
Abstract
Patients with the familial form of cerebral cavernous malformations (CCMs) are haploinsufficient for the CCM1, CCM2, or CCM3 gene. Loss of corresponding CCM proteins increases RhoA kinase-mediated endothelial permeability in vitro, and in mouse brains in vivo. A prospective case-controlled observational study investigated whether the brains of human subjects with familial CCM show vascular hyperpermeability by dynamic contrast-enhanced quantitative perfusion magnetic resonance imaging, in comparison with CCM cases without familial disease, and whether lesional or brain vascular permeability correlates with CCM disease activity. Permeability in white matter far (WMF) from lesions was significantly greater in familial than in sporadic cases, but was similar in CCM lesions. Permeability in WMF increased with age in sporadic patients, but not in familial cases. Patients with more aggressive familial CCM disease had greater WMF permeability compared to those with milder disease phenotype, but similar lesion permeability. Subjects receiving statin medications for routine cardiovascular indications had a trend of lower WMF, but not lesion, permeability. This is the first demonstration of brain vascular hyperpermeability in humans with an autosomal dominant disease, as predicted mechanistically. Brain permeability, more than lesion permeability, may serve as a biomarker of CCM disease activity, and help calibrate potential drug therapy.
INTRODUCTION
Cerebral cavernous malformations (CCMs) affect more than 0.5% of the population, with an associated cumulative lifetime risk of hemorrhage, epilepsy, and other neurologic sequelae.1,2 A CCM lesion consists of clusters of hemorrhagic dilated anomalous vessels (‘caverns’) lined by endothelium with defective intercellular junctions, and devoid of mature vessel wall angioarchitecture.3,4 Multifocal CCM lesions arise in familial cases with autosomal dominant mutations in CCM1 (KRIT1), CCM2, or CCM3 (PDCD10) genes. Isolated CCM lesions appear sporadically, often in association with a developmental venous anomaly, and in the absence of germ line mutations. 5 Currently, there is no proven therapy to prevent lesion genesis or alter the course of the disease.
Our team and others have previously shown that in vitro monolayer endothelial permeability increases in cells treated with CCM1, CCM2, or CCM3 siRNA. This hyperpermeability is associated with RhoA kinase (ROCK) activation, and can be rescued by ROCK inhibition.3,6,7 We also showed hyperpermeability to Evans blue dye in vivo in the brain and lungs of Ccm1 haploinsufficient mice, also rescued by ROCK inhibition. 3 The ROCK activity has been linked to increased CCM lesion burden in mice, and ROCK inhibition is being tested as a potential therapy to prevent CCM lesion development. 8 A similar vascular hyperpermeability would be expected, but has never been shown, in patients with familial CCM disease, which may represent a biomarker of disease activity and response to treatment.
We have applied the technique of dynamic contrast enhanced quantitative perfusion (DCEQP) to assess brain vascular permeability to gadolinium contrast agent in patients with CCM disease. We postulated that familial CCM patients, who are heterozygous for mutations in CCM genes, have increased brain permeability as compared to subjects with sporadic CCM, and nonCCM controls. We also proposed that increased brain permeability in familial CCM patients would correlate with a more aggressive CCM disease phenotype. Furthermore, we explored the pilot proposition that CCM patients receiving statin medications, which are known to have pleiotropic effects including RhoA inhibition,9–11 may exhibit comparatively decreased brain permeability versus those CCM subjects not on drug therapy.
MATERIALS AND METHODS
Subjects
Written informed consent was obtained from all participants according to the Declaration of Helsinki of 1975 (and as revised in 1983), with approval by The University of Chicago Institutional Review (IRB). Review and surveillance were conducted to assure the protection of the rights and welfare of all research subjects, including patient anonymity and confidentiality of patients' records. The ethical principles that guide the IRB are consistent with The Belmont Report, and comply with the rules and regulations of The Federal Policy for the Protection of Human Subjects (56 FR 28003; often referred to as the ‘Common Rule’). This prospective case–control observational study was designed with the following patient inclusion criteria: the presence of known CCM disease (either the sporadic of the familial form) diagnosed by imaging criteria, genotyping, or histopathology; and the absence of any other known brain pathology or a history of prior brain irradiation. NonCCM control subjects were patients with no known CCM disease, who presented concurrently for evaluation of neurologic symptoms requiring magnetic resonance imaging (MRI) scan with contrast, and subsequently were found not to harbor any brain pathology on their imaging (exclusion criteria). These were not specifically age matched.
Consecutive cases meeting the above criteria were consented for enrollment in the study at the time of contrast-enhanced clinical MRI, planned for routine clinical evaluation or follow-up at the University of Chicago Medical Center. Indications for gadolinium administration in clinical practice are well established, and include the need for visualization of associated venous anomalies, differentiating between tumor versus CCM lesion, and identifying associated tumors in patients with known familial CCM disease.5,12 Enrolled subjects received DCEQP image acquisition in conjunction with their clinical MRI. No additional gadolinium was administered solely for the purpose of this research.
All but one patient reporting for CCM evaluation or follow-up imaging between November 2012 and September 2014 consented for participation in this study. Twelve scans (10.2%) were excluded due to bad input functions derived from the contrast signal or due to poor contrast administration, five scans (4.2%) due to head motion, and one scan (0.85%) due to the improper selection of image slices during acquisition. Another 11 scans (9.3%) were excluded due to subsequently discovered concomitant brain disease. In all, 89 of 118 scans (75.4%) from 69 CCM subjects and 6 controls were ultimately used in the present analyses (Table 1).
Characteristics of study participants, and number of subjects in each category
Abbreviation: CCM, cerebral cavernous malformation.
