second migraineur reported visual disturbances in association with their headaches should be interpreted with much caution.
Our finding of a prevalence of 5.9% for probable migraine (category 1.6 in ICHD-II (16)) was high from a clinical perspective, yet considerably lower than the 9.1% found for ‘migrainous disorder’ (category 1.7 in the 1988 version of the IHS-criteria (15)) by Henry et al. in France (12).
Pain intensity was not part of the questionnaire in the first ‘head-HUNT’. Therefore, a revised version of the IHS criteria called ‘liberal’ migraine (Table 1) were defined to estimate the 1-year prevalence (14). In the two validation studies, acceptable agreement was found between the questionnaire-based ‘liberal’ migraine diagnosis and the migraine diagnosis made by clinical interview (17,18). We have also assessed ‘liberal’ migraine in the second ‘head-HUNT’, and found a small, but significant (P < 0.001), increase from 12.1% to 13.2%. As in a clinic-based study in Italy, there was no change over time in the sex ratio (27).
It must be taken into account, that the rather low sensitivity (49%) of the second ‘head-HUNT’ questionnaire for detecting ‘liberal’ migraine negatively affects the comparability between the two head-HUNT surveys. Two questions regarding migrainous symptoms were slightly revised between HUNT 2 and HUNT 3 to harmonise with ICHD-II (16). In HUNT 3, participants were not only asked for ‘nausea’, but for ‘nausea and/or vomiting’. Furthermore, aura was not only asked for ‘before’ the headache, but ‘before or during’. These somewhat broader definitions could increase the number of patients fulfilling the ‘liberal’ migraine criteria. According to clinical experience, however, patients seldom have vomiting without nausea, and seldom aura during but not before headache. The net influence of these factors is, therefore, likely to be small and unlikely to have influenced the conclusion.
The present finding of increasing migraine prevalence is in agreement with all replicate studies in children and adolescents (4–7), but not in adults (11–13). An exception is the Hong Kong study including participants aged 15 years and above (7), where the prevalence increased more than 4-fold. Notably, owing to significant changes in the methodology, the second survey was not a strict replicate which hinders the possibility to draw firm scientific conclusions as to a secular trend within this Chinese city population.
Self-assessed migraine is part of the ‘liberal’ migraine criteria. One could, therefore, ask if the increase in prevalence of ‘liberal’ migraine is driven by an increased disease awareness among migraineurs in Nord-Trøndelag during the 11 years between the surveys. Such a problem has been noted in the US, where an increase in self-reported migraine (9,10) could not be confirmed by Lipton et al. (11) in the form of a true increase in the prevalence of strictly diagnosed migraine. However, this phenomenon is probably not important in our study, since the prevalence of self-considered migraine (8.0%) had not changed, and was still low compared to both Sweden and the US (28,29).
The prevalence of ‘liberal’ migraine occurring >6 days per month did not increase significantly. We could, therefore, not confirm the earlier finding by Lyngberg et al. (13) of an amplified migraine frequency among adults in Denmark. In line with a stable prevalence of frequent migraine, which is a risk factor for transition to CM (30), the prevalence of CM (0.5% according to ICHD-II criteria) had not changed since the first ‘head-HUNT’ study. The women to men ratio of 2.4 found for CM according to the year 2010 criteria is the highest sex ratio among all studied diagnoses in the present study.
A plausible explanation for the increase in migraine prevalence, if the finding is true, is the occurrence of changes in society influencing the exposure to risk factors. During the 11-year follow-up period, several types of changes in the physical and social environments have been introduced, for example, an escalated use of computers and mobile phones, in particular among the young and middle-aged. Whether such changes could be directly linked to migraine or indirectly due to increases in stress (31), sedentary life (32) or other unfavourable life-style (33) are still unclear. Another factor may be the rise in mean weight that has recently been documented in Nord-Trøndelag (34). The frequency and severity of migraine attacks have been found to increase with body mass index (35). However, weight gain is not proven to cause new-onset migraine, which would affect the prevalence. Among other potential contributing factors may be an increase in psychiatric morbidity (36), which remains to be investigated in Nord-Trøndelag.
TTH and other non-migrainous headache
One in four persons (24%) were classified as having non-migrainous headache. As is common in questionnaire studies (22), the participants were asked to give answers based on the overall most distressing headache, whereby potential problems with ‘double-counting’ were avoided (26). The shortcoming is that we can only differentiate between those who suffer mostly from migraine and those who suffer mostly from non-migrainous headache, since migraine is hierarchically more important in the IHS diagnostic system (15,16,22). In Denmark, the majority of migraineurs also had other headache (13,37). In the present population, almost one-third (31%) of those with self-considered migraine considered themselves to also have non-migrainous headaches.
