
Abstract
Objective:
Stimulant abuse and dependence often complicate the care of people with psychotic disorders. This study systematically reviews the prevalence estimates reported for stimulant abuse and dependence in people with psychotic disorders, and examines personal, clinical, regional and methodological factors which explain variation in these rates.
Methods:
PsychINFO, EMBASE and MEDLINE (1946–2013) were searched systematically for studies reporting on stimulant drug use disorders in representative samples of people with psychotic disorders. Random effects models estimated the pooled rate of a stimulant use disorder, defined to include stimulant abuse and stimulant dependence. Study characteristics associated with heterogeneity in rates of stimulant use disorder were examined by subgroup analyses for categorical variables, by meta-regression for continuous independent variables and by multiple meta-regression.
Results:
Sixty-four studies provided 68 estimates of lifetime or recent stimulant use disorders in 22,500 people with psychosis. The pooled rate of stimulant use disorder was 8.9% (95% CI 7.4%, 10.5%). Higher rates of stimulant use disorders were reported in studies of affective psychosis, studies from inpatient settings, studies from the USA and Australia, and studies with higher rates of cannabis disorder; in multiple meta-regression analysis these factors explained 68% of between-study variance. Rates of stimulant use disorder were stable over time, and unrelated to age, sex, stage of psychosis, type of stimulant drug or study methodology factors.
Conclusions:
Reported rates of stimulant use disorder in people with psychosis are much higher than in the general population but vary widely and are associated with regional, service setting and clinical differences between studies. It is likely that stimulants contribute to the overall burden of psychosis, and that social and environmental factors combine with drug and illness-related factors to influence stimulant use in psychosis.
Introduction
Amphetamines, cocaine and other stimulants are the most widely used illicit drugs after cannabis in developed countries (United Nations Office on Drugs and Crime, 2011). They are most commonly used by males in their late teens and early 20s, who are also the group most at risk for the development of psychotic disorders (Adlaf et al., 2005; Degenhardt et al., 2007a; Durell et al., 2008; Substance Use and Mental Health Services Administration, 2010; Wilkins et al., 2006). In 2007, around 3% of Australians, including more than 8% of men aged 16–29 years, met the criteria for a lifetime stimulant use disorder (Sara et al., 2011a).
Stimulants may have harmful effects across the spectrum of psychotic disorders and, along with cannabis, may play a causal role in some episodes of psychosis (Sara, 2012). Many regular stimulant users report transient and dose-dependent psychotic symptoms (McKetin et al., 2006). Stimulants can precipitate brief syndromes of drug-induced psychosis (Bramness et al., 2012; Crebbin et al., 2009), sometimes diagnosed as ‘methamphetamine psychosis’ (Kittirattanapaiboon et al., 2010; Yui et al., 2000). Stimulant exposure can worsen existing psychotic symptoms or precipitate relapse among people with established psychotic disorders such as schizophrenia (Curran et al., 2004). The effects of stimulants on psychosis are more common in people with patterns of severe or dependent stimulant use (Chen et al., 2003; McKetin et al., 2013), and stimulants such as methamphetamine may be more potent than cannabis in precipitating psychotic symptoms (McKetin et al., 2013). Therefore, knowing the rate of severe or dependent stimulant use in people with psychosis may help in understanding whether stimulant drugs contribute significantly to the overall burden of psychosis.
Studies of people with psychosis have reported rates of stimulant use disorder which range from below 4% (Compton et al., 2005; Hambrecht and Häfner, 1996; Martins and Gorelick, 2011) to more than 30% (Gearon and Bellack, 2000; Sevy et al., 1990). In a population cohort of people with a diagnosis of schizophrenia in New South Wales, 14% also had a diagnosis of a stimulant use disorder (Sara et al., 2014b). This wide variation between studies may reflect differences in the personal, clinical or social characteristics of the people with psychosis who were included in the study. Delineating these factors would help in understanding which groups of people with psychosis may be at greater risk of stimulant-related harms. There are also significant regional differences in stimulant use in the general population (Agar and Reisinger, 2004; Degenhardt et al., 2008; United Nations Office on Drugs and Crime, 2011). If stimulants contribute to the overall burden of psychosis, then stimulant use disorders in people with psychosis may be more common in regions where stimulant use is also more common in the general population. Rates of stimulant use may also be influenced by the subtype or stage of psychosis: several studies of people with a first episode of schizophrenia-spectrum or affective psychosis have reported rates of stimulant use or dependence between 15% and 30% (Hides et al., 2006; Mauri et al., 2006; Rabinowitz et al., 1998; Ruiz-Veguilla et al., 2009; Sara et al., 2013; Wade et al., 2005). Cannabis use often precedes or accompanies stimulant use (Degenhardt et al., 2009; Power et al., 2014) and cannabis disorders are one of the strongest predictors of later stimulant disorder (Degenhardt et al., 2007b). Therefore, in examining stimulant use disorders, it is also important to measure and control for cannabis use disorders.
The wide between-study variation in rates of stimulant use disorder in people with psychosis may also be due to methodological differences between studies: rates of stimulant use disorder are likely to be influenced by issues including the period examined (lifetime or recent stimulant use), the inclusion or exclusion of specific stimulant drugs (amphetamine, cocaine, ecstasy), or whether drug-induced psychoses were included or excluded.
The first aim of this study is to synthesise the results of primary research through meta-analysis in order to derive a pooled estimate and range for the rate of stimulant use disorder in people with psychosis. The second aim of this study is to identify whether between-study variation in the rate of stimulant use disorder is systematically influenced by personal, clinical or social factors, or whether this heterogeneity is better explained by methodological differences between studies.
