
Abstract
The present study is a 16-year follow-up study assessing the long-term outcome of migraine with aura (MA). Additionally possible predictive factors in the prognosis of MA were evaluated. Patients were recruited from the files of Danish headache clinics. A total of 53 patients (11M:42F) with MA (IHS criteria) participated in a follow-up interview. At follow-up attacks had ceased (no MA for 2 years) in 36% of patients. Attacks had ceased in 55% of males and 31% of females (P = 0.17). Attacks had ceased in 41% of patients with visual aura without other aura symptoms and in 25% of those with sensory or aphasic aura besides their visual aura (P = 0.36). Among those with attacks of MA at follow-up frequency of attacks and headache intensity was improved in 44% and 41% of the patients, respectively. The results point to a favourable evolution of MA and suggest possible predictive factors.
Introduction
To guide patients with migraine with aura (MA) properly and to identify pathophysiological subgroups of MA it is essential to analyse the long-term outcome of MA and to identify possible predictive factors in the prognosis. Both can be analysed by doing long-term follow-up studies. Since epidemiological, genetical and pathophysiological evidence suggest that MA and migraine without aura may be distinct entities it is essential to analyse MA and migraine without aura separately (1–3). Several studies have evaluated the outcome of unspecified migraine or migraine without aura. However, only two studies have previously described the long-term outcome of MA diagnosed according to the operational diagnostic criteria of the International Headache Society (IHS-criteria) (4). The first study reported a favourable evolution of MA over time and identified several nonsignificant favourable predictive factors in the prognosis of MA (5, 6). The second study identified visual aura without other aura symptoms as a statistically significant favourable predictive factor in the prognosis of MA in children (7).
The aim of the present study was to analyse the long-term outcome of MA with regard to change in attack frequency and headache intensity of MA over time. Furthermore, to examine the prognostic significance of gender, number of aura symptoms, and age at onset of MA in predicting the cessation of MA-attacks.
Materials and methods
Study design
The patients were recruited from case records of the headache clinic at the Danish National Hospital or from Professor Jes Olesen's clinic at Glostrup Hospital. The case records were specifically designed to report symptoms of migraine and other headaches and furthermore included the outcome of a physical- and neurological examination. All patients had previously been interviewed and examined by a neurologist or a neurological resident trained in headache diagnostics. Approximately 2570 case records from 1977 to 1984 were screened for patients with MA. Exclusively patients with a detailed aura description presumed to fulfil the IHS-criteria of migraine with aura (IHS 1.2) were included. Patients with chronic tension-type headache or suspected of drug abuse were excluded. Drug abuse was defined as intake of a daily dose of headache medication every or every second day. The patients for enrolment received a written invitation, where they were asked to participate in a telephone interview regarding the natural history of their headache, before they were contacted by phone. The letter included a return slip and a prepaid envelope. The patients were contacted by telephone unless they stated they did not want to participate. All participants were telephone interviewed by a trained medical student (MKE). The semistructured telephone interview was based on the IHS-criteria and has previously been validated (8, 9). The project was approved by The Danish Ethical Committees.
Study population
Approximately 450 of the screened case records were presumed to describe patients with MA. Only 75 patients fulfilled the inclusion criteria of whom four patients were excluded due to chronic tension type headache and four patients were excluded due to drug abuse. Of the remainder 67 patients six patients were deceased and one had emigrated at the time of follow-up. Three patients refused to participate for unspecified reasons and four patients could not be located. A total of 53 patients participated in the follow-up telephone interview. The participation rate was 88% (53/60).
Statistical analysis
Statistical analysis was performed using SPSS Base System 8.0 statistical software. The Wilcoxon's test, Fisher's exact test, or Mann–Whitney test was used as appropriate depending on the type of data. A five percent level of significance was used.
