
Abstract
Deinstitutionalization has shifted the locus of psychiatric care from mental hospitals to community-based alternatives. Although the advantages of this process have been underlined [1–3], there have also been critical accounts of community-based psychiatry [4, 5]. Questions have been raised concerning the extent of service needs of some of the most severely disabled patients and the ability of psychiatric aftercare services to meet these needs [6–9], and the burden placed on the care-giving families [10, 11].
Since the beginning of the 1980s, the number of psychiatric beds in Finland decreased in less than 15 years from about four to slightly over one per 1000 population [12]. The rate of decrease of psychiatric beds was steady from 1982 on, ranging from 8% to 15% per period of 2 years [13]. The beginning of 1990s showed a rapid phase of deinstitutionalization, with a rate of decrease of psychiatric hospital beds of 21% from 1990 to 1992. In the mid-1990s the decrease of psychiatric hospital beds clearly slowed down.
The psychiatric hospitals in Finland are run by municipalities or federations of these. If the fee for hospitalization might impose financial burden, the patient is eligible for welfare benefits. Public psychiatric outpatient care is carried out mostly through a system of community mental health centres (CMHCs). By the early 1980s, the public sector CMHCs had extended their coverage over the entire country, and these services are provided free of charge. The contribution of private services to the psychiatric outpatient care of schizophrenic patients is very limited. The psychiatric outpatient services in Finland include, in addition to CMHCs, an expanding range of alternative outpatient services such as day centres, sheltered workshops, club houses, rehabilitation homes, small homes and supported residences. The number of visits to psychiatric outpatient care doubled between 1990 and 1994, without a compensating increase in personnel resources [13].
In Finland, there are several items of social support available for patients with schizophrenia. Patients are eligible for a disability pension after 1 year of continuous disability. Furthermore, they may be eligible for supplementary financial benefits, supported accommodation or home help. There are also voluntary organizations, such as church support services or mental health organizations, which may give support for schizophrenic patients.
In order to evaluate the effects of the deinstitutionalization process, a national project on Discharged Schizophrenic Patients (DSP) was launched in Finland in 1987. In our previous studies of the first three patient cohorts within the DSP project (i.e. patients discharged during 1982, 1986 and 1990) we found that the rapid deinstitutionalization process has led to major changes in the characteristics of discharged patients with schizophrenia and their need for services [14, 15]. Thereafter, one more cohort (patients discharged in 1994) was investigated. There was no increase in mortality rate between the cohorts [16]. In general, during the observation period of this study the use of alternative outpatient facilities had increased, while the proportion of patients who were totally out of contact with psychiatric or primary health care services after discharge had diminished [17]. Differences in psychosocial and clinical characteristics, however, and in secular changes in these characteristics, has remained unknown among patients in different treatment settings.
The aim of the present study is to investigate schizophrenic patients’ symptoms, psychosocial functioning and disabilities in various treatment settings at followup, and how these have changed during the era of rapid deinstitutionalization, from the mid-1980s to the end of the 1990s, in Finland. We anticipated changes especially among the group of patients using community-based residential and day care services and, on the other hand, among the group of drop-outs.
Method
The DSP samples comprised 4338 schizophrenic patients, aged 15–64 years, who had been discharged from the psychiatric hospitals of 20 mental health/health care districts in Finland after January 1, 1982 (S82), January 1, 1986 (S86), January 1, 1990 (S90) and January 1, 1994 (S94) with the official place of residence in any of the study districts. In each of the districts, altogether having a population of nearly 4 million (the total population of Finland is about 5 million), all consecutive patients with schizophrenia discharged from the psychiatric hospitals were included in the study until the samples consisted of 30 patients per 100 000 population. The demographic structure and the socioeconomic situation of the population in the study districts, as well as the health care services available in these districts, were representative of those found for the whole country [16].
