
Abstract
Subtle deviations in various developmental trajectories during childhood and adolescence can foreshadow the later development of later psychotic disorders [1]. The evidence, however, from prospective birth cohort studies linking measures related to physical growth and later psychosis has been less consistent.
Low birthweight or being small for gestational age (SGA) has been associated with an increased risk of schizophrenia in some birth cohort studies [2–4], but not in others [5–7]. A Finnish study found that schizophrenia was associated with small size at birth (shortness together with low birthweight and placental weight) and lower late-pregnancy maternal body mass index (BMI) [8]. There is mixed evidence over whether diminished head circumference (HC) presents a risk for schizophrenia [9]. Two case–control studies that examined HC at birth produced conflicting results [10, 11], while a prospective birth cohort study found no association between HC at age 7 and later schizophrenia [12]. There is also some evidence that dysmorphic growth in terms of disproportionate HC/birth length may increase the risk of later schizophrenia [10]. While birthweight has been examined in many studies, relatively few population-based studies have examined growth in childhood and adolescence and risk of later psychosis. Again, the evidence is mixed. An association between low childhood BMI and adult schizophrenia was found by Wahlbeck et al. [8] but not by Jones et al. [5]. Neither of the two British birth cohorts found a significant association between childhood height and weight and later schizophrenia [5, 12]. A number of population-based studies have identified that low adolescent BMI and/or reduced height was associated with later schizophrenia [13–16]. The evidence for any association between adult body build and schizophrenia is also mixed [8, 13, 17].
When examining the association between growth and later adverse health outcomes, it is important to examine within-individual trajectories as well as group means. For example, low-birthweight individuals may catch up during infancy and this altered trajectory may have consequences for later health [18, 19]. With respect to later psychosis, once again, the evidence from prospective birth cohort studies is mixed. A US-based study found that the growth trajectory from birth to age 9 was slower during early life for female subjects but not for male subjects who went on to develop schizophrenia spectrum disorder [19]. In contrast, a Finnish study found no association between catch-up growth and schizophrenia [20].
Apart from height and weight, pubertal maturation can also provide insights into physical growth and risk of later psychosis. Cross-sectional studies have found equivocal evidence regarding age at menarche and onset of schizophrenia. A negative association between age at menarche and age at schizophrenia or psychosis onset has been found [21, 22]. This effect, however, has not been supported by other studies [23, 24]. With respect to prospective birth cohort studies, the two that have reported on measures related to the timing of puberty found no association with later schizophrenia [5, 12].
We had the opportunity to examine these issues based on an Australian, population-based prospective birth cohort. To date, the prospective birth cohort studies that have examined physical growth and later psychosis have relied on linkage to registers to identify potential cases. Thus, clinical outcomes have been based on treated samples, rather than more representative community-based samples. The present study was able to explore a population-based sample of individuals who screened positive for non-affective psychosis (SP-NAP). A recent study of this cohort found that disturbed behaviour at 5 years for male subjects and at 14 years for both male and female subjects predicted SP-NAP [25]. Thus, it remains to be seen if indices of growth and maturational disturbances also predict SP-NAP in this cohort. Based on the previous literature, we predicted that cohort members who showed signs of prenatal growth restriction (such as SGA) would be associated with adult SP-NAP. Concerning within-individual growth trajectory, we predicted that those cohort members who (i) showed evidence of prenatal growth restriction and poor growth measures from birth through to year 21, or (ii) were short at birth and then showed catch-up growth at years 5 or 14, would be at increased risk of SP-NAP compared to their peers. Given that we have previously found gender differences in behaviour in this cohort, and other studies have reported gender differences in growth and development, we decided to examine the variables of interest in male and female subjects separately. Finally, concerning pubertal development and age at menarche, we predicted that these measures would not be associated with risk of SP-NAP.
Methods
The Mater–University Study of Pregnancy and its outcomes (MUSP) is a prospective study of 7223 women and their offspring who received antenatal care at a major public hospital in Brisbane, Australia between 1981 and 1984. The cohort, which has been followed up at various ages, has been used to assess the precursors of a broad range of physical and mental health outcomes; full details of the MUSP study design, sampling strategy, attrition, and follow-up sample characteristics are available elsewhere [26].