Results
Patient characteristics
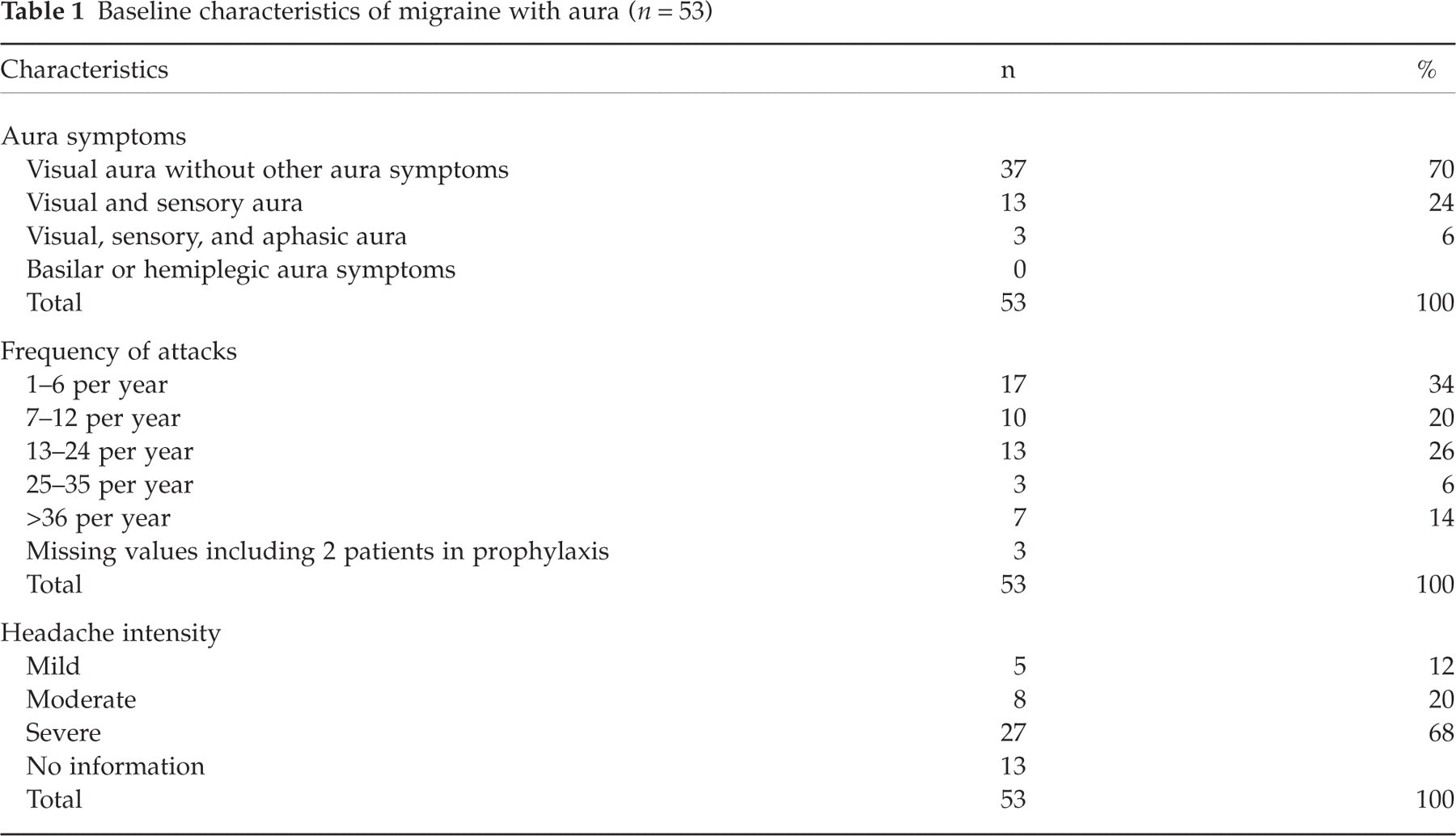
The 53 patients comprised 11 males (M) and 42 females (F). The M: F sex-ratio was 1 : 3.8. The median age was 34 years (range 12–66 years) at baseline and 52 years (range 27–80 years) at the time of follow-up. The median age at onset of migraine with aura (MA) was 19 years (range 4–55 years). The characteristics of MA of the participants from baseline records are shown in Table 1. The frequency of attacks were reported by the patients in a continuous fashion and then classified according to the categories in Table 1. The headache intensity was reported by the patients according to the categories in Table 1. The baseline characteristics of the nonparticipants was similar to those of the participants with regard to age at onset (6–40 years), age at follow-up (30–60 years), gender distribution (2M, 12F), aura symptoms, attack frequency, and headache intensity.