Image Acquisition and Processing
All scans were performed using a 3T Philips Achieva TX MRI/MRS system with MultiTransmit Parallel RF Transmission Technology, Quasar Dual Gradient System, and 32-Channel Architecture (Best, The Netherlands). Permeability experiments were performed according to the previously published protocols,13,14 using either gadodiamide or gadobenate dimeglumine contrast. This technique allows the computation of permeability index maps corresponding to respective pixels on matched axial magnetic resonance images.13–15 Unlike conventional MRI scans, the DCEQP technique requires the selection of axial slices for desired regions of interest because of limited time for dynamic imaging after contrast administration.14,15 Up to five axial slices were selected in each case, to permit sampling of as many CCM lesion(s) and normal brain parenchyma as possible (Figure 1). In 39 familial cases, 198 lesions (mean 5.1 lesions per subject) were visible on the axial slices, and were subsequently analyzed. In 30 sporadic cases, the index lesion was analyzed in every case.
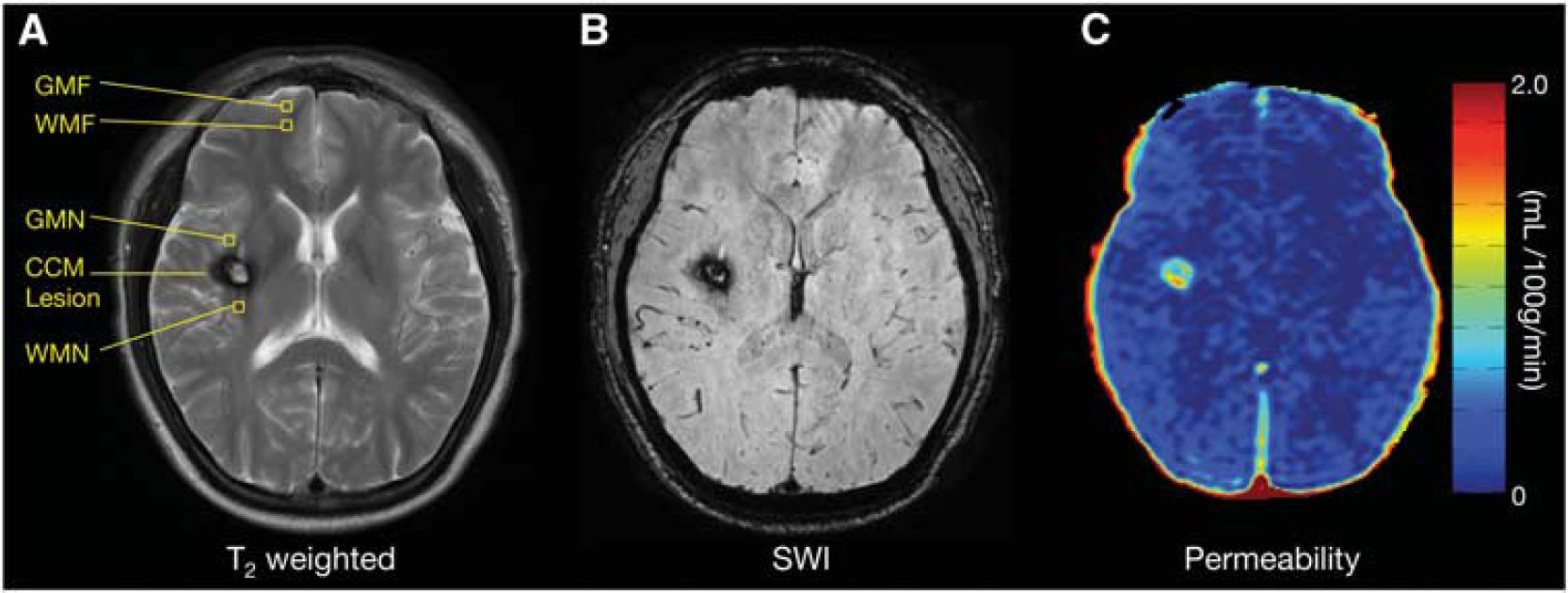
Magnetic resonance images of an axial slice from a patient with sporadic cerebral cavernous malformation (CCM) disease. (
Regions of interest (ROIs) were selected using Image J software (Bethesda, MD, USA: US National Institutes of Health; 1997 to 2011) on T2-weighted images acquired in the same orientation and immediately before the T1-weighted images. Lesional ROIs included the entire CCM lesion, including surrounding hypo-intense ‘hemosiderin ring,’ as seen on T2-weighted images. Normal brain ROIs consisted of square areas of 12.9 mm 2 (16 pixels) of gray matter near (GMN), white matter near (WMN), gray matter far (GMF), and white matter far (WMF) from lesions. Far regions were chosen in brain devoid of CCM lesions on any MRI sequence, including any small punctate lesions seen on respective susceptibility weighted imaging (SWI), and > 16 mm away from the border of any lesion seen on T2-weighted imaging. Near regions were defined as within 16 mm of the border of a CCM seen on T2-weighted images, or associated venous anomaly.
For each brain region (GMN, WMN, GMF, and WMF), numerous ROIs were selected on each axial T2 image, and were then averaged to yield a mean value per patient for subsequent analysis. In the 30 sporadic cases, we analyzed 800 ROIs within all 4 regions of background brain (mean 26.7/ subject), including a mean of 15.1 (range 3 to 38) for WMF ROIs per case. In 39 familial CCM cases, we analyzed 1,541 ROIs in the background brain (mean 39.5/subject), with a mean of 15 (range 2 to 66) for WMF ROIs per case. In nonCCM control patients, we obtained a mean of 14.2 (range 4 to 30) for normal brain white matter ROIs per case. For comparative internal validation, we also analyzed larger ROIs encompassing all lesion-free white matter areas in the same brain. For all subsequent analyses, the mean permeability index of all pixels within the respective ROIs was computed in units of mL/100 g per minute.
