
Abstract
Suicidal ideation is a precursor for attempted suicide and suicide [1]. Community surveys have found particularly high levels of suicidal ideation after the early adolescent phase of development [2] with females usually reporting higher rates of ideation than males [3–7]. There is also a well-recognized link between depression and suicidal ideation, with depression significantly increasing the likelihood of suicidal ideation [8]. Because depression is such an important risk factor, adolescent depression has become a key research focus for suicide prevention among young people [9].
Large-scale epidemiological studies have found that before adolescence rates of clinical depression are similar among boys and girls [10]. During adolescence the prevalence of depression among females increases markedly, while the rise for males is more modest [11–13]. The female : male ratio for clinical depression changes from approximate equivalence in childhood, to a female preponderance of 2:1 and this approximate ratio continues into adulthood. Studies using self-report measures have also found that females report higher mean levels of depressive symptomatology and a greater proportion of females will score above standard cut-off points for identifying depression compared with males [14, 15]. Despite a range of promising hypotheses, the reason for this increase in rates of depression for females is not clear [16].
The higher levels of depressive symptomatology for females compared with males is one possible explanation for the higher rate of female suicidal ideation. Alternatively gender itself might increase the risk for suicidal ideation quite independently from levels of depression. For example, even with the same level of depression females may be at greater risk of suicidal ideation than males. Indeed some commentators have speculated that females are more likely than males to express ideation in response to even quite low levels of depressive symptomatology and that this trend is more evident among young people in developed societies [6]. The possibility of a gender difference in the risk relationship between depression and suicidal ideation has yet to be systematically examined.
The present study sets out to model the risk relationship between depressive symptomatology and suicidal ideation for males and females in a large community cohort of young adolescents. Depressive symptomatology was measured with the widely used Centre for Epidemiological Studies Depression Scale (CES-D) [17]. Very little Australian CES-D data for community adolescent samples has been reported. The second aim of the study therefore was to examine the average level of depressive symptomatology among Australian adolescents in relation to levels found in other similar overseas samples.
Method
The data reported in the current study were collected in the first year of the Early Detection of Emotional Disorders (EDED) programme carried out by Southern Child and Adolescent Mental Health Service in 25 rural and suburban secondary schools in South Australia [18]. Data were collected from a questionnaire administered during a single classroom session. Students in these schools were drawn from lower to upper-middle socioeconomic catchment areas. The programme was approved by the Committee on Clinical Investigation (Ethics) of Flinders Medical Centre based on guidelines developed by the National Health and Medical Research Council of Australia. The total number of students involved in year 8 was 2489 which representedapproximately 85% of eligible students. No data is available on the gender of those students who did not take part in the programme. Of the 2489 students who took part in the program 2028 (1109 males and 919 females) or 81% provided fully completed questionnaires and are included in the analyses. The mean CES-D item score for students who provided a fully completed questionnaire compared with students who did not complete all questions was not significantly different for either males (t = 1.68, p = 0.09) or females (t = 0.92, p = 0.36).
Depression was measured using the CES-D which has been widely used internationally in studies of adolescents. The CES-D is a brief, self-report rating scale designed to measure group differences in depressive symptoms among community samples [17]. The scale consists of 20 items in which respondents indicate the frequency of particular depressive symptoms using four points ranging from 0 (rarely or none of the time), 1 (some or little of the time), 2 (occasionally or a moderate amount of the time) to 3 (most or all of the time). Unlike many self-report depression scales the CES-D does not include any items referring to suicide. The CES-D has respectable validity and reliability in the general adolescent population [19]. In the present sample the internal reliability of the CES-D measured by Cronbach's coefficient alpha was similar to that reported in other studies [16, 20] with adolescents (males α = 0.88, females α = 0.92, total α = 0.90).
Most studies treat the total CES-D score as a continuous variable with higher scores indicating higher levels of depressive symptomatology. In the present study the CES-D is also analysed as a continuous variable but for descriptive purposes the terminology outlined by Roberts [19] was adopted to classify adolescent depression across the range of possible CES-D scores. Students with CES-D scoresbetween 0 and 15 are referred to as ‘not depressed’, 16 and 20 as ‘mildly depressed’, 21 and 30 ‘moderately depressed’ and 31 and aboveas ‘severely depressed’.