Sampling was based on the Finnish hospital discharge register [18, 19]. The required number of patients with schizophrenia who met the study criteria were selected in order of discharge from among those whose diagnosis was a functional (non-organic) psychotic disorder. In 1982 and 1986, the diagnoses were based on the International Classification of Diseases [20] and, in 1990 and 1994, on the Finnish Classification of Diseases 1987 [21]. The researcher-physicians in each district reviewed the case records and assigned the research diagnoses for the patients using the DSM-III-R criteria included in the Finnish Classification of Diseases 1987. Patients suffering from disorganized (2951), catatonic (2952), paranoid (2953), residual (2956) and undifferentiated (2959) schizophrenia were included in the study; patients with schizoaffective and schizophreniform disorders were excluded. In a separate reliability study, four research-physicians blindly re-reviewed the case records of 40 randomly selected study patients and of 40 non-schizophrenic patients discharged next to the study patients. The researchers classified all the study patients as schizophrenic patients (i.e. the agreement with the primary research diagnoses was complete) [22].
The total numbers of patients with schizophrenia included in the DSP project were 1081 (S82), 1097 (S86), 1129 (S90) and 1031 (S94). On the basis of psychiatric case records, data were collected on the patients’ psychiatric history and use of services during the three-year period after the discharge. Data on the patients’ overall level of functioning, determined by using the Global Assessment Scale (GAS) [23] at discharge, were collected from the case notes.
Three years after discharge, the S86, S90 and S94 patients were traced in order to seek their consent to participate in the study. As informed consent was obtained, the interviews were conducted by each district's psychiatric professionals (psychiatrists, psychologists, psychiatric nurses, social workers) using a structured interview schedule specifically designed for the purposes of the present study. It included well-defined questions concerning the patient's clinical and functional state, disturbances in social behaviour and use of various psychiatric services.
The patients’ psychotic symptoms were assessed by a psychiatrist during a comprehensive clinical interview with the help of a separate symptom checklist. The psychotic symptoms classified included, for example, hallucinations, delusions and strong feelings of depersonalization or derealization. The severity of the symptoms was rated using five categories (i.e. no symptoms, mild, moderate, severe, constantly severe). The reported prevalence of psychotic symptoms refer to the presence of psychotic symptoms, however mild.
The patients’ physical health as well as use and abuse of alcohol were assessed by the clinical interview and according to the medical records. Physical health was assessed with a 4-point scale (no symptoms, somatic symptoms but no disorder, mild somatic disorder, severe somatic disorder) and alcohol use was assessed on a 4-point scale (little use, moderate use, intermittent abuse, constant abuse). The reported prevalences of alcohol abuse refer to either intermittent or constant abuse.
Psychosocial functioning was assessed on the GAS. In addition to this global measure, the patients’ functional ability was assessed using a modified version of the Medical Research Council Practices Profile [24]. In this version, 19 structured items included questions on housework, self-care (hygiene, use of toilet, eating, getting up/going to bed), taking medications, assuming responsibility for one's own care, managing money, taking care of children, working, marital relationship, other interpersonal relationships, social contacts outside family, embarrassing behaviour, social withdrawal, interest in current events, activity, managing emergencies and suicidal behaviour. The patients were asked how they coped with these areas of social role behaviour.
The present study is based on the three cohorts for whom interview data are available. Interviews were conducted with 775 patients (71%) of the S86 cohort, and 40 (4%) were examined by other means; 233 (21%) refused to participate in the study or could not be located, and 49 (4%) had died. The corresponding figures for the S90 cohort were 742 (66%), 96 (9%), 219 (19%) and 72 (6%); and for the S94 cohort, 663 (64%), 62 (6%), 255 (25%) and 51 (5%), respectively. In terms of sociodemographic background factors, there were no statistically significant differences between the patients who were interviewed and those who were not. In general, the patients who were interviewed were more disturbed at discharge and they had used psychiatric services to a greater extent both before and, in particular, after the discharge, compared with the others.