Data processing was performed by investigators who were blinded to the genotype of the patients whose data were being analyzed, and their associated clinical features.
Extraction of Clinical Parameters
For 10 randomly selected cases, one investigator performed permeability measurements of the same scan at two separate time points to assess for possible intraobserver variability. Furthermore, permeability measurements were also compared between two separate observers to account for any observer or ROI selection bias.
The electronic medical records of the patients were reviewed. Deidentified clinical information was collected and stored in a secure database. Cases were classified as familial in the presence of multifocal lesions on MRI, family history, and/or identified mutation on genetic screening. The genotype of familial cases was noted, and nongenotyped cases were characterized as ‘unknown genotype.’ Cases were classified as sporadic if they harbored a solitary lesion (or cluster of lesions with associated developmental venous anomaly).5,16 Lesion burden was cataloged including the number of CCM lesions seen on T2-weighted images and on SWI sequences in each case. 16 If the patient had > 100 lesions on SWI images, the number of lesions counted was considered as 100.
Overt hemorrhage was defined according to the criteria of Al-Shahi et al. 17 Other extracted clinical parameters included age, sex, the presence or absence of seizures, age at first bleed, first symptom and first diagnosis, number of clinical bleeds, and time between most recent bleed and the permeability study.
Statistics
Interobserver and intraobserver consistency was confirmed using Bland-Altman plot. Interpatient and intrapatient variability was evaluated using coefficient of variance (CV). The sample size calculation of N = 10 for intraobserver and interobserver analyses was chosen to provide 95% confidence, with a bias level of < 0.01.
Student's t-test with Welch's correction was used to compare permeability between sporadic versus familial cases. Pearson's correlation or Student's t-test was applied to examine the correlation between permeability and continuous or dichotomous factors of clinical activity, respectively. To meet the independence assumption of statistical tests, the mean value in the respective regions was calculated for each patient for the following analyses. For comparison of lesional permeability and hemorrhage, we considered the mean permeability in the respective lesion responsible for hemorrhage.
Correlations with age were performed as continuous variable, and post hoc between age groups to test apparent differences reflected by the data. Lesion burden was examined in familial cases (harboring multiple lesions) as a continuous variable, and per prespecified features of disease aggressiveness. 18 These included dichotomous classification of cases harboring more than 25 SWI lesions, more than 5 T2 lesions, and having more than one hemorrhage. These features of disease aggressiveness were examined alone and in combination in correlation with mean lesion and brain permeability.
For patients with multiple scans at different times, the first available scan was used in the aforementioned cross-sectional analyses, and the second scan was used only to compare changes over time within the same patient. For each patient with repeated scans, paired t-test was used to compare lesional permeability between repeated scans, while unpaired t-test was used on other regions (WMN, GMN, WMF, and GMF). Fisher's exact test was applied to compare the prevalence of significantly increased permeability between stable versus unstable patients (‘unstable’ denotes that their repeat MRI showed any of the following when compared with their first scan: increased lesion size, lesion hemorrhage, or new lesion formation). Statin effect was assessed using multivariate regression with genotype (sporadic versus familial) controlled for in the model.
All statistical analyses were performed using STATA12 (StataCorp LP, College Station, TX, USA). All reported P values were two sided and were considered to be statistically significant at *P < 0.05, **P < 0.01, ***P < 0.001.
RESULTS
Validity of Permeability Measurements Via Different Observers, Region of Interest Selection Methods, and Choice of Contrast Agent Used
Repeat analysis of patients by the same observer using the same images at two separate time points showed no significant difference in any ROI (Supplementary Figure 1). Furthermore, repeated ROI selection and analysis by two different observers also showed no significant difference in bias in WMF regions or CCM lesions (Supplementary Figure 2).
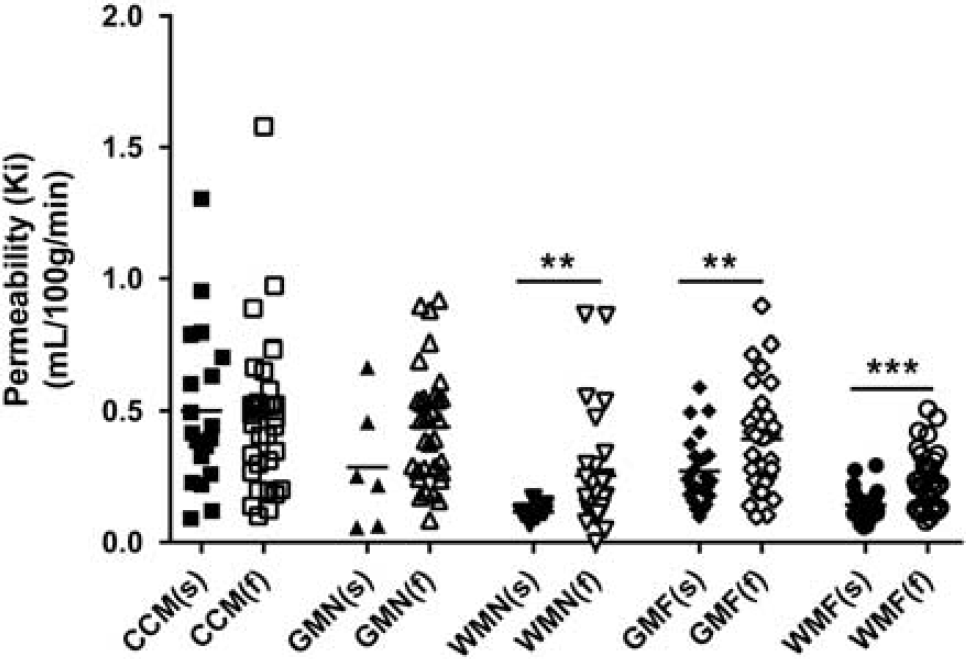
Permeability values in lesions and background brain in familial (N = 39) and sporadic (N = 30) cerebral cavernous malformation (CCM) patients. Each data point represents mean permeability index (Ki) in individual CCM lesions, or in regions of interest in background brain (averaged per patient). There were no significant differences in the average of the mean permeability indices in CCM lesions or in gray matter near (GMN) regions between sporadic (s) and familial (f) cases. In contrast, average background brain permeability indices per patient were significantly greater in familial than in sporadic cases in white matter near (WMN), gray matter far (GMF), and white matter far (WMF) regions. The difference was most pronounced in WMF regions. **P < 0.01 and ***P < 0.001.