Suicidal ideation was determined using the Adolescent Suicide Questionnaire (ASQ) [21] which is a 20-item self-report instrument that includes a series of questions about the spectrum of suicidal behaviours. The questions are framed in direct and simple language about thinking, planning, threatening, deliberate self-harm or trying to kill yourself. Students responding in the affirmative to any of these behaviours were also asked a series of questions about when this behaviour had occurred, how often it occurred and how likely they felt it would continue. The question for suicidal ideation was as follows: ‘Have you ever thought about killing yourself?’. Students who indicated that ‘Yes’ they had thought about killing themselves were classified as having had suicidal ideation. Students who responded ‘Never’ were classified as not having had suicidal ideation. In the present study the variable for suicidal ideation therefore is categorical (No/Yes).
Logistic regression was used to estimate the probability of suicidal ideation (No/Yes) with the single independent variable of CES-D total score. Two logistic regression analyses were performed: one for males and one for females. The EDED data-set is not random sample of South Australian students because a ‘two stage cluster sample design’ was used to select schools in the first stage of sampling followed secondly by students within those schools. Traditional statistical techniques assume that all observations are independent and if this assumption is violated, as it is in the present study, the results can be biased. To examine the effects of the clustering in the data-set two multilevel logistic regression analyses (for males and females separately) were performed. The results (available from the first author) were virtually identical to those carried using ordinary logistic regression. Because readers are likely to be more familiar with traditional logistic regression it is these results which are presented.
The key statistical technique used to examine more closely the relationship between depressive symptomatology and ideation is based on item response theory (IRT). A large number of different types of IRT models have been developed. A key component of IRT is what is known as the item characteristic curve (ICC) [22–24]. In the context of the present study ICCs were calculated for males and females to describe the probability of reporting suicidal ideation (a dichotomous variable) as a function of the severity of depressive symptomatology. The ICCs were calculated using non-parametric kernel-smoothing techniques with the level of depressive symptomatology estimated with maximum likelihood (ML) techniques [25].
A non-parametric kernel-smoothing IRT technique was chosen over the more usual logistic function model because this technique allows for the ordinal response format of CES-D items and is better suited to analyses of items which have not been developed with the logistic function in mind. Level of depressive symptomatology was estimated using Maximum Likelihood techniques to take into account that not all CES-D items are equally effective in measuring depression and that intervals among options (e.g. 0,1,2,3) may not be psychologically identical. For these reasons the ML technique provides a more accurate estimate of an individual's true level of depressive symptomatology than does a score calculated by simply summing all 20 items. The analyses were carried out using the TestGraf software package [26] and followed closely the analytical approach described in a series of papers by Santor and colleagues [26–28].
Results
The sample was predominantly white (99%) and the average age was 13.5 years. Basic descriptive statistics are reported in Table 1. A significantly greater proportion of females (27.3%) than males (18.9%) reported suicidal ideation (χ2 = 20.08, p < 0.01). Students reporting suicidal ideation on average (mean score = 22.3) had significantly (t = 20.40, p < 0.01) higher total CES-D scores than those who denied suicidal ideation (mean = 9.7). This was true for both males (mean = 9. 5 vs 19.7, t = 12.05, p < 0.01) and females (mean = 9.9 vs 24.5, t = 16.62, p < 0.01).
Descriptive statistics
The mean CES-D score for females of 13.9 was significantly higher than the mean score for males, 11.4 (t = 5.32, p < 0.01). The higher average CES-D score for females was also reflected in the proportions of females scoring above classification cut-off points. Nearly onethird (n = 293, 31.8%) of females scored above the standard CES-D cut-off point of 16 with 10% classified as ‘mildly depressed’, 10%as ‘moderately depressed’ and 12% as ‘severely depressed’. This compares with only around one-fifth (n = 245, 22.1%) of males who scored above the standard CES-D cut-off point of 16 with 9% classified as ‘mildly depressed’, 8% as ‘moderately depressed’ and 5%as ‘severely depressed’.
Logistic regression analysis indicated that there was a statistically significant positive linear relationship between the total CES-D score and the probability of reporting suicidal ideation (males: Wald = 148, df = 1, p < 0.01; females: Wald = 187, df = 1, p < 0.01). For every one point increase in CES-D score the odds of reporting suicidal ideation was increased by a factor of 1.12 for males and 1.13 for females. Despite these relatively high odds ratios, only 93 males and 167 females had CES-D scores high enough to be at least 50% likely to report ideation. Using the total CES-D score to predict ideation (with a cut-off value of 0.50 probability), 29% of males with ideation and 47% of females with ideation were correctly identified.