In the present study, the subjects were classified into five groups according to their treatment setting at follow-up (Table 1). The first group comprised those who had no care (NC), (i.e. were not in touch with either primary health care or psychiatric services at follow-up); the second group comprised those who were in touch with primary health care services only (PHC); the third group comprised those who visited community mental health centres only (CMHC); the fourth group comprised patients using alternative outpatient facilities (e.g. day care, day hospitals, rehabilitation homes) (AF); and the fifth group were those who were hospitalized at follow-up (HOS). We compared these five groups of patients with each other and across successive cohorts in terms of gender, duration of illness and GAS at discharge, as well as the use of services during the three-year follow-up period after discharge, and the patients’ clinical symptoms, psychosocial functioning (GAS) and disabilities at follow-up.
Treatment settings of schizophrenic patients 3 years after discharge in three different cohorts in Finland (%)
In statistical analysis, means and standard deviations were used for normally distributed continuous variables, medians and lower (Q1) and upper (Q3) quartiles for continuous variables with skewed distributions and percentages for categorical variables. To test the differences between the treatment settings in each cohort or between the cohorts in each treatment setting, one-way analysis of variance (ANOVA), Kruskal–Wallis one-way analysis of variance or χ2 tests were used. A probability level of < 0.05 was considered as statistically significant. The data were analysed using SPSS for Windows version 9.0 statistical software.
The ethical committees of the Tampere University Hospital and the Turku University Central Hospital gave their approval for the study.
Results
Gender, age, duration of illness and psychosocial functioning at discharge
There were no gender differences between the patients in different treatment settings at follow-up or between the cohorts in each treatment group (Table 2). With regard to age, in each cohort there was a significant difference between the patients in various treatment settings; the NC patients, and especially the PHC patients, were older than the others. Between the cohorts, the patients’ age increased in the NC (F = 3.086, df = 2, p = 0.048), the CMHC (F = 6.546, df = 2, p = 0.001) and the HOS group (F = 15.346, df = 2, p < 0.001). In each cohort, the duration of illness differed between the treatment setting groups. The average duration of illness in the PHC group was longer than in the others. In each treatment group, except the AF group, the patients’ duration of illness became longer from one cohort to the next (NC: F = 5.157, df = 2, p = 0.006, PHC: F = 4.312, df = 2, p = 0.015; CMHC: F = 8.524, df = 2, p < 0.001; HOS: F = 9.112, df = 2, p < 0.001). At discharge, the psychosocial functioning of the CMHC patients was better than that of the other patients (Table 2). The psychosocial functioning of the AF patients worsened after the first cohort (F = 4.035, df = 2, p = 0.018).
Characteristics of schizophrenic patients at discharge in three different cohorts by treatment setting at follow-up
Use of services during the three-year follow-up period after discharge
In each cohort, patients who were hospitalized at follow-up had been readmitted more often than others during the three-year follow-up period (Table 3). The differences between the cohorts in the number of readmissions were not significant in any of the treatment groups. In each cohort, patients of the AF group had more often visited outpatient services during the follow-up period than the others (Table 3). The number of outpatient visits tended to increase between the cohorts in all patient groups; the differences however, reached statistical significance only in the PHC (χ2 = 11.104, df = 2, p = 0.004), in the CMHC (χ2 = 59.478, df = 2, p < 0.001) and in the HOS group (χ2 = 7.148, df = 2, p = 0.028).
Use of services of schizophrenic patients during the three year follow-up period in three different cohorts by treatment setting at follow-up
Clinical status at follow-up
In each cohort, the HOS patients suffered from psychotic symptoms at follow-up more often than the others (Table 4). With regard to the S90 cohort however, the NC patients had psychotic symptoms nearly as often as those in the HOS group. In the NC (χ2 = 12.712, df = 2, p = 0.002) and the AF groups (χ2 = 6.280, df = 2, p = 0.043), the successive cohorts differed in the proportion of patients with psychotic symptoms. In both groups the proportion of patients with psychotic symptoms increased after the first cohort, although in the NC group, the proportion of psychotic patients decreased again in the last cohort.