The size of ROIs used did not alter the results of subsequent analyses. Using a larger ROI, as described in the Materials and Methods section, yielded significantly less variation in both sporadic and familial patients. While the variation was greater using smaller ROIs in combined sporadic and familial patients, the mean permeability was the same regardless of the ROI selection method used (Supplementary Figure 3).
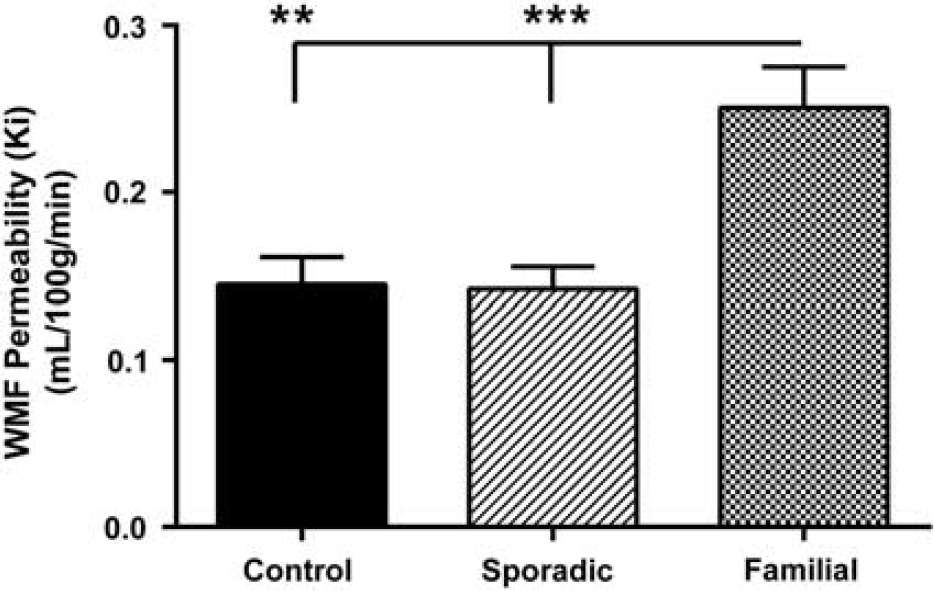
Permeability in white matter far (WMF) from lesions in control, sporadic, and familial patients with cerebral cavernous malformation disease. The mean WMF permeability in patients with familial disease was significantly higher than in control and sporadic patients (**P < 0.01 and ***P < 0.001, respectively).
When comparing the use of two different gadolinium contrast agents, gadodiamide and gadobenate dimeglumine, there was no significant difference in brain permeability measurements in either sporadic or familial patients (Supplementary Figure 4).
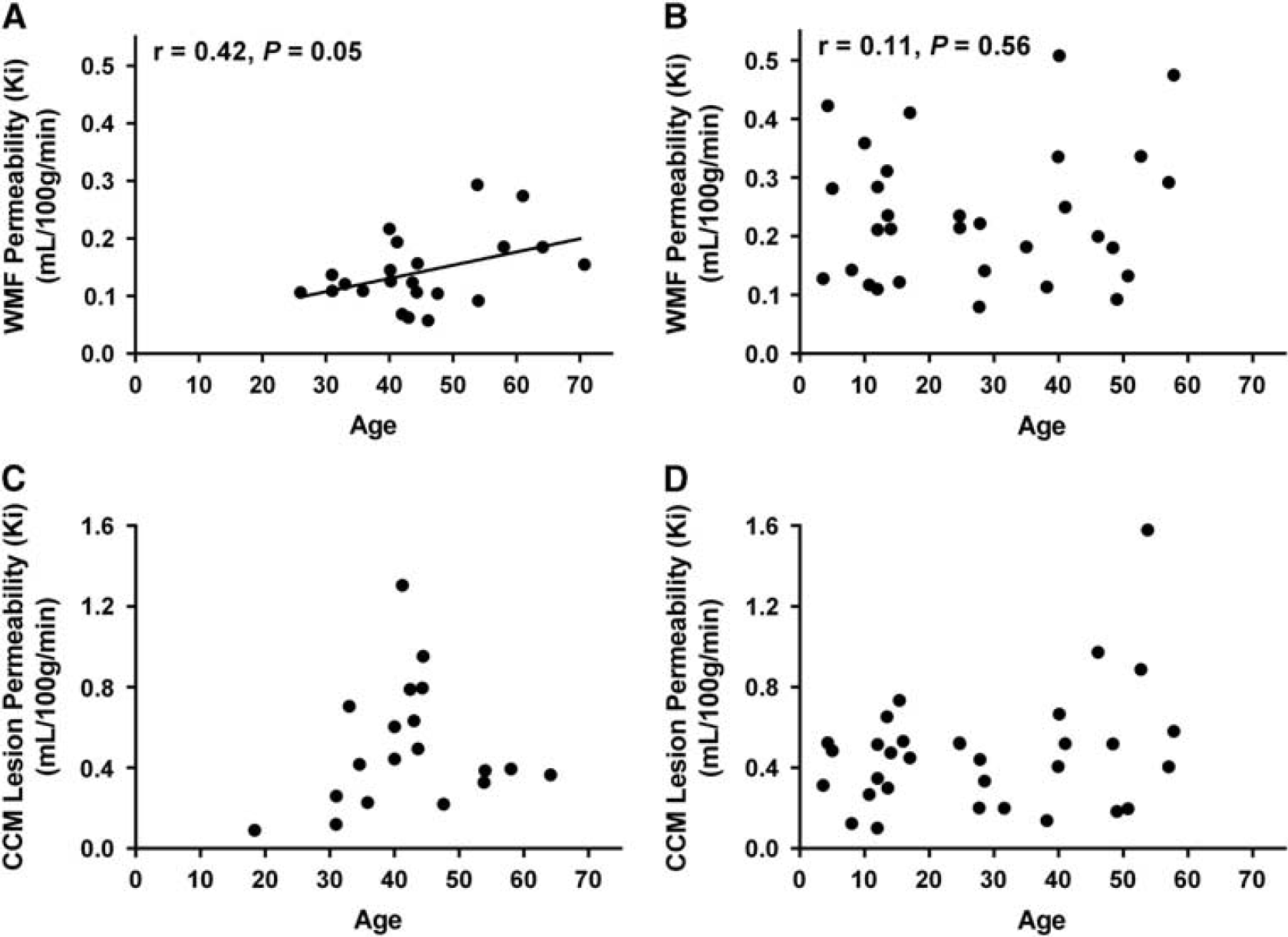
The effect of age on white matter far (WMF) and lesion permeability in patients with cerebral cavernous malformation (CCM) disease. WMF permeability was positively correlated with age in (
Variability in Brain and Cerebral Cavernous Malformation Lesion Permeability in Familial and Sporadic Patients
There was greater interpatient variation than intrapatient variation in permeability measures of brain and lesion ROIs in both sporadic and familial patient groups. For WMF regions, interpatient CVs were 2.29 and 2.09 for sporadic and familial patients, respectively, and intrapatient CVs were 0.85 and 0.86 for sporadic and familial patients, respectively. A greater interpatient versus intrapatient variation was also seen in CCM lesion permeability, with CVs of 1.46 and 0.72, respectively.
Brain and Cerebral Cavernous Malformation Lesion Permeability in Patients with Familial versus Sporadic Cerebral Cavernous Malformation Disease
There was greater brain permeability in familial CCM patients compared with sporadic cases (excluding patients on statin medications due to its potential pleiotropic effects on vascular permeability9–11). The difference was significant in WMN, GMF, and WMF regions (P < 0.01, P < 0.01, and P < 0.001, respectively). There was no significant difference between mean CCM lesion permeability per patient in the familial versus sporadic cohorts (Ki 0.50 and 0.47 mL/100 g per minute, respectively) (Figure 2). Mean permeability of WMN regions was similar to WMF regions in the sporadic (Ki 0.12 and 0.14 mL/100 g per minute, respectively) and familial patients (Ki 0.25 and 0.24 mL/100 g per minute, respectively).