Methods
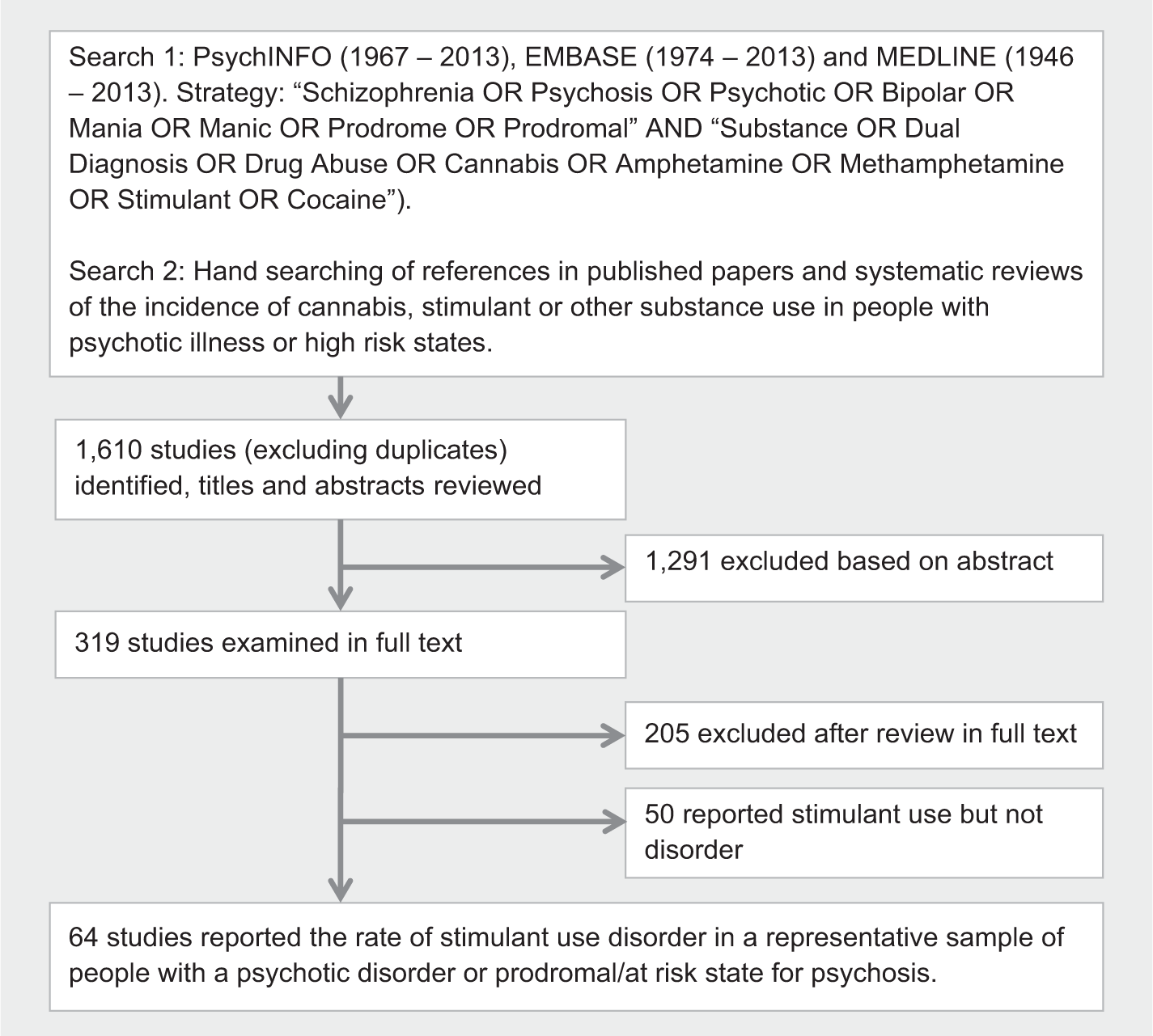
The methods conformed to the guidelines for Meta-analysis of Observational Studies in Epidemiology (Stroup et al., 2000). Figure 1 summarises the study selection method.
Search strategy.
Data sources
PsychINFO (1967–2013), EMBASE (1974–2013) and MEDLINE (1946–2013) were searched systematically for peer-reviewed English-language publications reporting rates of substance use in people with psychosis. To identify potential studies for examination in full text, titles, abstracts and keywords were searched for ‘Schizophrenia OR Psychosis OR Psychotic OR Bipolar OR Mania OR Manic OR Prodrome OR Prodromal’ AND ‘Substance OR Dual Diagnosis OR Drug Abuse OR Cannabis OR Amphetamine OR Methamphetamine OR Stimulant OR Cocaine’. The search strategy was broad, including any substance use disorder or cannabis disorder because rates of stimulant use disorder are often reported as incidental findings without mention of stimulants in the study’s title, keywords or abstract. The reference lists of identified studies and key literature reviews were hand-searched for further relevant studies.
Study selection and data extraction
Studies were included if they reported the recent or lifetime prevalence of stimulant use disorders in people with a diagnosed psychotic disorder. We accepted the diagnostic method used by the original study to identify and define stimulant use disorders and psychosis. Stimulant use disorders were defined to include Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD) categories of abuse and dependence, or, where these were not applied, levels of use characterised by the original study as ‘abuse’, ‘problem use’, ‘severe use’ or ‘harmful use’. Studies that reported stimulant use but did not report on rates of stimulant use disorder were excluded. Stimulants included unspecified stimulants or any specific stimulant drug identified through chemical or common names, including amphetamine, methamphetamine, ice, cocaine/crack, or ecstasy/MDMA. Psychoses included commonly used diagnostic categories (schizophrenia; schizoaffective disorder; affective psychosis; brief, atypical and drug-induced psychoses) or prodromal states.
Studies were included if they described rates of stimulant use disorder in representative clinical populations of people with psychosis, such as successive admissions or referrals from a defined catchment area or population. We excluded studies whose sampling framework rendered them non-representative or were likely to systematically influence the estimated prevalence of substance use disorders, such as clinical samples from dual diagnosis programmes, groups with only drug-related psychoses (such as ‘methamphetamine psychosis’), studies where groups were selected to obtain matched samples of people with and without substance comorbidity, and studies excluding people with substance use or dependence. Some studies had inclusion or exclusion criteria which were ambiguous or had the potential to distort prevalence estimates, such as referrals from clinical services to specialist treatment trials or imaging studies. If the study authors explicitly excluded people with substance use disorders, then these studies were excluded from this review. However, even where substance use disorders were not explicitly excluded, people with comorbid substance use disorders may have been less likely to be referred for these studies. Therefore, these studies were flagged for subgroup analysis rather than being excluded. Some representative samples allowed the inclusion of people with drug-induced psychoses within a larger multi-diagnostic sample: these studies were included in this review, but were flagged for subgroup analysis. In order to reduce the probability of chance results from very small samples, we defined an arbitrary minimum sample size of 15 people.
Two authors (GS, SM) selected the studies according to our inclusion criteria and extracted data independently. Multiple published studies based on a single clinical sample were examined for possible overlap; a single estimate was obtained from the most complete study reporting on those participants. One published conference abstract was identified which included all relevant data and was not otherwise reported: this was included in the review. Differences between raters were resolved by a joint examination of papers.
