
Abstract
To estimate the lifetime migraine prevalence in school adolescents aged 13–15 in Taiwan, we conducted a self‐administered questionnaire survey in four sampled public junior high schools. Migraine was diagnosed according to the diagnostic criteria of the International Headache Society. A total of 4064 students (1983 boys, 2081 girls) completed the questionnaire (response rate 91.6%). The lifetime prevalence of migraine was 6.8%. It was significantly higher in girls than boys (7.8% vs. 5.7%) and increased with age in both sexes. Students with migraine were more likely to be absent from school because of their headaches than those with non‐migraine headaches (30% vs. 14%, odds ratio (OR) 2.7). They were also more likely to use painkillers for their headaches than their non‐migraine headache peers (72% vs. 40%, OR 4.0). These results suggest that migraine is a common disorder of adolescents in Taiwan and its impact on the quality of life can not be ignored.
Introduction
Migraine in adolescents is not uncommon. Studies in Europe and the USA have reported prevalences of migraine in adolescents ranged from 2.7% to 22% (1–4). This wide range of reported prevalence of migraine may be the result of differences in study methodology, diagnostic criteria, and populations (5).
The diagnostic criteria for migraine defined by the International Headache Society (IHS) in 1988 have been widely accepted and provide a standardized tool for epidemiological studies of migraine (6). The only difference between the adult and adolescent (< 15 years) criteria for migraine is the duration of headache, with a 4–72‐h duration required for the adult and a 2–48‐h duration required for the adolescent (6). The application of IHS migraine criteria makes comparisons between different cultures possible.
Previous studies conducted in the People's Republic of China found a very low prevalence of migraine (7). In contrast, our recent study showed that the migraine prevalence in a Chinese elderly population in Kinmen, Taiwan, was much higher (8).
Migraine is responsible for a significantly reduced school attendance in adolescents in Western societies (9, 10). In addition, Chambers et al. reported that self‐administration of medications in adolescents usually started as early as age 11 years, including over‐the‐counter painkillers for headache (11). Therefore, migraine is an important health issue in this age group.
To understand migraine prevalence and its impact in Chinese adolescents in Taiwan, we conducted a survey of migraine headache among students aged 13–15 years using a population‐based sample.
Subjects and methods
A population‐based questionnaire interview was conducted among public school students aged 13–15 years from four different public schools during the period September 1998 to May 1999.
Sampling
The study subjects were a convenience sample of public junior high school students. In Taiwan, education is obligatory from age 6–15 years. More than 90% of teenagers aged 13–15 attend public junior high schools (grade 1 to grade 3, similar to grade 7–9 in the USA) and the remaining teenagers attend private schools. A total of four junior high schools were randomly chosen, with one each in the northern, central, southern and eastern region of Taiwan (Fig. 1). All of the students in these four schools were our targeted population (n = 4436), which was equal to 0.5% of the adolescents aged 13–15 years in Taiwan.

Map of Taiwan, showing the four regions included in the study.
Questionnaire design
A self‐administered questionnaire was used which consisted of 25 items including basic demographic data (n = 5); lifetime headache profiles including four aura manifestations, i.e. visual, motor, sensory and speech symptoms (n = 12); the frequency of pain‐killer use (n = 2); school absence due to headache in the past semester (categorized as follows: 0, 1–3, 4–7, 8–14, 15–28, > 28 days) (n = 1); ice cream headache (n = 1); recurrent abdominal pain (n = 1); cola drinking habit (n = 1); and menstruation in girls (n = 2). The items of headache profiles were designed based on the IHS diagnostic criteria. To make a diagnosis of migraine, the headache features had to fulfil all of the IHS diagnostic criteria from B to D for migraine (IHS code 1.1), except that criterion A, i.e. ‘at least five attacks’ was not mandatory in this study (12). ‘Non‐migraine headache’ was diagnosed if headaches did not fulfil the above modified criteria. Subjects who had both migraine and non‐migraine headaches were classified as migraineurs.
Validity of questionnaire‐diagnosed migraine
The clinical validity of the questionnaire‐diagnosed migraine was determined within 4 weeks after questionnaire administration. A total of 217 students with headaches were selected from the initial survey of the study. The students with moderate or severe headaches were over‐sampled. Three neurologists, who were blind to the questionnaire results, interviewed these students with a semi‐structured questionnaire and reached a headache diagnosis at a consensus meeting according to the modified IHS criteria described above.
Survey procedures
Letters describing our study objectives and methodology were first mailed to the school principals of the sampled schools for their approval. A self‐administered questionnaire was answered by all the students in these sampled schools. Data from completed headache questionnaires were analysed by computer algorithm.