Mean permeability of WMF ROIs had the least variability among cases in each of the sporadic and familial cohorts (Figure 2), and was the easiest and most accurate to select, due to the relative volume it occupies the total brain and its ease of distinction from adjacent cortical sulci. Mean WMF permeability was similar in nonCCM controls and sporadic patients, while familial patients had significantly higher WMF permeability than both (P < 0.01 and P < 0.001, respectively) (Figure 3).
Brain and Cerebral Cavernous Malformation Lesion Permeability Correlations with Patient Characteristics and Clinical Activity
In patients with sporadic CCM disease, WMF permeability exhibited a positive and significant correlation with age (r = 0.42, P < 0.05) (Figure 4A). In familial CCM cases, where permeability was greater than in sporadic cases, WMF permeability was unrelated to age (Figure 4B). Furthermore, sporadic CCM patients between ages 40 and 50 had higher CCM lesion permeability than other patients of all other ages (P < 0.05) (Figure 4C). However, there was no association of CCM lesion permeability with age in familial CCM cases (Figure 4D).
Neither brain nor CCM lesion permeability in either familial or sporadic CCM disease had a correlation with sex and age of symptom onset (headaches, seizures, or focal neurologic deficits). In either sporadic or familial cohorts, there was no significant association between brain or CCM lesion permeability and the age at which patients experienced their first hemorrhage, or the total number of hemorrhages experienced. Moreover, there was no temporal relationship between the time since patients' most recent hemorrhage and CCM lesion permeability. Specifically, when identifying the specific lesion responsible for a symptomatic hemorrhage, patients who had a hemorrhage in the past 3 months, 6 months, or 1 year did not have a significantly higher CCM lesion permeability compared with the average permeability of lesions of patients who had experienced earlier or no hemorrhage (data not shown).
Brain Permeability in Familial Cerebral Cavernous Malformation Patients with Aggressive Disease
Correlations among individual parameters of disease aggressiveness (lesion counts or hemorrhage) were not significant. Familial patients with aggressive disease phenotype (N = 8), defined as harboring greater than 25 lesions on SWI, > 5 lesions (≥5 mm diameter) on T2-weighted imaging, and a history of more than one clinical hemorrhage, had greater (P < 0.05) brain WMF permeability (Figure 5), but similar lesion permeability (not shown), compared with familial patients with more benign disease (N = 31).