Definition of outcome and moderator variables
The primary outcome measure was the rate of stimulant use disorder in each study, expressed as the number of people with stimulant use disorder divided by the number of participants with psychosis in the study. Recency of drug use was classed as either ‘Recent’ (within the previous 12 months) or ‘Lifetime’ (greater than 12 months). Psychosis diagnoses were grouped into ‘Schizophrenia Spectrum’ (including schizophrenia, schizoaffective disorder and schizophreniform psychoses), ‘Affective Psychoses’ (bipolar disorder, psychotic depression), ‘Other Psychoses’ (brief, atypical and drug-induced psychotic disorders), and ‘Mixed’ (diagnostic subtype mixed or unspecified). A binary variable was constructed to indicate whether persons with substance-induced psychosis were included or excluded. Stage of psychosis was classed as ‘Prodromal’ (including prodromal, pre-psychotic, ultra-high risk or comparable states), ‘First Episode’ (first episode psychosis, first hospitalisation or first contact with a specialist early psychosis service), ‘Established illness’ (ongoing or chronic illness, diagnoses limited to schizophrenia only, contact with extended care or rehabilitation services) or ‘Mixed’ (stage of illness mixed or not specified). Where reported, the rate of recent or lifetime cannabis use disorder was recorded. Where a study collected data over several years, the year of collection was taken as the midpoint of the study period. Where year of collection was not reported, it was estimated by calculating the average time-lag between collection and publication for other studies in the review where these data were available, and subtracting this from the publication year. Country, location within country (urban, rural, mixed or unspecified) and service setting (inpatient, community, mixed or not specified) were recorded.
Data were extracted on study design and eight strength of reporting variables: the use of research interviews in (i) psychosis or (ii) substance disorder diagnosis; the use of standardised criteria (DSM or ICD) for (iii) psychosis or (iv) substance disorder; (v) the inclusion of biological assays (hair, urine or blood) in substance identification; (vi) missing demographic data for (sample, average age or sex distribution); (vii) the use of an estimated year of collection and (viii) type of recruitment method (random/representative or non-random). A composite ‘strength of reporting’ score was constructed by simple addition of these eight individual scores.
Meta-analysis
Analysis was conducted using Comprehensive Meta-Analysis (CMA) Version 3 (Biostat, Inc., Englewood, NJ, USA). An a priori choice of a random effects model was made for all analyses because of significant variation in study design and populations. Where studies reported stimulant rates for mutually exclusive diagnostic groups, these were treated as subgroups and examined separately.
Subgroup analyses
The contribution of categorical study characteristics (e.g. type of stimulant, stage of psychosis) to between-study heterogeneity was assessed using Q-value statistics. The contribution of continuous variables (e.g. age, sex, year of publication, cannabis rate) to between-study heterogeneity was examined using a random effects (restricted maximum likelihood) meta-regression model. Continuous and categorical variables with univariate significance were examined together using a random effects (restricted maximum likelihood) meta-regression model, with Knapp-Hartung distribution. Categorical variables were examined and, where required, collapsed into fewer categories to ensure that no variable had a Variance Inflation Factor (VIF) greater than 3.
The effect of variations in strength of reporting was measured by subgroup analysis for individual strength of reporting variables and after splitting studies at the median of the composite strength of reporting score. To investigate possible publication bias, a funnel (Egger’s) plot of the main effect was examined for interaction between stimulant rate and standard error. Duval and Tweedie’s ‘trim and fill’ method (Duval and Tweedie, 2000) was used to examine the effect on the pooled effect rate of hypothetical missing studies.
Results
Search results
The search strategy identified 1610 potentially relevant citations: 1291 were excluded following abstract review and 255 were excluded after review in full text (Figure 1). The 64 remaining studies had a combined sample size of 22,500 people with psychosis (per sample mean 331; SD 1195; range 40–9919). They provided 68 estimates of stimulant use disorder rates, since some studies included estimates for more than one diagnostic group. Differences between raters were resolved for rates of stimulant use disorder (20 studies) and other study details (six studies). Summary details and citations for all included studies are provided in Supplementary Table 1.
Meta-analysis of studies reporting stimulant use disorder
The pooled rate of recent or lifetime stimulant use disorder was 8.9% (95% confidence interval (CI) 7.4%, 10.5%, median 8.5%, interquartile range 4.0–15.9%). Between-study heterogeneity was assessed as high (I2 = 91.0%). The study with the lowest reported rate of stimulant use disorders (0.5%) described recent (12-month) substance abuse in 475 medication-free young people referred to an early psychosis service in Denmark (Petersen et al., 2007). The highest rate was reported by a study examining 67 people attending a psychiatry outpatient service in an inner city mental health service in Baltimore, USA (Gearon and Bellack, 2000); 37.3% of that group had a 12-month diagnosis of cocaine abuse or dependence.
Test of possible publication bias
Examination of the funnel plot showed asymmetry (Figure 2). The trim and fill method identified and removed 10 studies, producing a revised pooled estimate of 10.5% (95% CI 8.9%, 12.4%).