Figure 1 shows the probability that males will report suicidal ideation as a function of expected CES-D score. The vertical dashed lines in the figure represents the 5th, 25th, 50th, 75th and 95th percentiles of the sample distribution while the vertical lines intersecting the curve indicate 95% confidence intervals (error bars). Relatively few males (see Fig. 1) had expected CES-D scores above 30 and consequently the estimated probability of ideation for these students was not well defined and the 95% confidence intervals wide. Given the paucity of data for estimating the probability of ideation at high levels of expected CES-D scores only the results for scores of less than 45 are shown.
Males’ probability of ideation.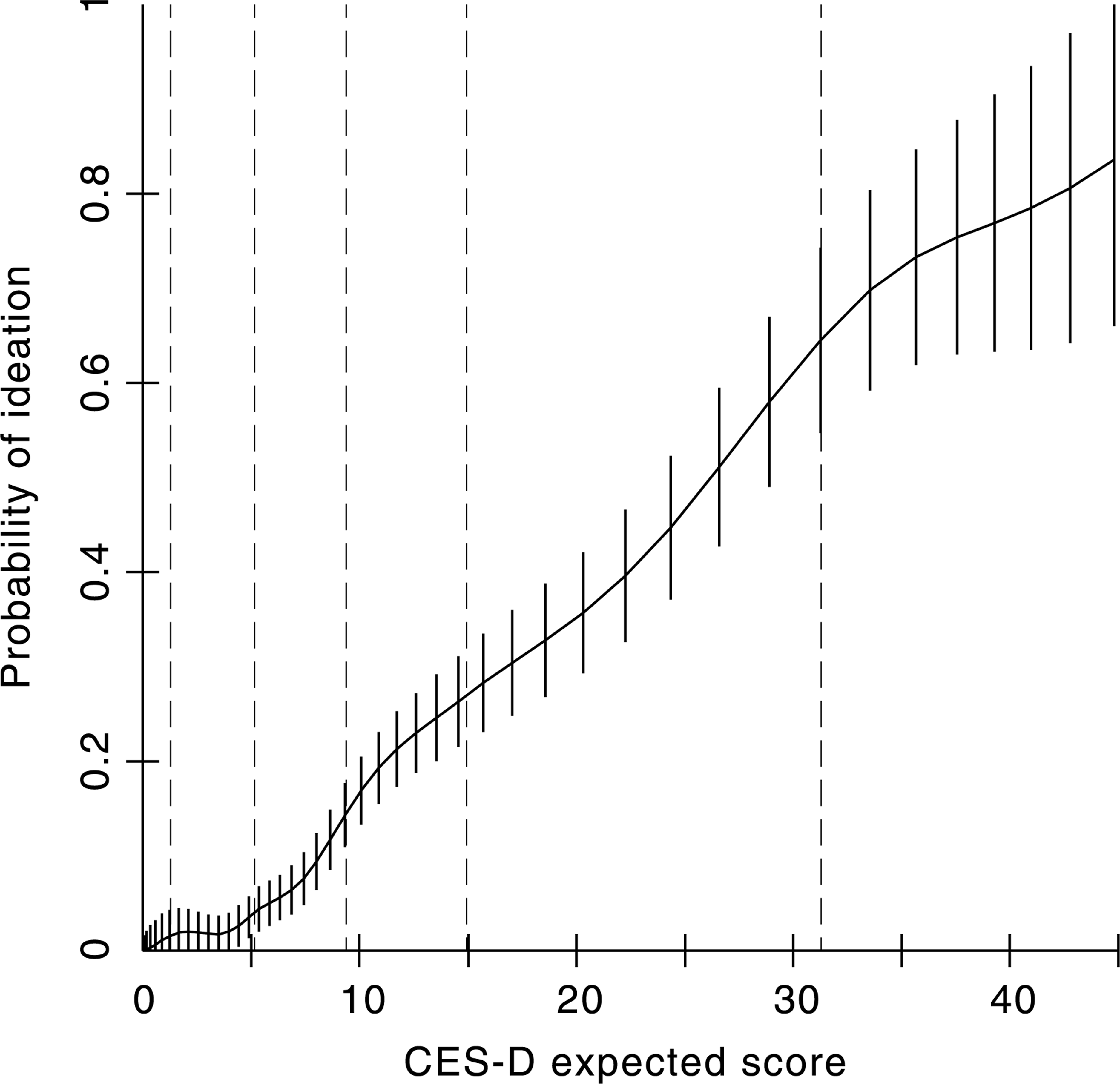
From Figure 1 the 25th percentile for males corresponded to an expected CES-D score of approximately 6 and an associated ideation probability of 0.05, the 50th percentile corresponded to a expected CES-D score of 9 and an associated probability of 0.14, the 75th percentile corresponded to a expected CES-D score of 15 and an associated probability of 0.28, and the 95th percentile corresponded to a expected CES-D score of 32 and an associated probability of 0.69. At an expected CES-D score of approximately 28, males were 50% likely to report ideation.