At the 21 year follow up, 2575 of the child cohort members undertook the lifetime version of the Composite International Diagnostic Interview (CIDI) computerized version [27]. All cohort members also completed a health outcomes checklist, which included the following item ‘Have you ever been told by a doctor that you have schizophrenia?’. For the current study we defined caseness as: (i) meeting the criteria for CIDI-generated DSM-IV [28] schizophrenia, brief psychosis, delusional disorder, or schizophreniform disorder; or (ii) for the 1226 not undertaking the CIDI, receiving a past medical diagnosis of schizophrenia as reported on the checklist. Henceforth, we refer to these individuals as having ‘screen-positive non-affective psychosis’ (SP-NAP).
Measures of physical growth and other data, such as parental body build, were obtained medical records and from the mothers or cohort members at various stages. Cohort members’ height and weight were record at birth and at the 5, 14 and 21 year follow ups. These measures allowed the BMI and ponderal index to be calculated. HC was measured at birth and at the 5 year follow up. To estimate pre- and post-natal growth proportionality at birth, indices were constructed by dividing birth HC by body length. To examine whether there were case/non-case differences in growth over time we also constructed rate-of-change indices between time points (i.e. birth and years 5, 14 and 21 follow up). Pubertal development was assessed at age 14 using the widely used Tanner's scale [29], together with self-reported age of menarche for female subjects obtained at years 14 and 21 follow up.
Details on variables that may modify growth and development were also examined, such as length of gestation, parental height and weight (as measured at the birth of the cohort members), maternal smoking during pregnancy, breast-feeding status, various sociodemographic measures, and age at assessment (cohort births occurred over a 3 year period and follow-up assessments occurred at one time point, thus actual ages at follow up varied slightly). Unexpectedly, we found that (i) fathers of cohort members who developed SP-NAP were taller than fathers of those who did not (179.09 vs 176.53 cm, respectively, p < 0.03); (ii) there was a trend level association between shorter gestation in the SP-NAP group (38.60 weeks vs 39.38 weeks, respectively, p < 0.07); and (iii) actual age at year 21 follow up was associated with SP-NAP for female subjects (p < 0.04). These variables were included in the statistical models as covariates; the other potentially confounding variables were not associated with SP-NAP and not included in the modelling.
For the logistic regression analyses some continuous variables were transformed into tertiles (based on the non-SP-NAP subjects), following previous research [16, 30]. Gestational length was dichotomized (<38 weeks vs ≥38 weeks). To allow for the impact of length of gestation on birthweight, we constructed an index of SGA, that is, being at or below the lowest 10th percentile (based on the non-SP-NAP distribution); this was then corrected for length of gestation. To examine whether there were case/non-case differences in growth over time we constructed indices of rate of change between time points (e.g. weight at age 14 minus weight at age 5 divided by interval in months). For the pubertal analysis, the Tanner scales (the six-level breast/genital and pubic hair development) were dichotomized into ‘mature’ and ‘immature’ (based on the non-case distribution). Age at menarche for female subjects was obtained at years 14 and 21 follow up and reported as tertiles.
We used maximum-likelihood logistic regression to examine the association between the indices of physical development at various ages and SP-NAP at age 21. Because we hypothesized sex differences in growth and development, apart from examining the total group, we also (i) tested specifically for sex differences (predictor variable×sex interaction), and (ii) repeated our analyses for male and female subjects separately. Models were adjusted for age at year 21 assessment, gestational age and paternal height. We also examined models which tested for (i) a linear effect; and (ii) differences in SP-NAP versus non-SP-NAP growth over time (using indices of rate of change between time points). Analyses were performed using the statistical package SAS (SAS Institute, Cary, NC, USA). Written informed consent was obtained from the mother at all data collection phases, and from the young adult at the 21 year follow up. Ethics approval for this study was obtained from the University of Queensland Ethics Committee.
Results
A total of 3801 members of the MUSP birth cohort completed the age 21 follow up assessment: 1806 (48%) were male. A total of 2575 (68%) completed the CIDI: of these, four were found to meet the DSM-IV criteria for schizophrenia, four for delusional disorder, 24 for brief psychotic disorder, and four for schizophreniform disorder, resulting in a total of 36 who screened positive for CIDI-based diagnosis of non-affective psychosis. Of the 1226 cohort members who did not complete the CIDI, 24 reported a past medical diagnosis of schizophrenia on the checklist. These respondents, together with the CIDI-diagnosed subjects, gave a total of 60 SP-NAP cases.