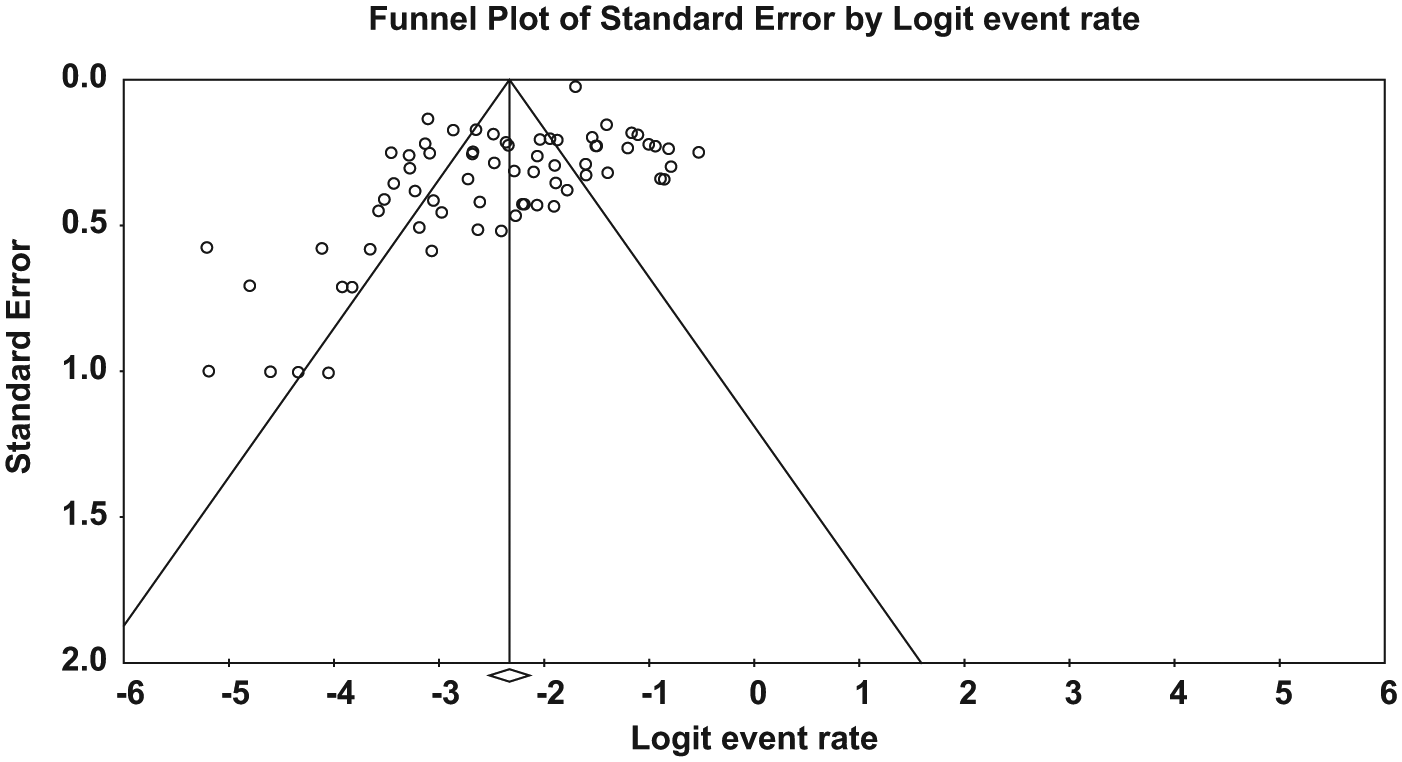
Funnel plot of standard error by logit event rate.
Subgroup analyses
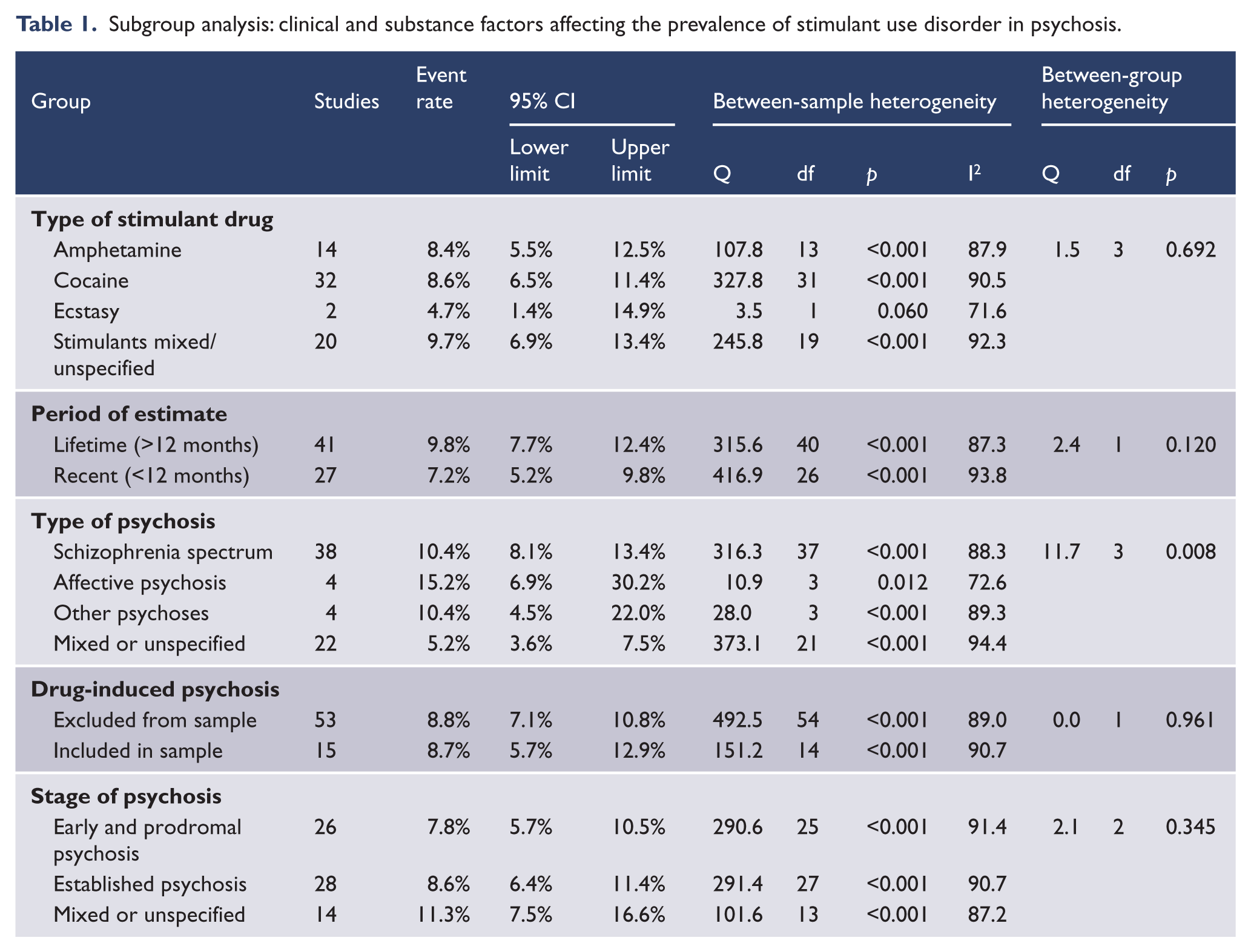
Subgroup analyses of clinical study characteristics are summarised in Table 1. The highest rates of recent or lifetime stimulant use disorder were reported in studies which examined affective psychosis (Miller and Tanenbaum, 1989; Mueser et al., 1992; Rabinowitz et al., 1998; Strakowski et al., 1996), having a pooled estimate of 15.2% (95% CI 6.9%, 30.2%). Studies of people with schizophrenia also reported higher rates of stimulant use disorder than studies of people with mixed or unspecified psychosis diagnoses. The pooled estimate of stimulant use disorder was non-significantly higher in studies examining lifetime rather than recent periods. The inclusion or exclusion of drug-induced psychosis, the stage of psychosis or the type of stimulant drug did not contribute to between-study heterogeneity.