TTH is the dominating non-migrainous headache (37), which was earlier confirmed in HUNT 2 (17). In the present analysis of HUNT 3, two-thirds of those with non-migrainous headache satisfied the ICHD-II criteria for TTH. Prevalence estimates for TTH vary largely between 16% and 87% (13,20). Our finding of 16.5% is thus in the low range. The wide disparity in prevalences for TTH might be due to different capture of subjects with infrequent TTH. The prevalence of infrequent TTH was only 4.5%. We may assume that this is an underestimation, mostly because the screening question ‘Have you suffered from headache during the last 12 months’ used in several population-based studies gives a much lower headache prevalence than a more neutral question (19). For infrequent TTH, the women to men ratio of 0.9 was the lowest sex ratio among all studied diagnoses. In previous studies, the prevalence of chronic TTH has been 1–3% (7,20,37), which is higher than the present study (0.6%).
Lyngberg et al. (13) found an increase in both the prevalence and attack frequency of TTH in Denmark. The narrow age-range (25–36 years) did not allow a safe estimation of the prevalence rate across all age-groups among adults. In Hong Kong, the prevalence of TTH among persons above 15 years of age was reported to increase dramatically from 2% to 27% during a 6-year period (7). However, methodological limitations probably account for an underestimation of prevalence in the initial Chinese survey. Our results point in the opposite direction. There was a small, but significant (P < 0.001), decrease both in the prevalence of non-migrainous headache altogether and in the prevalence of non-migrainous headache with high frequency. But since the diagnoses of migraine and non-migrainous headache were mutually exclusive, an increase in migraine automatically contributes to a decrease in other headache. All in all, we doubt there is a lower occurrence of TTH now than 11 years ago. Chronic non-migrainous headache had remained unchanged, and since TTH is still the most prevalent headache, the societal and individual burden associated with this primary headache is substantial (2,38).
Medication overuse headache
It is recommended that the MOH diagnosis should be given to patients if they have a primary headache plus on-going medication overuse (39). According to this, the 1-year prevalence of MOH is 1% in Nord-Trøndelag in both HUNT 2 and HUNT 3. This is in agreement with other European studies, where the prevalence of current MOH among adults has been 1–2% (20,40,41). In HUNT 3, we found a marked age dependency (almost twice as prevalent among those 30–49 years). This contrasts to HUNT 2 where the prevalence of MOH was nearly constant across the age groups (2,41,42). To our knowledge, this is the first time that the prevalence of MOH has been assessed repeatedly in a population-based longitudinal study. The lack of an increase in the 1-year prevalence during an 11-year period was a bit surprising from a clinical perspective. During this period, there has been a liberalisation of the sale of OTC analgesics, which from 2004 can be bought in grocery stores, petrol stations, etc. The definition of medication overuse is different in the two studies, and the comparability for MOH between the surveys is, therefore, limited. In the year 1999, diagnostic criteria medication overuse refers to a time period of 12 months, while in the year 2010 diagnostic criteria participants are asked to report their medication overuse within the last month. The question on medications was part of Q2 but not of the ‘head-HUNT’ questionnaire. Beyond our control, it was changed between HUNT 2 and HUNT 3 (see Methods). It must be pointed out that triptans are not sold OTC in Norway. Hence, specific triptan-overuse headache is not captured in HUNT 2 or HUNT 3.
General methodological considerations
The strengths of this study were the exact replication of design and methodology, the large and unselected populations, the wide age-range, the long follow-up period (11 years), and the use of validated definitions for all common headache syndromes. The fact that the precision of the headache diagnoses in HUNT 3 were as good as that in HUNT 2 enabled a comparison of the results between the two studies (18).
When interpreting the results of the study, some overall limitations must be taken into account. First, the questionnaire diagnoses were not optimal compared with the interview diagnoses (17,18). The main drawback of HUNT 3 was the relatively low participation rate of 42%. A differential participation rate depending on the occurrence of headaches can result in an overestimation of the prevalence rates. However, the fact that the ‘head-HUNT’ questionnaires were not the primary objectives of the HUNT 2 or HUNT 3 makes selective participation due to headache less likely. The majority (80%) of refusals were made by ‘complete non-participants’ for whom the presence of a headache questionnaire was not known. Since the overall prevalence of headache and self-reported migraine had not changed among participants in the two ‘head-HUNT’ surveys, it is expected that any non-participation effect would apply equally to both our cross-sectional cohorts and thus not interfere with the comparisons over time. In both HUNT 2 (43) and HUNT 3, non-attendance was lower among men and among the elderly. Although we standardised the prevalence data to match the age distribution for men and women in the general population, generalization of our results to non-participants should be done with special caution in these groups. Furthermore, in HUNT 3, the prevalence of chronic pain was slightly higher among participants than among ‘partial non-responders’. All in all, we may assume that the ‘head-HUNT’ results are fairly representative of the adult population in Nord-Trøndelag.
Conclusions
The main finding was stability over time in the prevalence of all headaches combined. There was a slight increase in the migraine prevalence, a result that should be followed-up in future studies.