Statistical analysis
The prevalence of migraine was reported as the number of cases per 100 persons with 95% confidence intervals (CI). Age‐ and sex‐specific prevalence were also calculated. The validity of the headache questionnaire was assessed by observed agreement rate, chance corrected agreement rate (κ statistics), sensitivity and specificity. Student's t‐test and χ2 test were used for comparison when appropriate. χ2 test for trend analysis was used to analyse the trend among different age groups. P < 0.05 was considered statistically significant.
Results
Our target population consisted of 4436 students (2216 boys, 2220 girls) in four public junior high schools. A total of 4239 questionnaires (2096 boys, 2143 girls) were returned with a response rate of 95.6% (Table 1); of them, 175 questionnaires were excluded because four or more items were missing. This exclusion resulted in a final sample of 4064 (91.6%) (1983 boys, 2081 girls) completed questionnaires for analysis. A significantly lower participation rate was found in boys (89.5% in boys vs. 93.7% in girls, P < 0.0001) and in second grade students (aged 14) (90.1% at age 14 vs. 93.1% at age 13 and 91.7% at age 15; P = 0.02).
The numbers of participants in the four public junior high schools

Validity of questionnaire
Of the 217 students selected for validity study, 201 (93%) finished the clinical interview. The comparisons of the migraine diagnoses made by the questionnaire and the neurologist showed the observed agreement rate was 78.6% and κ statistics 0.51. Using doctors' diagnosis as the ‘gold standard’, the sensitivity of the headache questionnaire for migraine diagnosis was 74.1% and specificity 80.4% (Table 2). However, the sensitivity of the four reported aura symptoms ranged from 0 to 33.3%, the specificity from 86.3% to 97.4%, and the κ value ranged from −0.05 to 0.35. Visual aura had the highest sensitivity (33.3%) and specificity (97.4%), whereas sensory aura had the lowest. Due to this unsatisfactory validity, only the results of visual aura are presented in this study.
The sensitivity and specificity of the questionnaire

Sensitivity = 43/58 (74.1%).
Specificity = 115/143 (80.4%).
Prevalence of self‐reported headache
Overall, 3440 of the participants (84.6%) reported they had had at least one headache in their lifetime. Table 3 shows the age‐, sex‐, and regional‐specific prevalence of self‐reported headache. The prevalence increased with age (χ2 for linear trend = 7.4, d.f. = 2, P = 0.02) in both sexes. Girls (87.9%) had a significantly higher prevalence than boys (81.3%) (χ2 = 34.4, d.f. = 1, P < 0.0001). A significantly higher prevalence (88.2%) was noted in the Yu‐Li Junior High School (Table 3).
The age‐, sex‐, and regional‐specific prevalence (%) of headache and migraine
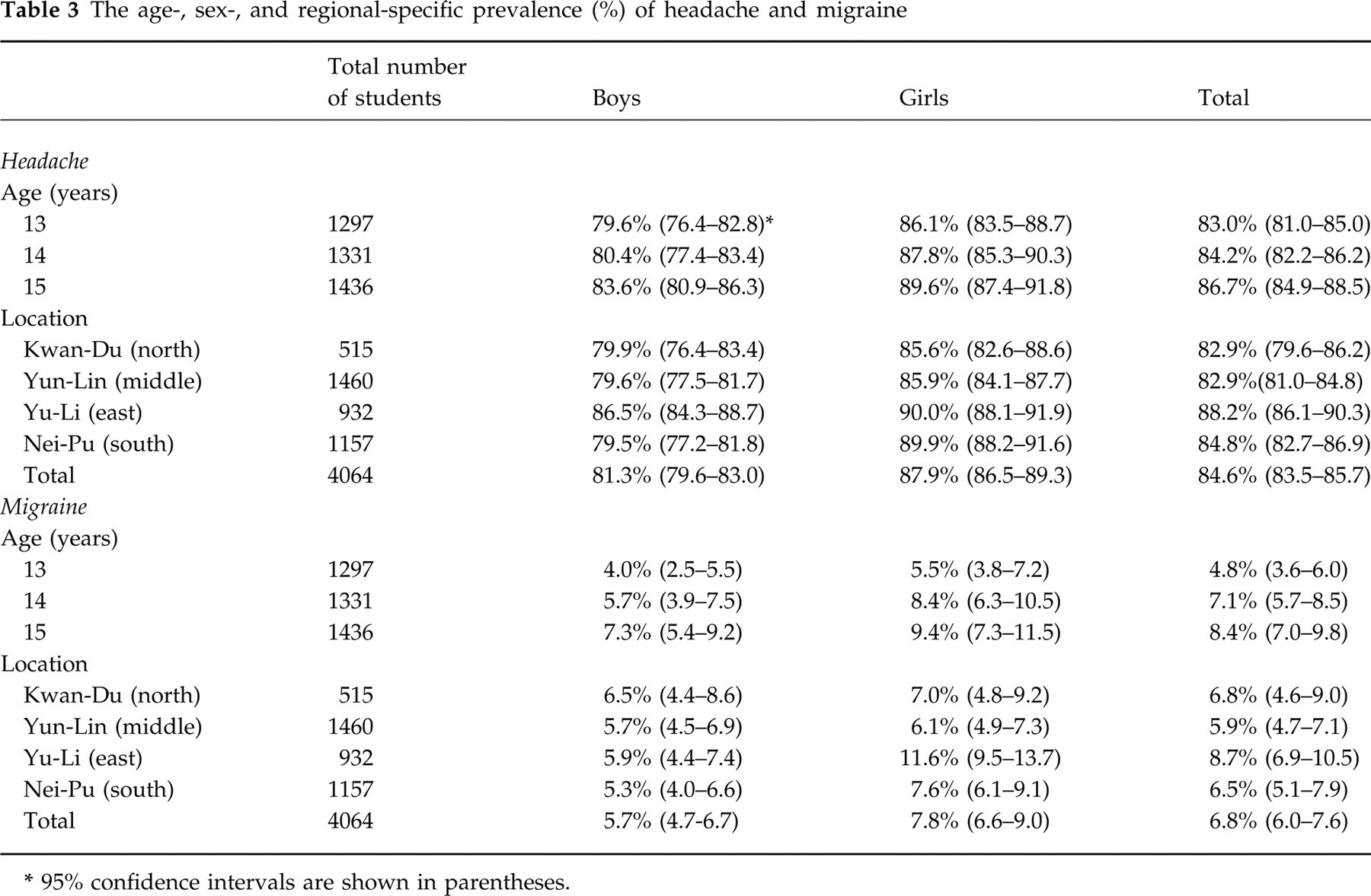
95% confidence intervals are shown in parentheses.
Prevalence of questionnaire‐diagnosed migraine