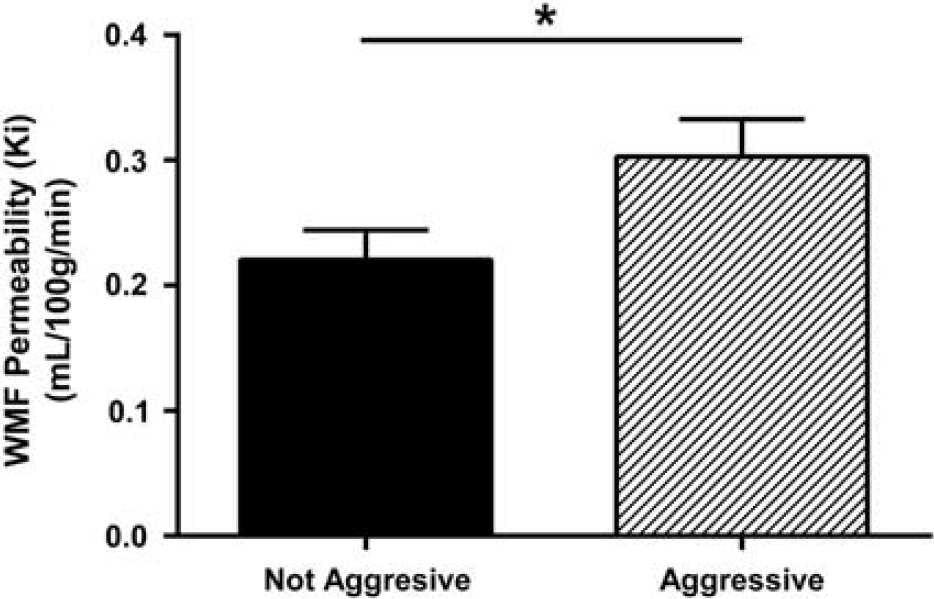
The average white matter far (WMF) permeability was significantly higher in familial cerebral cavernous malformation patients with aggressive disease (N = 8) compared with familial patients with milder disease (N = 31). Aggressive disease was defined as harboring > 25 lesions on susceptibility weighted images, > 5 lesions (≥5 mm diameter) on T2-weighted images, and a history of > 1 clinical bleed. *P < 0.05.
Repeat Permeability Measurements in Stable Versus Unstable Familial Cerebral Cavernous Malformation Patients
Fourteen patients with familial CCM disease were evaluated at two separate time points (ranging from 91 to 378 days apart) to assess their lesion and brain permeability (Supplementary Table 1). Patients were categorized as ‘unstable’ if their repeat MRI showed any of the following when compared with their first scan: increased lesion size, lesion hemorrhage, or new lesion formation. Patients meeting none of the above criteria were deemed ‘stable.’ Of the six patients categorized as ‘unstable’, four patients had increased brain permeability between scans, and one patient had increased lesion permeability between scans. Of the eight patients considered ‘stable’, six had similar lesion and brain permeability between scans, whereas two patients had significantly decreased brain permeability between their two visits. None reported any new symptoms or change in symptom severity. The prevalence of patients with significantly increased WMF permeability in the ‘unstable’ cohort is significantly higher than the ‘stable’ patient cohort (P < 0.05, Fisher's exact test).
Effect of Statins on Brain and Lesion Permeability
Nine patients (four sporadic and five familial) who were taking statin medications for cardiovascular indications at the time undergoing the permeability scan had a trend toward lower WMF permeability (P = 0.07), but similar lesion permeability, compared with those not on statins (Figure 6). No trends were observed between patients on anticonvulsant and antihypertensive medications and those without.
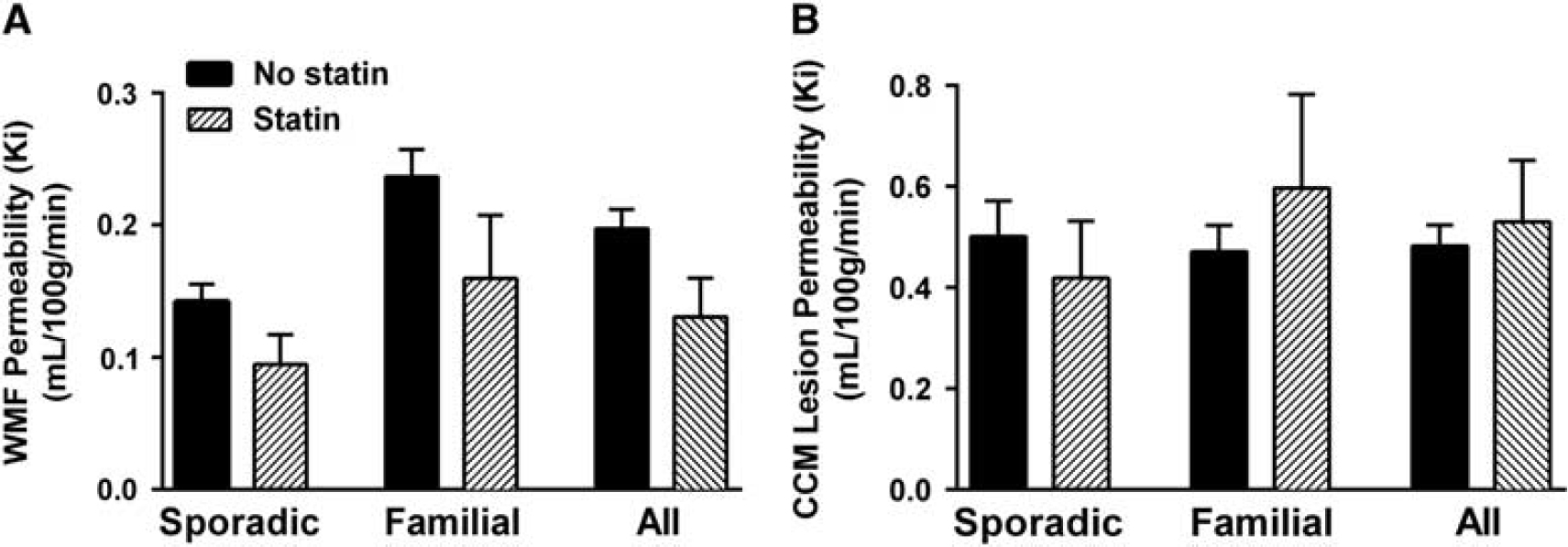
The effect of associated statin use on white matter far (WMF) and cerebral cavernous malformation (CCM) lesion permeability. (
DISCUSSION
Cerebral Cavernous Malformation as Vascular Permeability Disease Abnormal neurovascular architecture is central to CCM disease, with disruption of endothelial cell junctions and defective subendothelial layer in CCM lesions.19–21 The loss of CCM genes has been shown to cause ROCK-mediated vascular hyperpermeability in endothelial cells in vitro,3,6,7 and in the skin, 6 brain and lungs 3 of Ccm heterozygous mice. This hyperpermeability is rescued by ROCK inhibition, a proposed therapy for CCM disease.3,8,10 Statin medication was shown to reverse dermal hyperpermeability associated with heterozygous Ccm in mice. 6 Until the present study, it has not been determined whether vascular permeability measurements in the human brain could reflect the differences postulated mechanistically. Also, it is unknown whether differences in brain or CCM lesion permeability are associated with various aspects of clinical disease activity.
Results of DCEQP have been validated in relation to 14C-AIB quantitative autoradiography using rat models of tumors 22 and transient focal ischemia, 23 and in human pathologies with known hyperpermeability, including tumors and multiple sclerosis.14,24,25 The value of nonlesional brain white matter DCEQP as a biomarker of multiple sclerosis activity and response to treatment was recently shown by one of the co-authors. 24 While simpler magnetic resonance perfusion paradigms have been published previously and are widely used clinically,15,26 these differ from the DCEQP technique in that they assess blood flow and transition time, but do not allow the calculation of a vascular permeability index.