Clinical and functional status of schizophrenic patients 3 years after discharge in three different cohorts by treatment setting at follow-up (%)
The treatment setting groups differed in the number of patients with somatic disorders in the first two cohorts; in the first cohort somatic disorders appeared more often among the PHC patients than among the others. In the second cohort, both the PHC and the NC patients had somatic disorders more often than the others. A significant difference also emerged between the cohorts in the proportion of patients with somatic disorders in the NC group (χ2 = 7.962, df = 2, p = 0.019), the AF group (χ2 = 9.528, df = 2, p = 0.009) and the HOS group (χ2 = 6.524, df = 2, p = 0.038). In the NC group, the proportion of patients with somatic disorders was largest in the second cohort, whereas in the AF and the HOS group, the proportion was largest in the last cohort.
In the first and last cohorts, the AF patients abused alcohol less often than the others. The proportion of patients with alcohol abuse increased in the AF group during the observation time (χ2 = 7.522, df = 2, p = 0.023). Altogether, however, reported alcohol abuse was rather uncommon among all patients in each cohort. In addition to recent alcohol problems, the patients in the last cohort were also asked whether they had used other psychoactive substances during the previous year. About 5% of the patients had used such other substances.
The differences in psychotic symptoms, somatic disorders or alcohol abuse between the patients in the various treatment settings remained significant even when GAS at discharge and duration of illness were controlled for.
Psychosocial functioning at follow-up
Impairment in social functioning was common among all patients. In the HOS group, nearly all patients had at least one disability in social functioning (Table 4). In the AF group, the number of patients with disabilities increased in the successive cohorts (χ2 = 7.331, df = 2, p = 0.026).