Analysis of the completed questionnaire data revealed that a total of 277 students (114 boys/163 girls) (6.8%) had migraine according to the modified IHS criteria (Table 3). The prevalence of migraine increased with age (χ2 for linear trend = 14.5, d.f. = 2, P = 0.001) in both sexes. Girls had a significantly higher prevalence than boys (7.8% vs. 5.7%, χ2 = 7.0, d.f. = 1, P = 0.008). Compared with the other schools, girls in the Yu‐Li Junior High School had a significantly higher migraine prevalence (11.6%) (χ2 = 12.5, d.f. = 3, P = 0.006) (Table 3). In contrast, no regional difference was noted in boys.
Clinical features of migraine headaches
The location of migraine headache was predominantly bilateral (58.5%) or unilateral/bilateral (36.8%), while strictly unilateral was much less common (4.7%). Phonophobia was the most common associated symptom (80.9%), followed by nausea (70.4%), photophobia (63.5%) and vomiting (59.1%). Twenty‐two percent of students with migraine reported a visual aura, but no significant gender difference was noted (16.8% boys vs. 25.2% girls, χ2 = 2.7, d.f. = 1, P = 0.10).
Menstruation and migraine
Eighty‐nine percent of girl students had already started menstruation. Girls who had started menstruation seemed to have a higher migraine prevalence than those who had not, and this finding showed a trend of significance (8.2% vs. 4.8%, χ2 = 3.4, d.f. = 1, P = 0.06). Compared with girls with non‐migraine headaches, a significantly higher percentage of girls with migraine reported that their headaches were precipitated by menstruation (17.7% vs. 10.2%, χ2 = 7.6, d.f. = 1, P = 0.006). However, the migraine attacks precipitated by menstruation did not increase with age.
Impact of migraine on school attendance in the past semester
Up to 30.4% of students with migraine had been absent from school because of headache in the past semester (1–3 days, 27.0%; ≥ 4 days, 3.4%). Only one girl with migraine had school absence of more than 14 days due to headaches. This rate of school absence was significantly higher than that in students with non‐migraine headache (30.4% vs. 14.0%, χ2 = 50.7, d.f. = 1, P < 0.0001, odds ratio (OR) = 2.7).
Headache‐related painkiller usage
Among all students with headache, 42.1% had used painkillers to relieve their headache. The frequency of painkiller usage increased significantly with age (χ2 for linear trend = 8.3, d.f. = 1, P = 0.004) but did not differ between sexes. Among the four participating schools, the frequency of painkiller usage was significantly higher in the Yu‐Li Junior High School (Yu‐Li 50.7%, Nei‐Pu 42.7%, Kwan‐Du 41.6% and Yun‐Lin 35.9%, χ2 = 43.6, d.f. = 3, P < 0.0001). Overall, 72.1% of students with migraine used painkillers for their headache, in contrast to 39.5% of students with non‐migraine headache (χ2 = 110.9, d.f. = 1, P < 0.0001, OR = 4.0). As many as 11.5% of students with migraine used painkillers ≥ 1 day/week.