Figure 2 presents the probability of ideation by expected CES-D score for females. The 25th percentile corresponded to an expected CES-D score of 5 and an associated ideation probability of 0.06, the 50th percentile corresponded to an expected CES-D score of 11 and an associated probability of 0.16, the 75th percentile corresponded to an expected CES-D score of 19 and an associated probabilityof 0.47, and the 95th percentile corresponded to an expected CES-D score of 41 and an associated probability of 0.83. At an expected CES-D score of approximately 20, females were 50% likely to report ideation.
Females’ probability of ideation.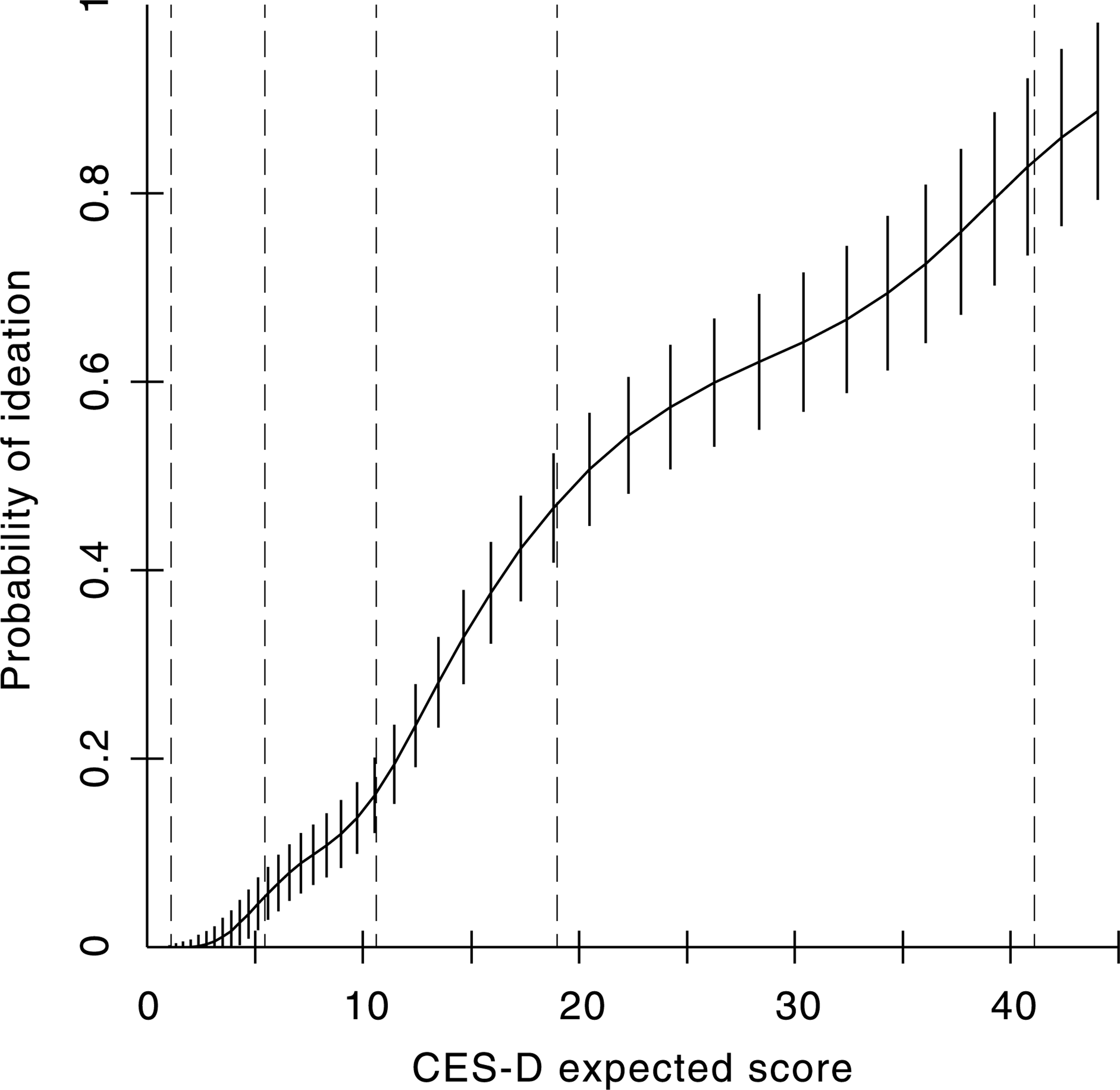
Figure 3 transposes the data series for males and females on to the same figure. When we compare males and females striking differences are apparent on expected CES-D scores between 18 and 25. Not depressed (i.e. scores less than 16) males and females had similar probabilities of reporting ideation: for example at an expected CES-D score of around 10 the probability of reporting ideation was around 0.15 for both males and females. Between scores of 10–15 there was more than a doubling of risk for females while the rate of increase for males was more modest. At scores of around 22 the steepness of the curve for females reduces while the steepness of the curve for males increases. For severely depressed (i.e. scores of 31 and above) males and females the probability of ideation is again roughly equivalent. The 95% confidence intervals are not shown in this representation for reasons of clarity but they do not overlap for CES-D scores between around 18 and 25 as can be seen from the previous figures for males and females.
Males (––) and females (·······) probability of ideation.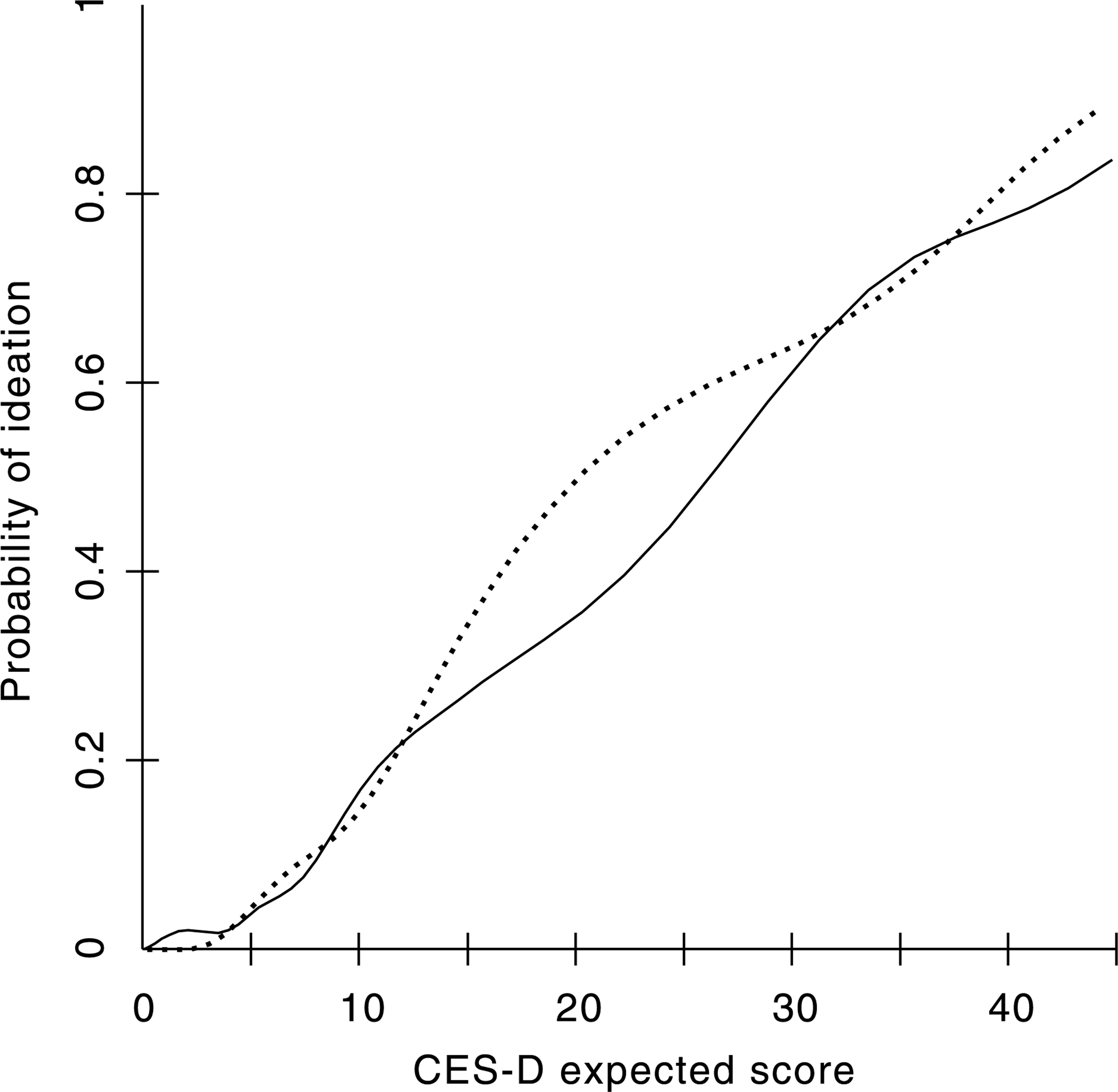
Discussion
Suicidal ideation was widespread in this large cohort of Australian students during their first year of secondary school. Nineteen per cent of males and 27% of females reported ideation. This level of suicidal ideation and the gender difference (favouring females) is consistent with the results found in other surveys of adolescents [2]. Females in this study reported higher levels of