Subgroup analysis: clinical and substance factors affecting the prevalence of stimulant use disorder in psychosis.
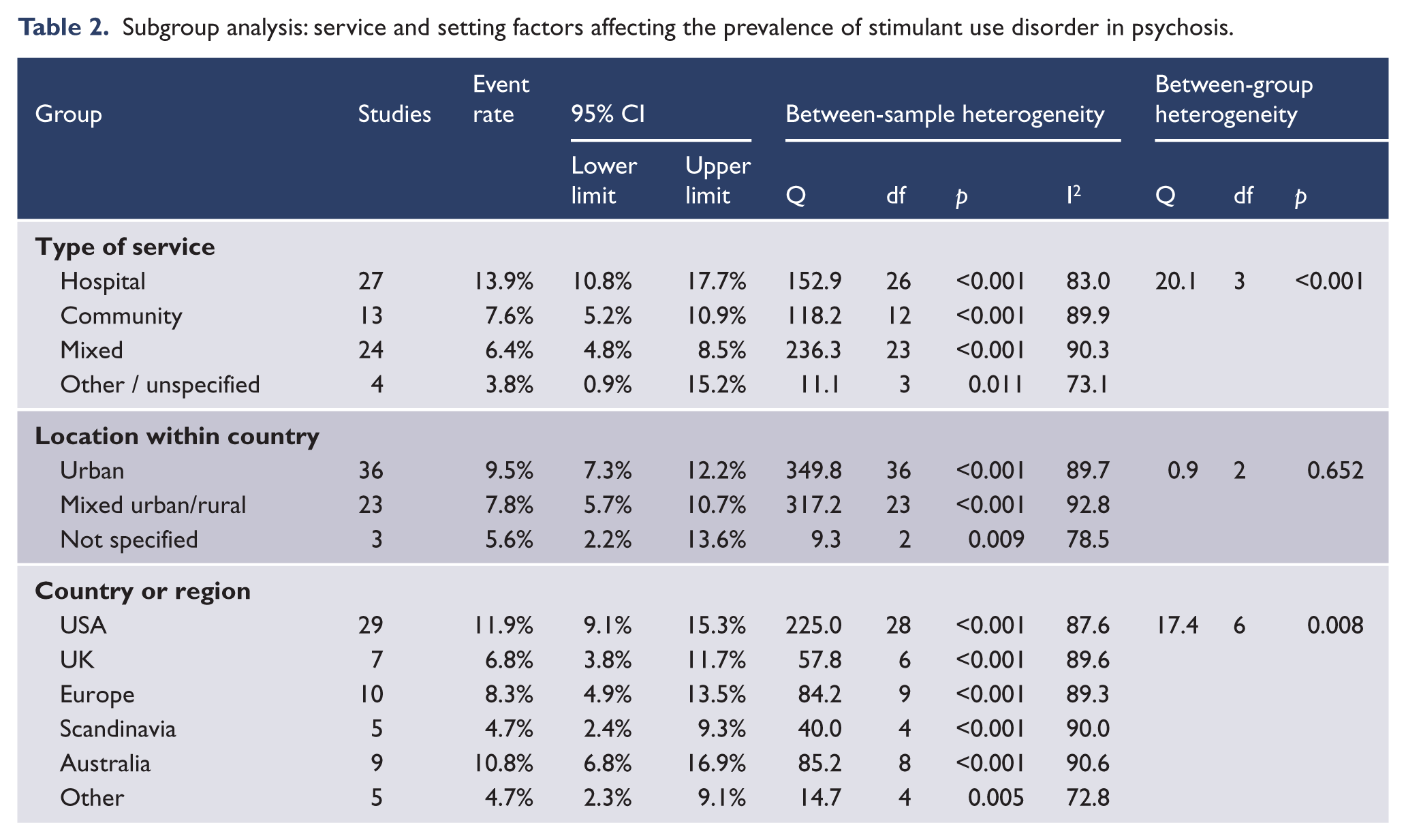
The influence of service and setting factors is summarised in Table 2. Higher rates of stimulant use disorder were reported in studies from hospital settings than in studies from community or mixed settings. There were significant regional or national differences, with the highest rates of stimulant use disorder being reported by studies from the USA and Australia, and lower rates reported by studies from western and southern Europe, Scandinavia, the UK and Ireland. There were differences between regions in the type of stimulant drug examined: most studies from the USA (19 of 29 studies) reported cocaine use disorders, UK studies reported a mix of amphetamine (three studies) and ecstasy use disorders (two studies), European studies reported cocaine (seven studies) or unspecified stimulant use disorders (five studies). Australian studies reported amphetamine/methamphetamine disorders (five studies) or unspecified stimulant disorders (four studies).
Subgroup analysis: service and setting factors affecting the prevalence of stimulant use disorder in psychosis.
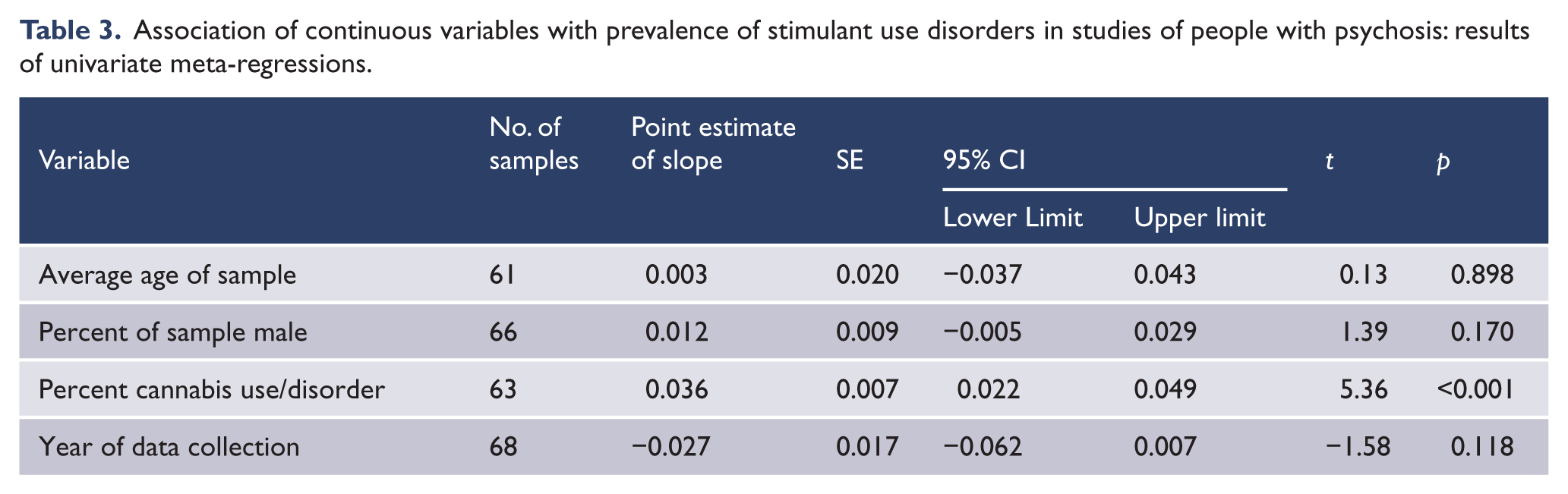
Meta-regression was used to examine whether individual continuous variables predicted differences between studies in the reported rate of stimulant use disorder (Table 3). Higher rates of stimulant use disorder were associated with higher rates of cannabis use disorder. Stimulant use disorder rates were not related to the average age or proportion of males in study samples. There was no significant change in stimulant use disorder rates over the period covered by the studies, from 1971 (McLellan and Druley, 1977) to 2009 (Sara et al., 2013).