There were no significant associations between any of the predictor variables and SP-NAP for the total group or for male subjects separately. There were, however, several measures for which female subjects had a significant effect (see Table 1). At birth, female subjects who developed SP-NAP were significantly more likely to be longer than their female peers, with a trend association at age 5. Consistent with this, by age 21 female SP-NAP subjects were significantly less likely to be in the shortest tertile (i.e. they were taller than non-SP-NAP subjects). At birth, female SP-NAP subjects were also significantly more likely to have a larger HC. No male SP-NAP subjects had a large HC at birth, thus the odds ratio could not be calculated (but we note that the distribution of male cohort members was in the opposite direction to that for female subjects). There was no effect for SGA. There were also no differences between SP-NAP subjects and non-SP-NAP subjects in (i) the rate of growth over the various ages at assessment; and (ii) the derived measures of proportionality (data not shown). There was no significant association between the measures of pubertal development at age 14 years and later SP-NAP. There was no difference between SP-NAP subjects and non-SP-NAP subjects in either age at menarche or whether menses had commenced or not. None of the analyses identified significant linear trends across the levels. None of the analyses that tested for sex by predictor variables identified significant effects.
Subject characteristics (n = 3527)†
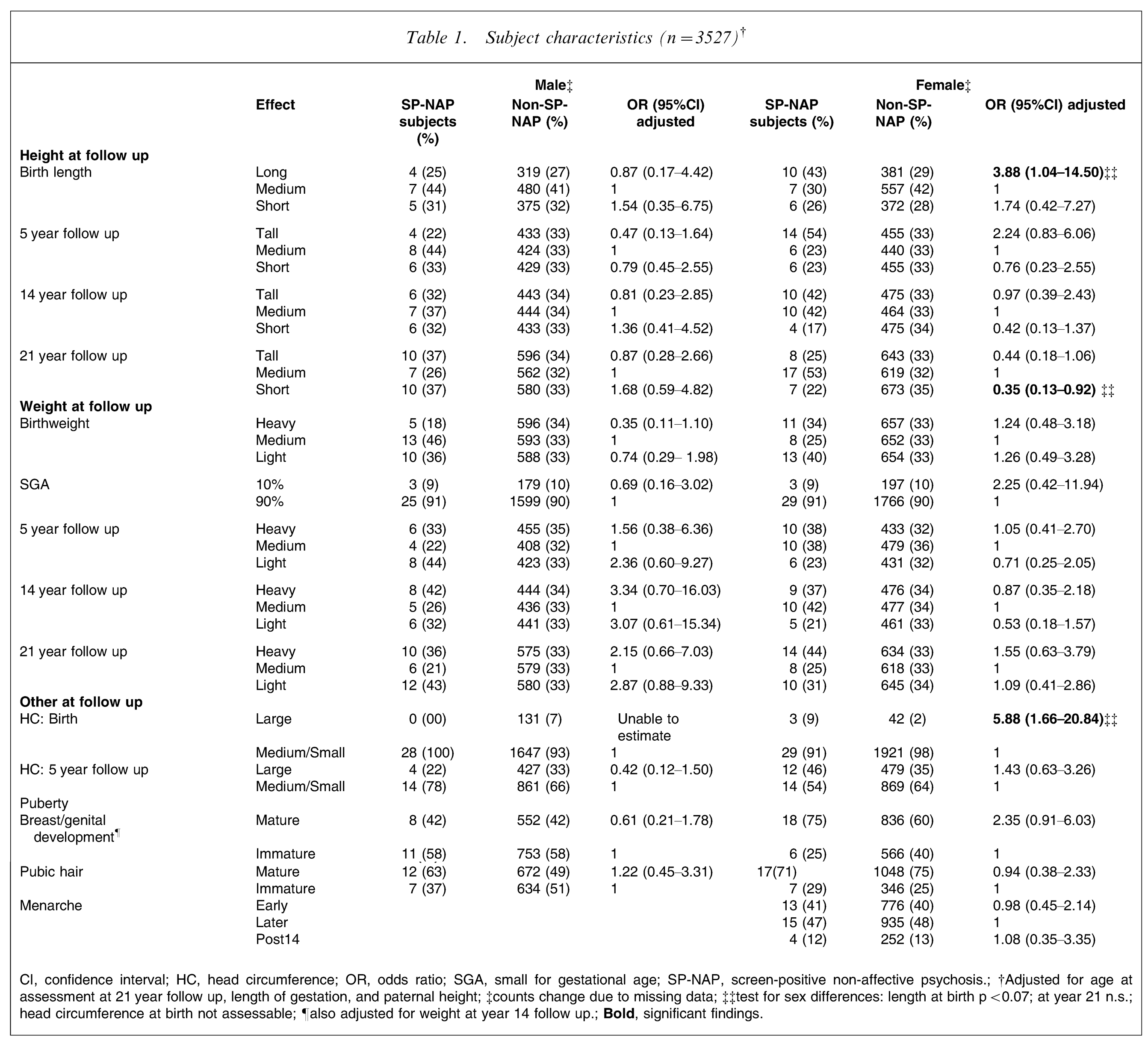
CI, confidence interval; HC, head circumference; OR, odds ratio; SGA, small for gestational age; SP-NAP, screen-positive non-affective psychosis.; †Adjusted for age at assessment at 21 year follow up, length of gestation, and paternal height; ‡counts change due to missing data; ‡‡test for sex differences: length at birth p < 0.07; at year 21 n.s.; head circumference at birth not assessable; ¶also adjusted for weight at year 14 follow up.;
When we restricted the SP-NAP subjects to those with a CIDI-generated diagnosis only (n = 36), the point estimate for the odds ratios generally changed little. The reduced sample size, however, led to confidence intervals becoming broader with no statistically significant associations.