Baseline characteristics of migraine with aura (n = 53)
Long-term outcome of migraine with aura
The median follow-up period was 16 years (14–21 years). At follow-up attacks had ceased in 19 of 53 (36%) patients. Cessation of attacks was defined as no MA for at least 2 years. Seventeen (32%) patients had been attack-free for more than 5 years. One patient had been attack-free for one year only. The median age at 2 years cessation of MA-attacks was 40 years (range 20–70 years).
An improvement was noted among patients still having MA-attacks. Eleven (44%) patients had less frequent attacks. That is, the frequency of attacks of the patients moved to a better category according to the categories defined in Table 1. Five (20%) patients had more frequent attacks and 9 (36%) patients had no change in attack frequency (P = 0.12, Wilcoxon's test). Nine patients on prophylactic medication or without data were not included in the analysis. Eleven (41%) patients had reduced headache intensity of MA of whom 7 patients had totally absent headache. That is, the headache intensity of the patients moved to a better category according to the categories defined in Table 1. Six (22%) patients had more severe headache and 10 (37%) patients had no change in headache severity (P = 0.062, Wilcoxon's test). Seven patients on prophylactic medication or without data were not included in the analysis. Combined analysis of the patients experiencing improvement of MA showed that 3 patients had both less frequent and less severe MA-attacks, 8 patients had exclusively less frequent attacks, and 8 patients had exclusively less severe attacks
Of the 34 patients still having MA-attacks, 27 patients experienced a headache during attacks (IHS 1.2) and 7 patients exclusively experienced aura without headache (IHS 1.2.5). Seven of the 27 patients who experienced a headache during MA-attacks occasionally experienced migraine aura without headache (1.2.5). Of the 34 patients still having MA-attacks 11 (32%) patients experienced migraine without aura at follow-up. Of the 19 with cessation of MA-attacks 7 (37%) patients experienced migraine without aura at follow-up. The concurrent primary headache diagnoses of patients still having MA-attacks and the current diagnoses of patients with cessation of MA-attacks are shown in Table 2. The concurrent primary headache diagnoses at baseline were not recorded.