Association of continuous variables with prevalence of stimulant use disorders in studies of people with psychosis: results of univariate meta-regressions.
Study methodology variables had little impact on estimated stimulant use disorder rates (Table 4). Studies with missing demographic (age or sex) data reported higher rates of substance use disorder. Studies which used biological assays to define recent substance use had a higher pooled estimate of stimulant use disorder rates than studies which did not use assays. Differing rates of stimulant use were not explained by whether studies used operational criteria or research interviews for defining psychosis or stimulant use disorder, or by a lower composite strength of reporting score.
Subgroup analysis: study methodology factors affecting the prevalence of stimulant use and disorder in psychosis.
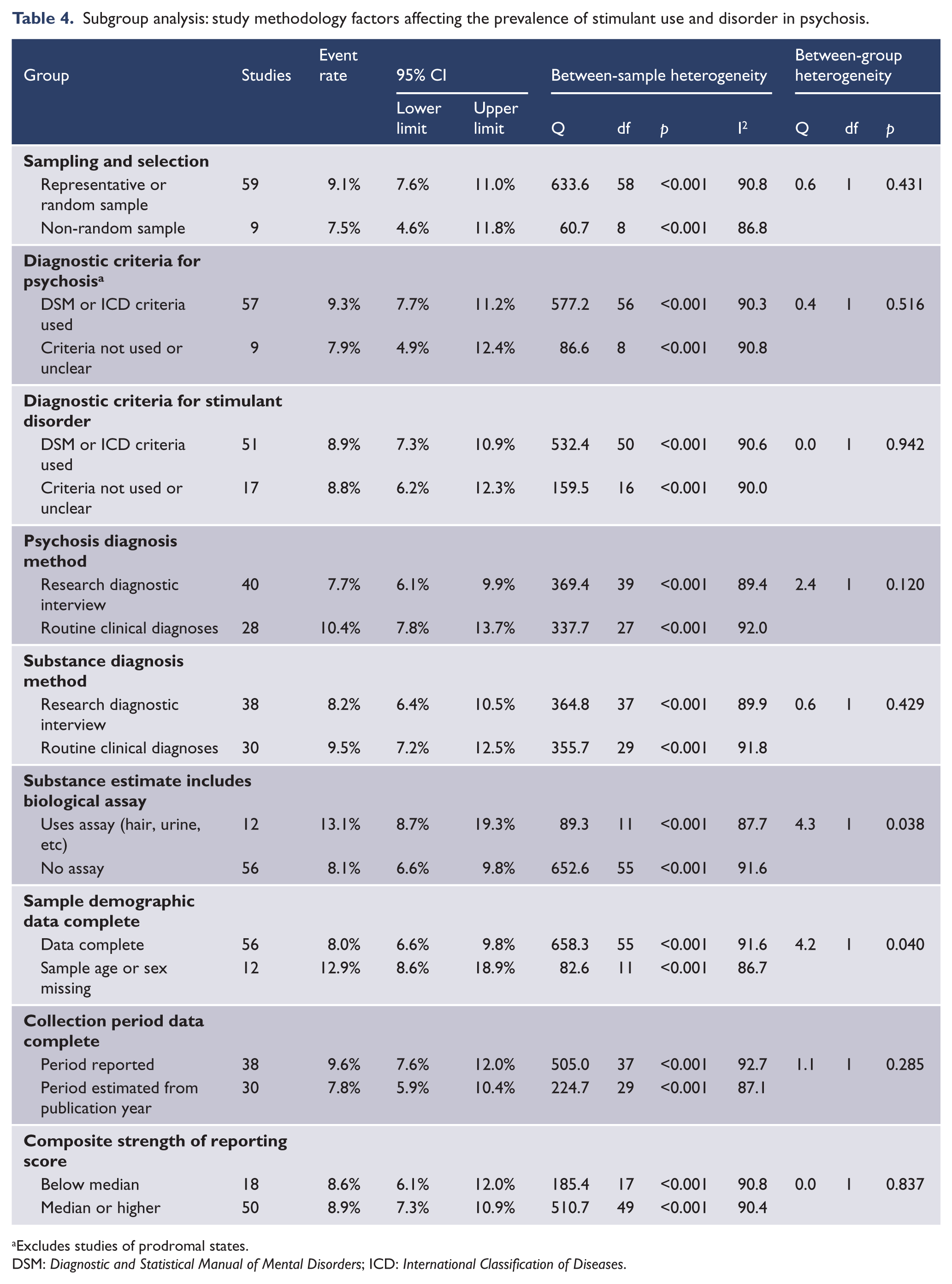
Excludes studies of prodromal states.
DSM: Diagnostic and Statistical Manual of Mental Disorders; ICD: International Classification of Diseases.