Discussion
We have previously found emotional and behavioural antecedents in individuals from this birth cohort who were classified as SP-NAP as young adults – an effect especially strong for male subjects. There are no differences, however, in the physical growth trajectory or other growth indicates, such as SGA, for men. In contrast, women who are classified as SP-NAP as young adults are more likely to be longer and have a larger HC at birth, and are less likely to be short at age 21. Other indices of growth, however, showed no associations. Although the present definition of caseness was based on different criteria, the overall findings of the current study support the studies that report a lack of deviance in the growth trajectory of individuals who develop non-affective psychosis.
With respect to the findings in women, the present findings are opposite to those reported by (i) Gunnell et al., who found that birth length was inversely associated with schizophrenia [16]; and (ii) a high-risk study, which found that pre-schizophrenia girls were shorter at birth [31]. Although we found increased HC at birth, previous studies have either found no effect at birth [11] or at age 7 [12], or reduced HC at birth [10].
We did not find evidence of deviance or discontinuity in growth in pre-psychosis subjects: measures of rate of change across the developmental trajectory were similar for SP-NAP and non-SP-NAP subjects. Consistent with the recent Finnish study [20], this suggests that growth patterns were not characterized by catch-up growth.
As far as we are aware, the finding of an association between paternal physique and non-affective psychosis in offspring has not previously been reported. Thus, our post-hoc finding that taller fathers were associated with increased risk of SP-NAP should be interpreted with caution. Nevertheless, given the current interest in paternal risk factors [32] and the potential role of growth factors in the antecedents of schizophrenia [19], this finding is worthy of further hypothesis-driven research.
Although there was no significant association between pubertal development and SP-NAP, there was a trend level association between increased maturity on Tanner measures at age 14 years and increased risk of SP-NAP in female subjects. The present sample size may not have been large enough to detect a small effect size.
The present study has several caveats. While the MUSP cohort was subject to attrition, we found in our birth cohort review that the level of MUSP attrition at age 21 (47%) reflected the average attrition of other cohorts [1]. Although MUSP attrition was primarily due to lack of resources to track cohort members rather than refusal to participate, participants lost to follow up (LTFU) were more likely to be male, have younger mothers, come from lower income families and have at least one migrant parent [33]. If the associations we found were absent or in the opposite direction in those LTFU, then this would limit our interpretations. Although we cannot assess this directly, we consider the more likely result of attrition would be to make true associations more difficult to detect. We conducted multiple statistical tests, thus, although we provided directional hypotheses, some associations may be chance findings and require further study. Finally, SP-NAP as an outcome variable was not clinically validated. In population-based studies otherwise-well individuals may endorse psychosis-related items [34, 35]. SP-NAP subjects then may include individuals who score highly on psychosis-screening items, but who do not meet full clinical diagnostic criteria. We hope to explore this issue in future follow up of the cohort.
In conclusion the present study, based on a large, prospective, general population birth cohort, shows that, in general, male subjects who screen positive for non-affective psychosis as young adults follow normal growth trajectories. The data suggest that SP-NAP female subjects display an altered skeletal growth trajectory with significant differences at birth and year 21. These physical growth effects are in contrast to our recent findings from the same cohort that demonstrated pre-morbid continuity in childhood psychopathology in boys, and adolescent psychosis-like experiences for both sexes [25]. This finding of stronger effects of behavioural rather physical growth antecedents calls for further research. Other results of the study have also generated hypotheses suitable for further study (e.g. fathers’ height and risk of SP-NAP). Understanding how developmental pathways lead to adverse mental health outcomes may provide important clues to the pathogenesis of these disorders.