
Abstract
The hypothesis that viruses or other infectious agents may cause schizophrenia or other serious psychiatric disorders dates back to the 19th century. Over recent decades, many studies have examined the putative role of prenatal viral infection as a risk factor for schizophrenia [1]. A number of authors have suggested that prenatal infection with polioviruses could contribute to the development of schizophrenia [2]. However, previous studies comparing the incidence of poliomyelitis and the number of births of individuals who develop schizophrenia have yielded mixed results. In the United States, neither Watson and colleagues [3] nor Torrey and colleagues [4] found an association in Minnesota, whereas the latter study found a significant correlation in Connecticut, where poliomyelitis preceded the schizophrenia births by 18 months. A study in England and Wales [5] found no relationship between the number of deaths from poliovirus and schizophrenia; however, death is a rare outcome of poliovirus infection and may not be an accurate index of the onset or ending of an epidemic. The most recent study [6], using a large Finnish sample with accurate psychiatric and poliomyelitis incidence data, found a weak but significant association between poliomyelitis and births five months later of individuals who developed schizophrenia later in life.
To date, however, no study has examined links between poliomyelitis epidemics and schizophrenia birth rates in the Southern Hemisphere. Given that the epidemiological profile of schizophrenia may be different in the Southern Hemisphere, for instance in seasonality of birth [7], and season of first admission [8], such a study is relevant. The specificity of the association between poliomyelitis epidemics and schizophrenia versus affective psychosis also warrants examination. Using a large dataset from Queensland, Australia, the aim of this study was to test whether there was any association between prenatal exposure to poliovirus epidemics and the later development of either schizophrenia or affective psychosis.
Method
All Australian cases born between January 1930 and December 1964 and first registered between 1972 and 1991 with an ICD8 or 9 diagnosis of schizophrenia (ICD295.x; n = 6078) or affective psychosis (ICD296.x; n = 3707), were extracted from the Queensland Mental Health Statistics System, a state-wide public psychiatric register.
For the same period, monthly counts of cases of poliomyelitis were obtained from the Annual Reports of Queensland Health Department. Similarly information on background population numbers and monthly totals of general population births for Queensland were obtained from the Australian Bureau of Statistics. Using these data, we calculated rates per 10 000 background population for poliomyelitis and rates per 10 000 general population births for the psychoses.
The eight identified poliomyelitis epidemics peaked in either summer or early autumn: February 1932, March 1938, January 1941, December 1945, April 1951, March 1953, March 1955 and January 1962. During these eight epidemics, the mean poliomyelitis cases per month was 36.15 (SD = 36.99), compared with 2.32 (SD = 5.21) in nonepidemic months.
A ‘poliomyelitis window’ was constructed for the months surrounding the eight peak poliomyelitis rates. To supply a simple model for the extent of the epidemic, poliomyelitis was deemed to be active within this window. Thus, based on 24 months surrounding each of the epidemic peaks, the ratio of the psychosis birth rates within the polio epidemic window and the birth rates in remaining nonepidemic months provides an estimate of the relative risk of psychosis attributable to the poliomyelitis epidemic.
We examined three windows of different lengths – namely 6, 8 and 10 months. The latter covers possible prenatal exposures from conception to 10 months postnatal and compares epidemic months with a combination of the 7 months preceding and 7 months following the epidemic window, thus controlling for seasonality. It also includes the fifth month following the epidemic, which was found to be associated with polio in the Finnish study.
An empirically weighted regression was used, in which the pooled psychosis birth rates R h are regressed on X h, h = − 12,…, 12, where R h is the mean of eight corresponding rates over the period 1930–1964. The reciprocal of the sample variance of R h provides the weights, and X h is an indicator variable, equal to unity within a poliomyelitis window, and zero elsewhere. These analyses were performed on all subjects, and repeated for males and females separately, using PROC IML in SAS version 7 [9].
Power analysis suggested that the number of patients with schizophrenia in this sample would have sufficient power (82%) to detect (at p < 0.05) a relative risk as low as 1.175. For affective psychosis, the study had sufficient power (95%) to detect (at p < 0.05) a relative risk as low as 1.30.
Results
Taken over the period of the window, there were no statistically significant associations between psychosis rates and poliomyelitis epidemics.
Figure 1 displays the pooled rates of schizophrenia and affective psychosis surrounding the poliomyelitis peaks for the 8-month window – which showed the largest relative risk. Here the risk for schizophrenia was estimated to be 1.04 (95% CI 0.93, 1.16) while for affective psychosis it was 0.99 (95% CI 0.85, 1.15).