Multiple meta-regression
Significant univariate predictors of between-study heterogeneity were examined by multiple meta-regression (Table 5). To avoid unacceptable inflation of variance, two categorical variables (region, service setting) were collapsed to a smaller number of categories. Five studies (8%) had no data for rates of cannabis use and were excluded from this analysis. The rate of cannabis use disorders was the strongest predictor of stimulant use disorder rates, accounting for 43% of between-study variance. After controlling for cannabis use disorders, the period of observation (lifetime or 12-month) and the type of psychosis diagnosis did not contribute to between-study heterogeneity. Significant differences between regions remained in the multivariate model. Higher rates of stimulant use disorder were reported in studies from the USA and Australia. The combined model explained 67% of between-study variance (goodness-of-fit: tau2 = 0.8646, I2 = 91.37%, Q = 718.81, df = 62, p < 0.0001).
Multiple meta-regression: predictors of variation in the rate of stimulant use disorder in studies of people with psychosis.
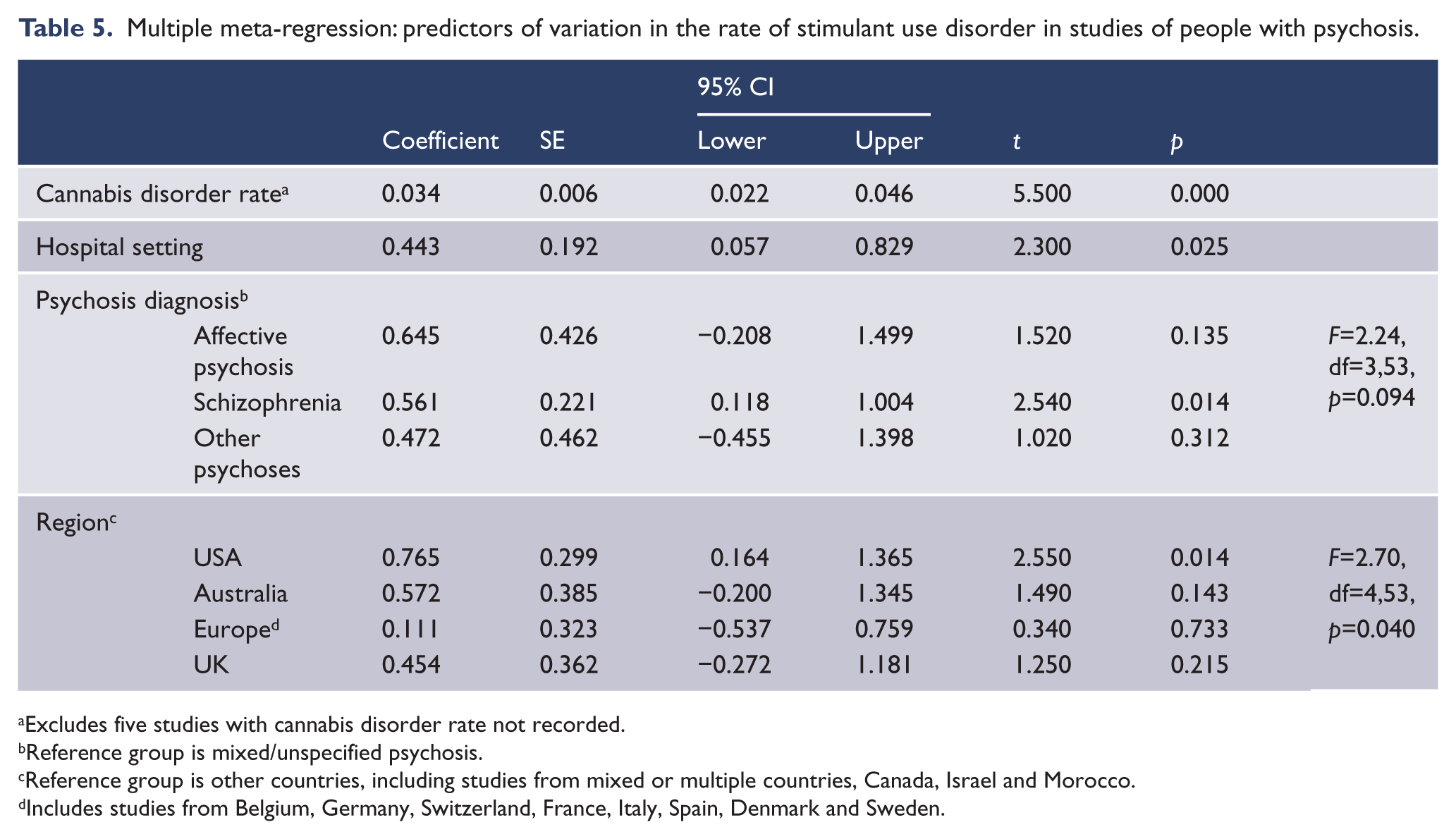
Excludes five studies with cannabis disorder rate not recorded.
Reference group is mixed/unspecified psychosis.
Reference group is other countries, including studies from mixed or multiple countries, Canada, Israel and Morocco.
Includes studies from Belgium, Germany, Switzerland, France, Italy, Spain, Denmark and Sweden.
Discussion
The first aim of this study was to estimate the rate and range of stimulant use disorders in people with psychosis. We found a pooled estimate (including recent and lifetime disorders) of 8.9% (95% CI 7.4%, 10.5%). Estimates varied widely between studies, and factors contributing to this variation are discussed below. The overall rate of stimulant use disorders in people with psychosis was substantially higher than estimated rates in the general population. The Global Burden of Disease Study estimated the 12-month prevalence of amphetamine or cocaine use in the general population to be 0.3–1.3% (Degenhardt and Hall, 2012), and the point prevalence of stimulant dependence to be 0.10–0.25% (Degenhardt et al., 2014). The current study cannot directly demonstrate the effect of stimulants; however, there is substantial evidence that stimulants may precipitate or worsen psychotic symptoms (Curran et al., 2004; Hermens et al., 2009).The high prevalence of stimulant use in people with psychosis therefore suggests that stimulants may make a significant contribution to the overall burden of psychosis.
The second aim of this study was to examine whether between-study variation in the rate of stimulant use disorder reflected factors that may be relevant to clinical care or health service planning, or was merely due to methodological differences between studies. There was very wide variation in rates of stimulant use disorder in people with psychosis: estimates ranged from 0.5% to 37.3%, with an interquartile range of 4.0–15.9%. We found that in a multiple meta-regression model, a combination of clinical and setting factors together accounted for nearly 70% of observed variation. Higher rates of stimulant use disorders were reported in studies with higher rates of cannabis disorder and studies from the USA and Australia. In univariate analyses, higher rates were also reported in studies of affective psychosis and from inpatient settings. Studies which included biological assays in the diagnosis of substance disorders reported higher rates of stimulant use or disorder, but other study methodology factors such as the period examined (lifetime or recent), the inclusion or exclusion of drug-induced psychosis or the use of structured diagnostic interviews had little impact on reported rates of stimulant use disorder.