Current diagnoses of primary headaches (n = 53)

Possible predictive factors in the prognosis of migraine with aura
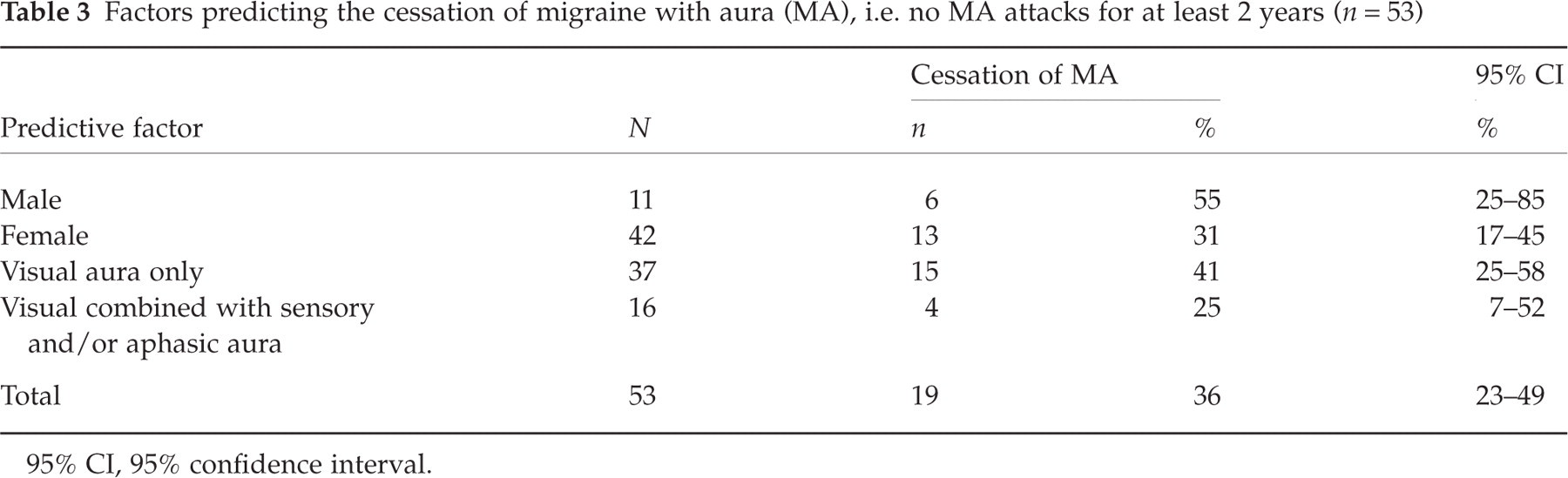
MA-attacks had ceased (no MA for at least 2 years) in 6 (55%) of 11 males compared to 13 (31%) of 42 females (P = 0.17, Fisher's exact test). MA-attacks had ceased in 15 (41%) of 37 patients with visual aura without other aura symptoms compared to 4 (25%) of 16 patients with sensory or aphasic aura besides their visual aura (P = 0.36, Fisher's exact test) (Table 3). Among the 15 patients with cessation of MA-attacks exclusively with visual aura 5 were males and 10 were females. Among the 4 patients with cessation of MA-attacks with sensory or aphasic aura besides their visual aura 1 was male and 3 were females. Among males with cessation of MA-attacks (and among males in general) the median length of follow-up was 18 years. Among females with cessation of MA-attacks (and among females in general) the median length of follow-up was 16 years. The median age at baseline was 25 years among males with cessation of MA-attacks and 24 years among men in general. The median age at baseline was 42 years among females with cessation of MA-attacks and 38 years among females in general. Sub-analysis of patients categorized according to the presence or absence of different aura symptoms, and to the cessation or continuation of MA-attacks showed no difference in the median length of follow-up. Among patients exclusively with visual aura, the median age at baseline was 34 years among patients with cessation of MA-attacks and 35 years among patients still having MA-attacks. Among patients with sensory or aphasic aura besides their visual aura, the median age at baseline was 28 years among patients with cessation of MA-attacks and 29 years among patients still having MA-attacks.
Factors predicting the cessation of migraine with aura (MA), i.e. no MA attacks for at least 2 years (n = 53)
95% CI, 95% confidence interval.
The median age at onset of MA was 26 years in patients with cessation of MA-attacks compared to 17 years in patients still having attacks (P = 0.075, Mann–Whitney test). The median length of time having MA was 11 years (inter quartile range (IQR) 1–26 years) in patients with cessation of MA-attacks and 28 years (IQR 20–40 years) in patients still having attacks. The patients with cessation of MA-attacks and those still having MA-attacks did not differ with regard to age at baseline (P = 0.66, Mann–Whitney test), baseline frequency of attacks (P = 0.85, Mann–Whitney test), baseline headache intensity of MA (P = 0.59, Mann–Whitney test), and length of follow-up (P = 0.99, Mann–Whitney test).