Using an 8-month window, pooled rates for schizophrenia births and affective psychosis births (per 10 000 births), and poliomyelitis rate (per 10 000 population) around the peaks of eight polio epidemics (1930–1964).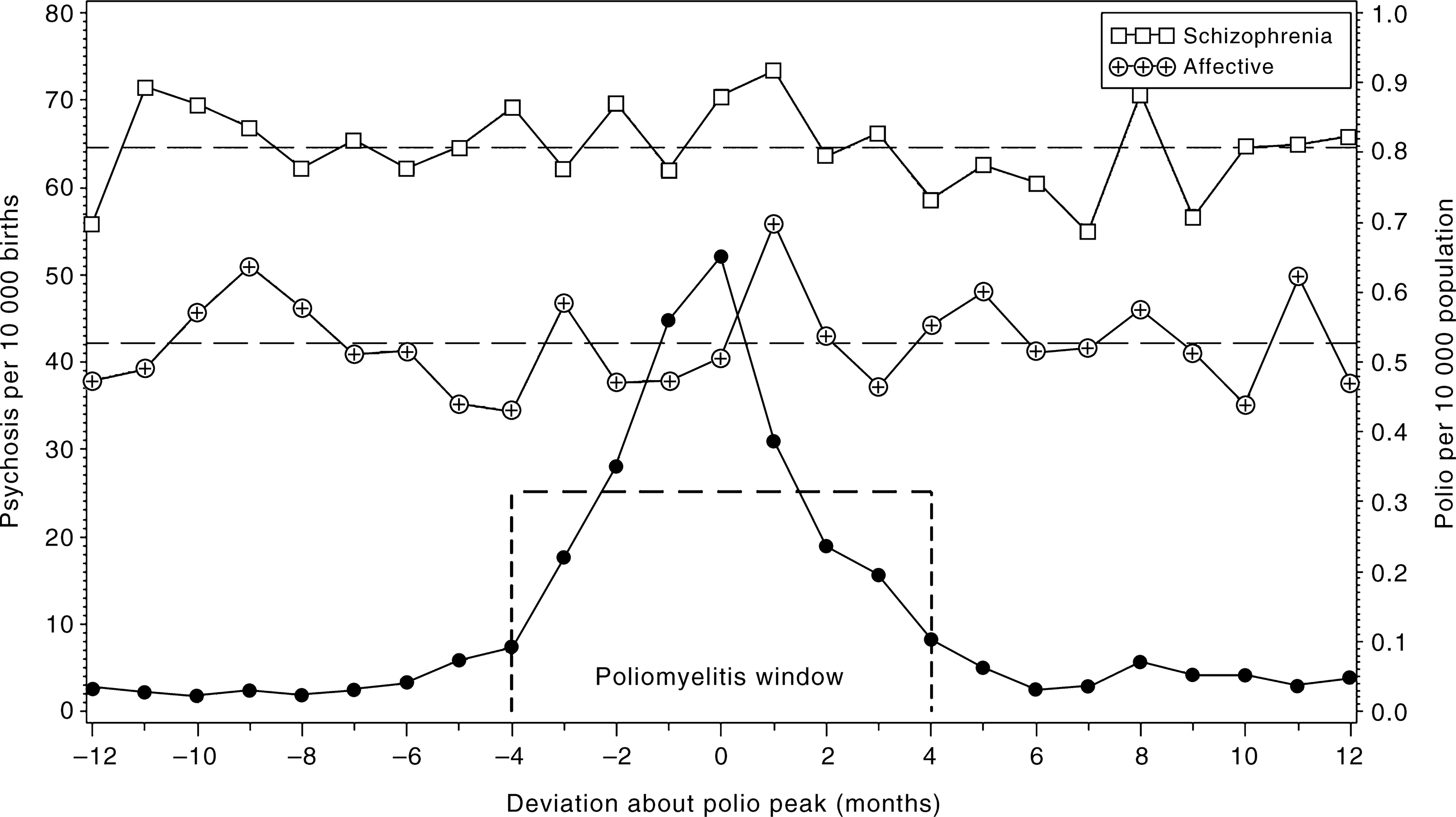
No significant associations were found when the poliomyelitis window was adjusted to 6 or 10 months, nor when any of the analyses were conducted for males and females separately (data not shown).
Discussion
Our study found no significant association between prenatal exposure to poliomyelitis epidemics and increased rates of schizophrenia and affective psychosis. When the same analysis was conducted on males and females separately, the results did not change.
One strength of the study was that we included statewide data, which allowed us to calculate rates for both the psychiatric disorders and poliomyelitis. During the study period, Queensland experienced eight clearly demarcated poliomyelitis epidemics; however, given this was an ecological analysis, we could not determine the exposure status of mothers of those who developed a psychosis. The register was designed primarily for administrative purposes and thus the reliability of diagnoses may be suboptimal, and may overestimate case birth rates (because the numerator includes cases born in other Australian states, whereas the denominator covers only Queensland births and between-state migration is unlikely to be systematically linked to poliomyelitis epidemics). Nevertheless, any true association between poliomyelitis epidemics and psychosis birth rates would be more difficult to detect. In addition, our study did not have sufficient power to detect the small effect size found for schizophrenia in the Finnish study (i.e. a relative risk of 1.05, 95% CI 1.00–1.11). To exclude a true but weak effect of polio, larger sample sizes and/or meta-analysis would be required. This may be important given that exposures associated with small effect sizes, if prevalent, may account for sizeable population attributable risks.
While we found no association between prenatal exposure to poliomyelitis epidemics and increased risk of schizophrenia, an association has been found in some other sites. It is possible that poliovirus epidemics may act as proxy markers of other risk-modifying factors (for example, staying indoors may result in hypovitaminosis D [10], or transmission of viruses may differ in warm versus cold climates). These other risk factors associated with poliomyelitis epidemics may not be uniformly distributed (in timing, place and/or strength). There has been a relative poverty of novel non-genetic risk factors for psychoses. We believe that poliovirus warrants further study, and that inconsistencies between sites may provide fertile ground for the refinement of candidate riskmodifying factors of schizophrenia.
Footnotes
Acknowledgements
The Stanley Foundation supported this project.