At follow-up, the psychosocial functioning of patients was poorest among the HOS patients (1986: F = 28.6185, df = 4, p < 0.001; 1990: F = 17.7046, df = 4, p < 0.001; 1994: F = 15.2416, df = 4, p < 0.001). Furthermore, only in the HOS group did the change between the average GAS score at discharge and the GAS score at follow-up appear to be negative (Fig. 1). The differences in psychosocial functioning between patients in various treatment settings remained significant even though GAS at discharge and duration of illness were controlled for.
The change in psychosocial functioning (the mean Global Assessment Scale score) of schizophrenic patients between discharge and follow-up. □, cohort 1986; ▪, cohort 1990; □, cohort 1994. NC, no care; PHC, primary health care services only; CMHC, community mental health centres only; AF, alternative outpatient facilities; HOS, hospitalized at follow-up.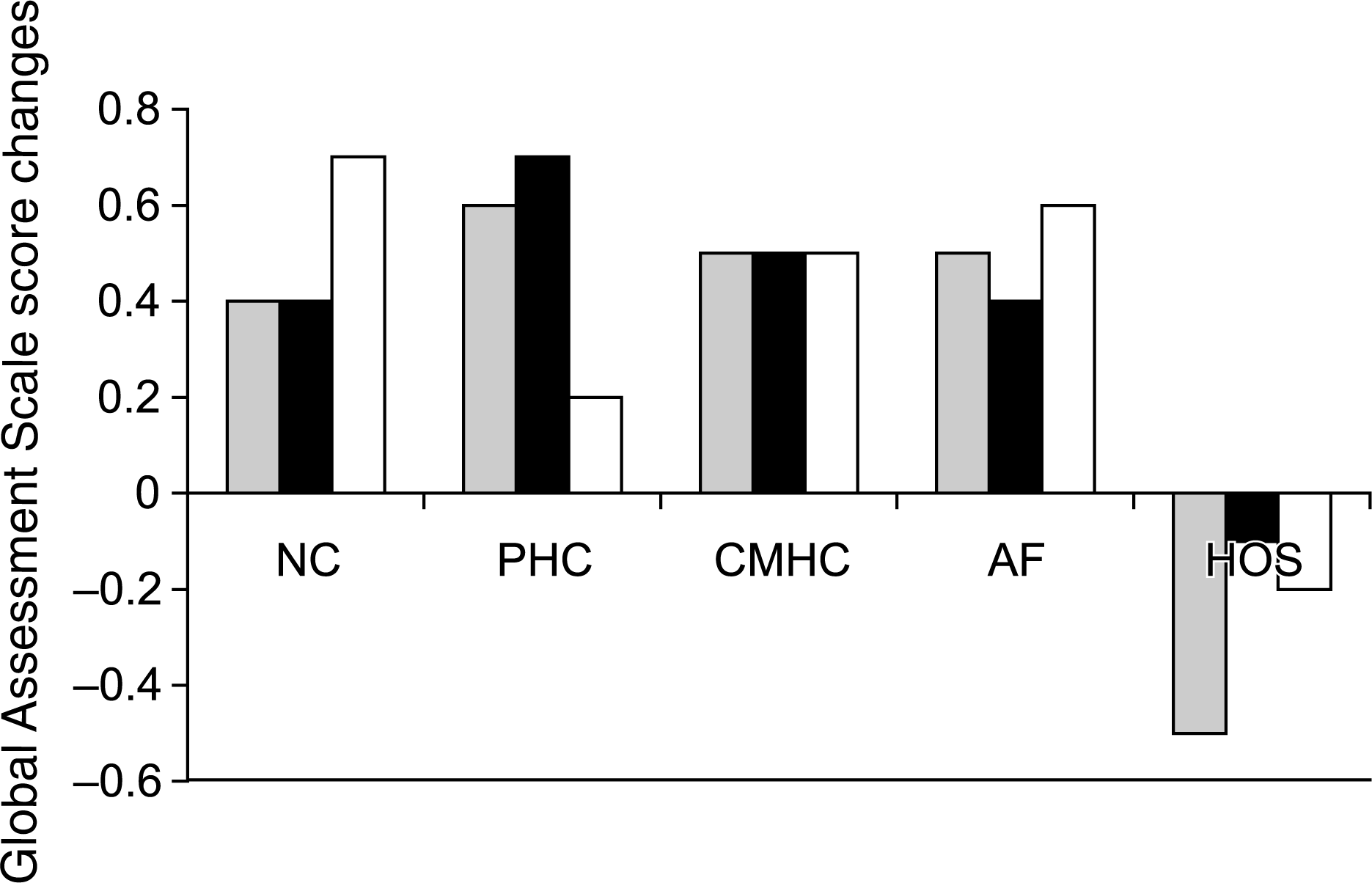
Discussion
During the observation period of the study (late 1980s to the end of the 1990s) the proportion of patients who were to use community-based residential and day care services increased. In the late 1990s about 30% of patients planned to use these facilities after discharge. We found that in the 1990s these patients were already in poorer condition at discharge than patients in the previous decade. Consequently, in the late 1990s the number of patients with psychotic symptoms and somatic disorders as well as social disabilities increased in the alternative outpatient facilities, thus placing more demands on the staff. Our findings are in line with those from other countries: the patients deinstitutionalized in most recent years tend to be more disabled than prior discharge samples, and they often have special behavioural problems that make them difficult to place and maintain in community settings [8, 25]. However, it is notable that in the present study the overall level of functioning, as measured by the GAS, had improved after discharge among the patients using the community-based residential and day care services. Thus, in spite of the growing number of discharged patients who were in poor condition, these alternative outpatient facilities may have been able to meet the needs of these patients at least satisfactorily.