Hart et al 27 were the first to show the feasibility of DCEQP measurements in CCM patients. 27 That landmark study analyzed permeability in 39 CCM lesions in 14 CCM subjects, all with familial disease related to the Common Hispanic CCM1 mutation. In a previous study from our own group, we showed that CCM lesions with greater permeability also exhibited higher iron content. 13 These studies, however, did not systematically examine differences in brain or lesion permeability between sporadic and familial CCM cases, with the latter harboring haploinsufficiency of CCM genes. These studies did not analyze interobserver, intrapatient, and interpatient variability in permeability measurements. Neither were permeability measurements in relation to clinical disease activity examined, nor were changes in permeability over time.
Variability in Permeability Measurements
Our results validate intraobserver consistency and interobserver agreement in permeability measurements for both CCM lesions and WMF regions. We further validated the technique of selecting multiple small ROIs for WMF measurements, as compared with larger segmented areas. This approach is easier to implement in cases with familial CCM where ROIs of lesion-free brain must be carefully selected to avoid including tiny SWI lesions in the brain permeability regions. There was greater interpatient than intrapatient variability in all permeability measurements. This interpatient variability was greatest in WMF regions in familial cases, indicating that patients likely differ in inherent ROCK activity, and hence exhibit varying vulnerability to vascular permeability. Other observations helped clarify possible factors influencing interpatient variability in vascular permeability among CCM subjects.
Vascular Permeability Differences in Brain Versus Lesions
Our results herein confirm the primary hypothesis that nonlesional brain permeability is greater in familial CCM disease, which is known to harbor germline heterozygous mutations, compared with sporadic CCM cases and control subjects who lack those mutations. The loss of endothelial cell integrity in association with inherited heterozygous germ line mutations has been shown to result in ‘leaky’ vasculature not just within the CCM lesions themselves, but in nonlesional vascular beds. The increased brain permeability in familial patients compared with sporadic cases shows a direct translation of experimental observations made in murine models,3,8 and serves as a proof of concept that ROCK-induced brain vascular hyperpermeability may be quantitated in the clinical setting.
The CCM lesion vascular permeability did not differ between familial and sporadic cases, consistent with their known indistinguishable pathologic features. 28 Our group and others have reported somatic mutations of CCM genes in excised sporadic 29 and familial30–32 CCM lesion specimens. The presence of CCM germline mutations in familial but not in sporadic or control cases would result in brain hyperpermeability in areas devoid of lesions in familial cases only. Conversely, the CCM lesions themselves are not biologically different in sporadic and familial cases, and have similar permeability indices.
Age and Vascular Permeability in Brain and Lesions
We showed higher background brain permeability with advancing age in sporadic but not in familial cases. These results are consistent with ROCK-induced vascular hyperpemeability in aging endothelium, 33 but had never been shown previously in human subjects. In our study, familial CCM cases exhibited ROCK-induced hyperpermeability at all ages, as expected with CCM germline mutations. Another recent study found increased white matter hyperintensities (leukoaraiosis) in familial CCM1 subjects with advancing age, compared with age matched controls, 34 also suggesting that CCM haploinsiufficiency may enhance the effects of aging in the human brain. The present research was not aimed or powered at addressing the effects of aging on brain vascular permeability in normal subjects, but it raises cogent questions in this regard, to be addressed in future investigations aside from CCM.