Discussion
Patients were diagnosed using the widely accepted diagnostic criteria of the International Headache Society in a validated semistructured telephone interview (4, 8, 9). A long follow-up period furthermore supports our results of the natural history of migraine with aura (MA). However, it should be borne in mind, that the study is retrospective which makes it difficult to monitor the periodicity of migraine and implies a risk of recall bias. Furthermore, the study population is selected because it consists of patients referred to a headache clinic. Therefore there is a risk that patients came to the clinic at a time with frequent attacks. Thus, an improvement at follow-up could, to some extent, reflect the fluctuation in attack frequency and severity. The participation rate was high. This is probably due to the recruitment procedure and due to the fact that the study population comprised patients who had previously been in contact with a headache specialist. The number of patients included in our study was limited by the strict IHS-criteria which were applied to patients with MA previously diagnosed according to the Ad Hoc Committee on Classification of Headache (10) and only patients with full details available for IHS classification were included. Most of the screened case records of patients with MA lacked information on the characteristics of MA. That is, most case records did not describe the duration of the aura, the gradual spread of the aura, or the relation between the aura and a related headache. Therefore, most screened cases did not fulfil the IHS-criteria and could therefore not be included in the study. As a result only 75 patients fulfilled the inclusion criteria. It is uncertain whether the following selection of patients is a bias. Due to the size of the study population analysis for confounders were not performed and therefore, it was not possible to discover confounding bias.
However, the present study clearly points to a favourable evolution of MA over time. At 16-years follow-up approximately one third of patients had been free from MA-attacks for more than 5 years. Additionally, an improvement was noted among patients still having attacks, i.e. 44% had less frequent attacks and 41% had less severe attacks. Thus, our results confirm previous studies. Cologno et al. (5) did a 10–20-year follow-up of 81 subjects, aged 11–63 years (26M: 55F) with an IHS diagnosis of MA (except concerning the minimum number of attacks). At the time of follow-up 35% of patients had been attack-free for at least 1 years and 19% of patients for at least 5 years. In patients still having attacks at 1 years follow-up 9% had less frequent attacks and 36% had less severe attacks. Balottin et al. (7) did a 7-years follow-up of 45 subjects aged 7–17 years (M16: 29F) with an IHS diagnosis of MA. Six patients had basilar migraine and one patient had familial hemiplegic migraine. At the time of follow-up 62% of patients had been attack-free for at least 18 months.
The present study suggests a favourable prognosis among males (despite length of follow-up as a possible confounding bias), among those who only experience visual aura (despite age as a possible confounding bias), and among those with late onset of MA. The longer the patients had suffered from MA, the less likely was the cessation of attacks. Factors as age, attack frequency, headache intensity, and length of follow-up showed no direct relation to cessation of MA-attacks. Previously Ballottin et al. (7) found that a visual aura without other aura symptoms was a significant favourable predictive factor in the prognosis of MA in children. Balottin et al. (7)also found a positive relation between migraine with typical aura or long duration of the aura, and cessation of MA-attacks in children. Cologno et al. (6) found a weak positive relation between gender or type of aura, and cessation of MA-attacks in adults. Cologno et al. (6) also identified a family history of MA, the absence of other forms of primary headache, and the absence of light stimulation as trigger factor as nonsignificant favourable predictive factors in the prognosis of MA. A comparison of factors predicting the cessation of attacks of MA is shown in Table 4.
Comparison of factors predicting the cessation of attacks of migraine with aura (MA). The table includes positive predictive factors reported by at least two studies

Cessation of attacks was defined as no MA for at least 2 years
∗, 18months
†, or 1 years
‡, respectively.
In conclusion our results indicate that cessation of MA is likely among males, among those who only experience visual aura, and among those with late onset of MA. However, women, patients with sensory or aphasic aura besides their visual aura, and patients with early onset of MA tend to continue with MA but with less frequent and less severe attacks.