Earlier studies have shown that persons with schizophrenia are at increased risk for comorbid substance use disorder [26, 27]. In addition to the high risk of a lifetime substance use disorder, the rates for recent alcohol and drug use are also high, about one-quarter to one-third of patients with a recently active substance use disorder [28]. As a result of deinstitutionalization, people with schizophrenia may experience a high rate of regular exposure to psychoactive substances and the social pressures to use them. In the present study the rate of recent alcohol abuse among patients with schizophrenia appeared to be rather low (i.e. 10–15% in each cohort). The abuse of alcohol seemed to be particularly rare among patients who were regularly using community-based residential and day care services. This may have contributed to the fact that in spite of their otherwise poor psychosocial functioning, they managed to live outside the hospital. However, it is somewhat worrying that during the observation period alcohol abuse in this patient group was increasing.
A recent questionnaire-based population study found that about 11% of a representative sample in Finland to be currently (12-months prevalence) alcohol dependent [29]. There is no data on the changes in prevalences of alcohol use disorders in the Finnish general population. On the other hand, the drinking patterns have been studied during the period of the 3 cohorts of the present study [30]. In the latest specific drinking pattern survey from the year 2000, no major changes have been found since 1992. So far, it remains unclear whether the rate of alcohol abuse among patients with schizophrenia parallels that in the general population.
In the present study, except for the last cohort, we collected data on use and abuse of alcohol only. Until recently the abuse of psychoactive substances other than alcohol has not been common in Finland [31, 32]. In the last cohort, only about 5% of all discharged patients with schizophrenia had been using illegal drugs during the year preceding the follow-up.
Socially isolated schizophrenic patients with a severe current disorder are at particular risk of outpatient nonattendance and subsequent admission [33]. The results of our earlier study of patients discharged in 1986 indicated that the patients who were out of touch with psychiatric care at follow-up were more disabled compared with those in community care [34]. It was suggested that their community care would have required more attention to prevent them from losing contact with services. In the present study, which included patients discharged during the 1990s, the clinical state of the patients who had dropped out of all treatment had become even worse in the beginning of the 1990s; in fact, at follow-up, they had as many active psychotic symptoms as the inpatients. About half of the drop-outs were having problems with their somatic health as well. However, at follow-up at the end of the 1990s, the psychiatric as well as the somatic state of this patient group had improved, although they had been in poorer condition at discharge. During the 3-year follow-up period after discharge, patients in the last cohort had more often used psychiatric services compared to those in the previous cohorts, and this may have had a positive effect on their mental and somatic health. By paying attention to this special group of schizophrenic patients (i.e. the drop-outs), it may have been possible to enhance their use of services and thus also their psychosocial functioning at follow-up. Recently, a study of patients with schizophrenia and related psychotic disorders living in supported housing showed that direct supervision of medication is associated with better adherence in residential treatment settings [35].
In each cohort, the patients’ psychosocial functioning, as measured by the GAS, had improved after discharge. The group of patients who were rehospitalized at follow-up were an exception. In each cohort this group of inpatients had also been readmitted during the 3-year follow-up more often than the others. On the other hand, during the 3-year follow-up period, these patients had not used community-based services less often than the others, and the number of their outpatient visits had increased during the study period. Thus, between the hospitalizations, these patients did not constitute a group of drop-outs. Their community care, however, had not been sufficient enough to improve their clinical state and psychosocial functioning after discharge. It seems, in fact, that those who were inpatients at follow-up were actually in the right treatment setting considering that their clinical state and psychosocial functioning was significantly lower than those of the others, thus making their life in the community difficult.
In the 1990s the length of index hospital stay of patients with schizophrenia decreased and there were only few long-stay patients (i.e. length of stay over 5 years). Design of the present study might have been enhanced by each cohort having a comparison group who had remained in hospital measured on similar parameters. However, while there were only few longstay patients, it would not have been possible to find enough patients for a diagnostically and length of stay matched comparison group for the follow-up interview three years after discharge.