depressive symptomatology than males, and this gender difference is also consistent with previous studies [15, 16]. As expected there was a strong positive relationship between the probability of reporting ideation and CES-D depression scores. Among both females and males this meant that higher mean depression scores were associated with higher levels of suicidal ideation.
Although the CES-D has been widely used in the USA, this is the first study to report CES-D scores for an Australian community sample of young adolescents. The average CES-D score in this sample of 12.5 was lower than that obtained from studies of high school students in different parts of the USA (e.g. South Carolina: mean = 15.6 [3], Connecticut: mean = 16.7 [29], Oregon: mean = 17.0 [19], rural Southern communities: mean = 17. 16 [30] and Boston: mean = 14.98 [31]). The sample of students in the present study was younger on average (13 and a half years of age) than students in these other studies and this may possibly account for the lower levels of depressive symptomatology found for Australian adolescents compared with their USA counterparts.
Numerous studies have demonstrated that levels of depressive symptomatology and suicidal ideation are higher in females compared with males. It is also known that depression and suicidal ideation are stronglyassociated [1, 8]. The results of the present study are consistent with these earlier findings in that the probability of ideation increased progressively with higher levels of depression for both males and females. A closer inspection of the trends, however, showed significant differences between males and females. At moderate levels of depressive symptomatology (particularly CES-D scores between 18 and 25) females experienced a significantly higher risk of ideation than males. Importantly the increased risk for suicidal ideation among females does not appear to apply at either low, mild or severe levels of depression: only in the moderate range.