Cannabis use disorders were the strongest correlate of the prevalence of stimulant use disorders. A meta-analysis cannot examine whether cannabis and stimulant disorders co-exist in the same individuals, but evidence from many other sources demonstrates such overlap. In the Australian population, 73% of people with lifetime stimulant use disorders also had lifetime cannabis use disorders (Sara et al., 2012). In clinical studies, most people with psychosis who used stimulants also used cannabis (Degenhardt et al., 2010; Power et al., 2014; Sara et al., 2014b). This is clinically significant because stimulants and cannabis may act synergistically in worsening psychotic symptoms (Paparelli et al., 2011).
Australian clinicians have expressed concern that stimulant abuse has contributed to increased demand for acute mental health services (Australian Senate Select Committee on Mental Health, 2006). We found that after controlling for differences in diagnostic mix and service setting, rates of stimulant use disorder in people with psychosis were higher in studies from Australia and the USA than in studies from the UK and Europe. Studies from the USA mainly reported cocaine use disorders and Australian studies mainly reported abuse of amphetamine-related stimulants. These findings mirror regional differences in stimulant use in the broader population: the Global Burden of Disease Study (Degenhardt et al., 2014) found high rates of stimulant dependence in North America, South East Asia and Australasia, with cocaine being the main stimulant used in North America and amphetamines being more prevalent in Australasia and South East Asia. This suggests that people with psychosis may be influenced by the same social and environmental drivers of drug use and choice as other people in their community. It also suggests that the impact of stimulant drugs on people with psychosis might be greater in the USA and Australia than in some other regions.
In univariate analyses, higher rates of stimulant use disorder were reported by studies of people with affective psychoses. There are several possible explanations for this finding. First, it is based on a small number of studies, and may be a chance finding or influenced by other characteristics of those studies. Second, people with affective psychoses may use stimulants as self-medication for experiences of depression or dysphoria (Barch and Carter, 2005; Mueser et al., 1998). Third, recent evidence suggests a strong relationship between affective disorders and psychotic experiences in the general population (van Os, 2014), and it is possible that stimulants and other substances interact with vulnerabilities to both mood disturbance and psychotic experience. Finally, substance use disorders can cause diagnostic uncertainty in psychosis (Mathias et al., 2008; Sara et al., 2014a) and it is possible that stimulant misuse causes overactivity or elation, contributing to misdiagnoses of an affective disorder. On the other hand, our findings are less consistent with ‘reward deficiency’ models, which focus on anhedonia, negative symptoms and antipsychotic medication as primary causes of stimulant and other substance comorbidity in psychosis (Bedard et al., 2013; Blum et al., 1996; Green et al., 1999). These would predict higher rates of stimulant use disorder in studies of schizophrenia and in studies of established or chronic psychosis: we found that studies of schizophrenia reported lower rates than those of affective psychosis, and rates of stimulant use disorder did not differ between studies of early psychosis and those of established or chronic psychoses (Bedard et al., 2013; Blum et al., 1996; Green et al., 1999; van Os, 2014)
We did not find a significant change in the rate of stimulant use disorder in people with psychosis between 1974 and 2009. This negative finding may have been due to the substantial between-study heterogeneity. However, it is also consistent with the Global Burden of Disease Study, which found no discernible increase in the prevalence of stimulant dependence in the general population between 1990 and 2010 (Degenhardt et al., 2014).
Finally, we also found higher rates of stimulant use disorder in studies of people in hospital settings than in community or mixed settings. This may reflect better detection and diagnosis of substance comorbidity in hospital settings, a greater level of severity and acuity in hospital settings, or selection of people more likely both to use substances and to require inpatient care (e.g. younger males or people with fewer personal or social supports). However, higher rates of stimulant use disorder in inpatient settings would also be consistent with stimulants playing a role in precipitating or worsening psychosis. We have previously found that admissions to New South Wales mental health units with stimulant-related psychosis occurred more often during periods of greater amphetamine availability (Sara et al., 2011b).
Limitations of the study
This study aimed to examine factors contributing to between-study variation in stimulant use disorder estimates; however, the high degree of heterogeneity in these estimates is also a limitation of this study. Many of the pooled estimates in subgroup analyses had wide confidence intervals, and therefore some negative findings in this study may reflect type II error. For example, estimates of lifetime abuse of any drug would be expected to be higher than estimates of recent abuse: we found lifetime rates of stimulant use disorder were non-significantly higher than recent rates.
We found that rates of stimulant use disorder were low in studies with higher variance, suggesting that the pooled estimate of the rate of stimulant use disorder has not been inflated by publication bias. We excluded studies whose selection criteria appeared likely to bias the estimated rate of stimulant or other drug use, and found that studies with potentially non-representative samples did not have systematically higher rates than those with more clearly representative samples. However, there may have been other sources of selection or reporting bias in the studies included. All studies examined were in English, and there were more estimates and higher precision in estimates from English-speaking countries. There were few studies from many individual countries; lower estimates from those countries may reflect less complete capture of studies or systematic differences in studies from those countries published in English compared with other languages. Self-reported drug use may differ systematically between countries, and is likely to be underestimated in countries where drug use may lead to more serious criminal sanctions. We examined stimulant use disorders as a group since few studies reported on stimulant abuse or dependence as separate disorders. The strong correlation between stimulant use disorders and cannabis use disorders also suggests that some of the univariate associations found may be non-specific associations of substance use disorder rather than specific associations of stimulant use disorder. As in any meta-analysis, the associations found are ecological associations, and may not be reflected in individuals.
Conclusions
People with psychosis abuse stimulants at much higher rates than the general community. The type of psychosis, service setting and country all affect estimates: higher rates of stimulant use disorder are reported in studies of affective psychosis, from inpatient settings or from the USA and Australia. Methodological factors contribute little to between-study variation in rates of stimulant use disorder. Increased rates of stimulant use disorder are not limited to younger people or earlier stages of psychosis, suggesting that stimulants may contribute to the burden of psychosis at all stages of illness, from early psychosis to established schizophrenia. Cannabis use disorders are the strongest correlate of stimulant use disorders in studies of people with psychosis. Further research is required to disentangle the adverse effects of stimulants and cannabis: clinical or population-based studies using very large samples are likely to be required.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.