Lesional permeability was significantly higher in sporadic cases aged 40 to 50 years as compared with younger and older subjects. This was an unexpected finding, but unmistakable when examining the data distribution. It will need to be confirmed in future studies, perhaps in correlation with clinical CCM lesion activity at various ages. Previous natural history study had suggested a low rate of CCM diagnosis in later decades of life, speculating about more quiescent behavior in the elderly. 35 The relation of vascular permeability to age will require further investigation, including a greater number of non-CCM control subjects in various age groups, and control for disease features and comorbidities.
Vascular Permeability and Clinical Disease Activity
Cerebral cavernous malformation patients often manifest with wide-ranging degrees of disease aggressiveness, making it difficult to predict their clinical course. Our results suggest that brain or lesional permeability did not correlate with any individual features of CCM disease activity in cross sectional comparisons, including recent hemorrhage. However, the cohort of familial cases with greater lesion burden and prior multiple clinical hemorrhages had significantly greater WMF permeability than familial cases with lesser aggressiveness. And in our limited cohort with longitudinal follow-up, cases with unstable clinical activity were more likely associated with increased permeability. These features will need to be reexamined in larger cohorts, stratified with sufficient subjects with the respective features and prospective follow-up.
Vascular Permeability Therapy and Role as Biomarker
Statins, with ROCK inhibitory pleiotropic effects, have been proposed as a potential therapy for CCM patients. 10 Others have cautioned whether statins might have deleterious effects in light of broader signaling effects beyond ROCK inhibition. 36 Our results herein indeed suggest that CCM patients taking statins for routine cardiovascular indications have a trend of lower white matter permeability compared with those not on statins. However, statins did not seem to have an effect on the permeability of the CCM lesions themselves. We caution that these observations are highly preliminary, and they were not controlled for duration or dose of statin therapy, nor age or patient or disease features. A Phase I trial is already underway to assess the potential safety of statin dose escalation in patients with familial CCM and the common Hispanic CCM1 mutation, and the study also is probing any potential effects on lesional and brain vascular permeability using similar DCEQP technique in a limited number of subjects (ClinicalTrials.gov Identifier NCT017644510). Our group is currently investigating the potential effect of ROCK inhibition therapy, comparing specific inhibitor fasudil and statins on CCM lesion development and vascular leak in murine models, sponsored by the United States National Institutes of Health (R01 NS077957). Another ongoing exploratory and developmental research study (R21NS087328) is seeking to correlate brain and lesional permeability in CCM subjects with ROCK activity measured in peripheral blood leukocytes. 9 Results from these various projects will complement preliminary observations reported herein, and generate further information on this topic, with potential clinical interest.
For clinical trials and beyond, it would be useful to validate a biomarker by which to monitor the clinical course of CCM disease, varied as it may be. Four out of six patients who were categorized as ‘unstable’ at the time they underwent repeat MRI scans as part of their routine clinical management (with findings of new lesion formation, lesion growth, or lesion hemorrhage) were found to have a significant increase in permeability between their scans in their background brain regions; however, only one of these patients had a concomitant increase in mean CCM lesion permeability. All patients who were deemed ‘stable’ at the time of their second scan had similar or decreased lesion and brain permeability, and none of the patients reported experiencing any new or worsening symptoms. Indeed, the sensitivity, specificity, and predictive value of permeability measurements in conjunction longitudinal clinical activity will need to be examined within a larger cohort, with sufficient representation of cases with varying disease and lesion phenotypes, and a greater number of age-matched control subjects, using multivariate methodology.
Brain vascular permeability could help select patients more likely to benefit from ROCK inhibition or other vascular permeability therapies, by targeting those with higher brain vascular permeability reflecting inherently higher ROCK activity. Drug dosing could also be titrated to lower vascular permeability to control levels. In this regard, brain vascular permeability may be a more sensitive biomarker than lesional permeability.
Limitations and Future Directions
An inherent limitation of the DCEQP technique is its nonvolumetric acquisition, necessitating the selection of 4 to 6 slices for analysis, during the time window of contrast perfusion. Hence, not all regions of the brain, or all lesions in familial cases can be sampled.
Other limitations of the current study were that most patients were observed in cross-sectional correlation rather than longitudinal follow-up. Initial validations suggested multiple factors that will require control in future studies, including age, genotype, and exposure to various drugs. Other factors including inflammatory biomarkers may also influence brain permeability and disease aggressiveness. 37
Our number of non-CCM control subjects recruited concurrently was small; hence, our comparisons were primarily aimed among cohorts with CCM (familial/multifocal versus sporadic disease, with and without various disease features, those with and without statin use). Additional hypotheses were generated, particularly regarding brain permeability and age, which require further study in larger cohorts on nonCCM subjects.
Nevertheless, this is to our knowledge a first demonstration of vascular hyperpermeability in the human brain with autosomal dominant disease, as predicted mechanistically. It includes an effect on brain vascular permeability due to germ line haploinsufficiency in the absence of lesions. It also provides a proof of concept about this measure as a potential biomarker of disease aggressiveness, and could serve as a possible target to calibrate therapies in clinical trials. Beyond CCM disease, endothelial ROCK activity has been postulated as a central mechanism in the aging brain. 33 Thus, our studies of brain permeability optimized and clarified in CCM patients may motivate future research and find broader biomedical applications in the clinical setting.
Footnotes
IAA designed and conceptualized the study. HBWL provide the software for the study. HBWL, XG, and GSC helped optimize study design and permeability technique. AGM, OK, RG, RS, AS, HT, LL, and MAW acquired the data. AGM, OK, LZ, RG, RS, AS, LL, CS, and IAA analyzed and interpreted the data. All authors drafted the work, revised it critically for important intellectual content, gave final approval of the version published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The authors declare no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.