The present study is in line with a recent German study of long-term hospitalized psychiatric patients [36]. In that prospective, controlled study the patients who remained in hospital care did not show significant changes during the one-year follow-up period whereas those discharged did, suggesting that long-stay patients can benefit from discharge into the community, particularly with respect to their quality of life. On the basis of the results of the Team for the Assessment of Psychiatric Services (TAPS) project, a prospective study dealing with the outcome of a population of long-stay psychiatric patients resettled in the community in Britain, Trieman, Leff and Glover [2] pointed out that carefully planned and adequately resourced community care for long-stay psychiatric patients is beneficial to most. Similarly to the TAPS project, a recent Australian study by Hobbs et al. [6] demonstrated the clinical effectiveness of deinstitutionalization, when planned within a mental health system with adequate community resources. Also, in the Netherlands, where the deinstitutionalization process has been slow in comparison to a large part of Europe, day treatment, sheltered residences and assertive home treatment have proved to be effective alternatives rather than additions to inpatient care; between 1989 and 1997 the use of alternative community services grew significantly and the average length of stay in the hospital reduced by 33% [37]. On the other hand, the results of the TAPS project implied that, even with the best treatment and adequate support, patients with schizophrenia or other chronic severe disorders are prone to exacerbation of symptoms that necessitate periodic admissions. Similarly to the present study, a considerable proportion of the TAPS sample required transient readmissions, thus creating a steady demand on local services for acute admissions.
The large patient cohort samples of the present study represent schizophrenic patients discharged in the whole country. All the patients in this study had been discharged from psychiatric hospitals; thus, the results can not be generalized to those schizophrenic patients who had used outpatient services only. During the observation period patients’ average duration of illness increased from 10 to 16 years. The study sample thus represents long-term patients with schizophrenia. The participation rate for the follow-up interviews was high. Those who were examined at follow-up were more disturbed at discharge and they had used psychiatric services more often than the patients who were not examined. There was no indication, however, that the differences between those who took part in the follow-up study and those who did not was systematically different in the cohorts studied.
The clinical and social outcome of patients in different treatment settings was assessed by clinical interviews. We did not use internationally standardized rating scales for the measurement of psychotic symptoms. Use of such scales would have increased validity and reliability and made international comparisons easier. However, each interviewer had a separate, detailed instruction list regarding the assessment of severity of psychotic symptoms.
Data on the patients’ overall level of functioning at discharge (via the GAS) was collected from case notes, whereas at follow-up it was assessed on the basis of the interview. The GAS assessment had been in systematic routine clinical use in Finnish mental hospitals during the whole study project, and the scores collected from the case notes had been assessed by psychiatric teams trained in the use of this measure. The research interviewers, all of who were psychiatric professionals, made the GAS assessments at follow-up. The interrater reliability of the GAS scoring was not investigated in the present study. A number of earlier studies, however, have reported that the reliability is adequate [23, 38]. Although the reliability has been lower among clinicians than researchers, the raters of the present study were trained in the use of the GAS, which has been shown to improve the reliability of the assessments [39].
Conclusion
After a particularly rapid decrease in the number of psychiatric hospital beds in Finland in the 1980s, the psychiatric treatment system has worked rather well for most discharged schizophrenic patients during the 1990s. The use of community-based rehabilitation and day care services has increased and the proportion of drop-outs has decreased. As expected, the characteristics of these two patients groups had changed since the 1980s. In the late 1990s more patients with a poor clinical and psychosocial state were using community-based residential and day care services, while the psychiatric and somatic state of the small group of dropouts had somewhat improved. In general, fears that the deinstitutionalized patients were destined to downfall of psychosocial functioning have been unfounded. In the future, however, alcohol abuse and especially the potentially increasing abuse of other psychoactive substances may create new demands for the services. As the locus of care is shifting more and more to community-based alternatives, and at the same time more disturbed patients are transferred into these facilities, as shown in the present study, it is extremely important that the quality of care and adequate resources are ensured, and that the training needs of the staff are recognized.
Footnotes
Acknowledgements
We thank the members of the psychiatric teams for their help in data collection. This study was supported financially by the health care and mental health care districts that participated in the study, the Academy of Finland, the National Board of Health, the Association of Finnish Mental Hospitals and the League of Hospitals in Finland.