The increased female risk of suicidal ideation at moderate levels of depressive symptomatology is one reason why females have higher overall rates of suicidal ideation than males. Another reason is the greater proportion of females with high levels of depressive symptomatology. For example, 11.5% of females vs only 4.9% of males had CES-D scores high enough to be at least 50% likely to report suicidal ideation. This combination of a greater proportion of females with moderate to severe levels of depression together with their increased risk in the moderate range contributed to the higher overall level of female suicidal ideation.
The current study is limited to a cross-sectional design and self-report methods. The significance of the selfreported depression was not assessed by structured interview and many students with moderate to severe levels of depressive symptomatology were likely to have been in the subclinical range. Even moderate levels of depressive symptomatology (below the threshold for clinical depression) have been found to be associated with considerable impairment [32]. Consistent with these findings, the results from the present study show that moderate levels of depressive symptomatology are also associated with an increased risk of suicidal ideation.
Replication of these results in other adolescent populations is necessary to provide greater confidence about the validity of the findings. This will require the use of IRT statistical methods which allow the risk relationship between depressive symptomatology and suicidal ideation to be delineated across the different levels of depressive symptomatology. Further research could also profitably investigate whether the different risk relationship between depressive symptomatology and suicidal ideation for males and females is caused by gender specific responses to particular depressive symptoms. Clinically the results of the present study suggest that a substantial proportion of young adolescents (particularly females) presenting with moderate levels of depressive symptomatology will also have suicidal ideation and that a suicidal risk assessment should be undertaken.
Footnotes
Acknowledgements
We are grateful to Vikki Dadds and Kerin Williams for assistance during the implementation of the Early Detection of Emotional Disorders program and to Robert Goldney for his helpful comments on an earlier version of this paper.