Discussion
This study had several methodological limitations.
Sampling bias
In this study, students from four public schools in different regions around Taiwan were chosen as our target population. Public junior high schools in Taiwan have a population which consists of more than 90% adolescents, with a wide range of socioeconomic status. Because our response rate (91.6%) was high for a population‐based study, the final participants could be regarded as a representative sample of adolescents aged 13–15 in Taiwan. A lower response rate was noted in boys, which is common in this kind of study.
Validity of questionnaire
Our questionnaire was designed based on the IHS criteria for migraine. Its sensitivity and specificity are appropriate for a field study. As in two previously reported studies (12, 13), we did not utilize the number of migraine attacks (IHS migraine criteria A) as a diagnostic criterion. In addition, migraine equivalents, which are common in children and adolescents, such as recurrent abdominal pain (14), benign paroxysmal vertigo (15) and recurrent limb pain (16), were not considered in our study. Our questionnaires inquired about four aura symptoms defined by IHS criteria. The validity of the questionnaire segment on aura symptoms was poor in the present study, as is quite often the case for a retrospective study because of incomplete memory of migraine aura (17) and the difficulty in defining so‐called ‘focal cerebral dysfunction’ by questionnaire (12). The low sensitivity of the questionnaire‐diagnosed aura might underestimate the prevalence of migraine with aura in this study.
Recall bias
Our questionnaire queried about the lifetime prevalence. ‘Telescopic effect’, that is, the reporting of events in the past at a time closer to the present, was a frequent recall bias in research based on recall (18). The increase in lifetime prevalence from age 13–15 in this study suggested that the recall bias was small.
This is the first survey of migraine using IHS criteria in adolescents of Taiwan. Our results show that the lifetime migraine prevalence in this age group was 6.8%. In comparison with the only two previous studies using IHS criteria in this age group, our migraine prevalence was higher than that in Italy (19) but lower than in the UK (9) (Table 4). These discrepancies might have resulted from differences in methodology or survey period (lifetime vs. 1 year). Racial diversity might also have played a role. Previous studies have found a low migraine prevalence in Asian adults (7, 12, 20). However, no adequate data on migraine prevalence in Asian adolescents are available.
Age‐specific migraine prevalence of adolescents in different population‐based studies using the IHS criteria

SAQ, Self‐administered questionnaire; NA, not available.
Data recalculated from original articles.
Consistent with other studies, our results showed that the prevalence of migraine in adolescents increased with age and female sex (1, 13). We found regional difference in migraine prevalence among these four schools, with the highest rate in the Yu‐Li Junior High School. As high as 25% of the inhabitants in Yu‐Li are aborigines, in contrast to < 5% in the other three regions. This finding suggests that ethnic factors may be responsible for this difference (13). The low socioeconomic status of Yu‐Li might also contribute to the high prevalence (13).
Eighteen percent of girl students with migraine reported that their headaches worsened during menstrual periods. This precipitation was less frequent in students with non‐migraine headaches, which supports the previous finding that menstrual precipitation itself is probably a migrainous feature (21). In the present study, this menstrual precipitation was observed as early as age 13 years.
In this study, 30.4% of students with migraine had school absence due to headache and 3.4% had been absent for more than 4 school days in the past semester. Abu‐Arefeh & Russell in the UK (9) reported that school children with migraine (aged 5–15 years) lost 2.8 school days due to headache in a year. For comparison, we calculated the average number of days of school absence using the mean value of each school absence category in our questionnaire. We found that students with migraine had been absent for an average of 0.78 school days due to headache in the past semester, equal to 1.6 days a year. The lower absence rate in our study was probably due to cultural factors. The severity of migraine attack is under‐recognized and school absence for headache may not be allowed in Taiwan. In addition, students may be less willing to be absent from school due to high levels of academic stress because of the need to pass a national entrance examination to enter senior high schools.
We found that painkiller usage was common in adolescents with headaches in this study. Forty‐two percent of students with headache used painkillers for relief. The prevalence of painkiller usage among adolescents with headaches increased significantly with age but did not differ between sexes, which is consistent with the findings of a previous study (11). It is not clear why students of the Yu‐Li Junior High School had a higher frequency of painkiller usage. Painkiller usage was even more common in adolescents with migraine, and up to 11.5% of them used painkillers at least 1 day per week. Because of the possibility that rebound headache might be caused by the overuse of analgesics, an early education of adolescents to prevent the transformation of migraine is mandatory.
Footnotes
Acknowledgements
This study was supported by grants from the National Science Council (NSC 89‐2314‐B‐010‐032). The authors would like to thank all the teachers and students in the Kwan‐Du, Yun‐Lin, Yu‐Li and Nei‐Pu Junior High School for their great help.