
Abstract
Central post-stroke pain (CPSP) is a neuropathic pain syndrome that often develops in a delayed manner after thalamic stroke. Here, we describe a new model of CPSP by stereotaxic thalamic injection of endothelin-1. Stroke rats (
INTRODUCTION
Central post-stroke pain (CPSP) is a neuropathic pain syndrome characterized by constant or recurrent pain after central nervous system injury. 1 Central post-stroke pain can be triggered by either an ischemic or hemorrhagic infarct at any level of the spinothalamic pathway and its cortical projections often involving the thalamus. 2 Central post-stroke pain is frequently overlooked, and can be misdiagnosed as musculoskeletal pain resulting from paresis and/or muscle tone abnormalities. 3 Epidemiological data are scarce, probably because of the difficulty in interpreting the clinical signs and the variable symptom onset. Thus, CPSP is often perceived as a rare event. 4 However, the true incidence in stroke patients is as high as 8% to 11%. 5
The pathophysiology of CPSP is still poorly understood, and therapeutic options are limited in part owing to a lack of clinically relevant animal models. 6 For example, experimental CPSP models involving thalamic hemorrhage all show acute onset of the pain symptoms,7,8 in contrast to the delayed onset of CPSP several weeks later in patients. 4 To address these shortcomings, we aimed to develop a new experimental model that better mimics the late-onset hypersensitivity seen in CPSP patients. Recently, two clinical reports linked CPSP to more posterior, inferior, and lateral thalamic infarcts, clustering at the ventral posterior thalamic nuclei.9,10 These relay nuclei receive inputs from medial lemniscus, spinothalamic, and trigeminothalamic tracts, and project to the somatosensory cortex where noxious and non-painful, thermal, and mechanical stimuli are processed. We, therefore, targeted the ventral posterior thalamic complex by using stereotaxic microinjections of endothelin-1 to create highly focal ischemic lesions in rats.
MATERIALS AND METHODS
Experiments were approved by the Institutional Animal Care and Use Committee of Massachusetts General Hospital, conformed to the National Institutes of Health ‘Guide for the Care and Use of Laboratory Animals', and carried out in accordance with ARRIVE guidelines. Sprague-Dawley rats (male, 9-10-weeks old, Charles River Laboratories, Wilmington, MA, USA) were randomly allocated, and allocation concealed by a blinded investigator and maintained throughout the study. Sample size was calculated assuming a group difference of 30%, power 90%, alpha 0.05 and an s.d. of 35%, based on pilot behavioral data.
Thalamic infarcts were produced by injection of the potent vasoconstrictor endothelin-1 causing transient ischemia.11,12 Briefly, isoflurane anesthetized rats (4% induction, 2.5% to 2% maintenance, in 70%N2O/30%O2) were placed on a stereotactic frame (Stoelting, Wood Dale, IL, USA), and the body temperature was maintained at 37°C. A burr hole was drilled under saline cooling, and 1 μL of endothelin-1 (0.3 mg/mL, American Peptide, Sunnyvale, CA, USA;
Thermal and mechanical sensitivity and motor deficits were assessed at 1, 2, and 4 weeks, as previously described.11–13 Paw withdrawal latencies to heat were measured according to the Hargreaves's method. A heat beam was applied to the mid-plantar surface of each hindpaw from underneath a glass floor with a projector lamp (Stoelting). Two trials were performed on each paw, by alternating the starting paw, with an interval of at least 5 minutes. A positive pain reaction was defined as sudden paw withdrawal, flinching, and/or paw licking. Paw withdrawal thresh-olds to tactile stimulation were measured using calibrated nylon von Frey filaments (Stoelting; target force: 10, 15, 26, and 60 g). Rats were placed on a wire mesh table and the filaments were applied in ascending order to the plantar surface of each hindpaw, for 1 to 2 seconds with an interval of at least 5 seconds; the stimulus was applied by alternating the starting paw. Only vigorous withdrawal responses were counted; a positive response in three out of five consecutive stimuli was defined as the threshold. In the cylinder test, rats were placed in a transparent plastic cylinder, which the animal rears to explore. The number of wall touches with right, left, and both forelimbs was recorded to count contralateral forelimb contacts expressed as percentage of total forelimb contacts. In the adhesive removal test, rats were gently held by the torso and a 1 × 1 cm piece of surgical tape was placed on the palmar surface of the forepaws. Time to contact and time to remove the tape were obtained from a total of three trials. For the open field test, rats were allowed to freely explore an arena (60 × 60 cm) for 5 minutes; exploratory activity was analyzed using the ANY-MAZE tracking system (Stoelting).
Animals were euthanized after the last behavioral assessment (4 weeks). Fresh-frozen brains were cryosectioned (interval 0.5 mm) and stained with luxol fast blue for myelin, and cresyl violet and hematoxylin and eosin for general histology. Images were acquired using a Super Coolscan 9000 ED scanner and a TE-2000 microscope (Nikon, Melville, NY, USA). Luxol fast blue-cresyl violet-stained sections were imported as TIFF images into Photoshop (Adobe Systems Incorporated, San Jose, California, USA) along with the corresponding coronal templates from a rat brain atlas. 14 The histological images were then manually warped to match the reference template, properly aligning the layers by using well defined anatomical landmarks (i.e., internal capsule and hippocampus). A third layer was used to outline the infarct areas. Infarct was always located between −2.0 and −5.0 mm posterior from bregma. Therefore, we performed lesion mapping and volumetric assessments within this segment. To obtain a probabilistic map of the infarct distribution, the individual infarct outlines on each section level were superimposed and fused along with the reference template. For volumetric assessments, the individual infarct outlines were merged with the corresponding atlas template. The areas of individual thalamic nuclei, internal capsule, and the infarct were quantified by using the ruler on the atlas template as calibration scale. Furthermore, the ischemic injury affecting the individual thalamic nuclei and internal capsule was outlined and quantified as well. The sums of the areas were integrated with the interval between adjacent sections to obtain the volumes.
RESULTS
There was no mortality after endothelin-1 or vehicle injection during the 4-week monitoring, and body weight did not differ between the groups. Baseline assessments did not reveal any difference between the groups or the ipsilateral and contralateral side. After thalamic stroke, the thermal withdrawal latency of the contralateral hindpaw progressively decreased, suggesting reduced thermal pain threshold (Figure 1). Control rats did not show any asymmetry in thermal sensitivity at any time point. Asymmetry index (ipsilateral/contralateral withdrawal latency) was significantly higher in stroke rats compared with controls at 4 weeks. Mechanical pain threshold and performance in cylinder, adhesive removal and open field tests did not change after endothelin-1 or vehicle injection.
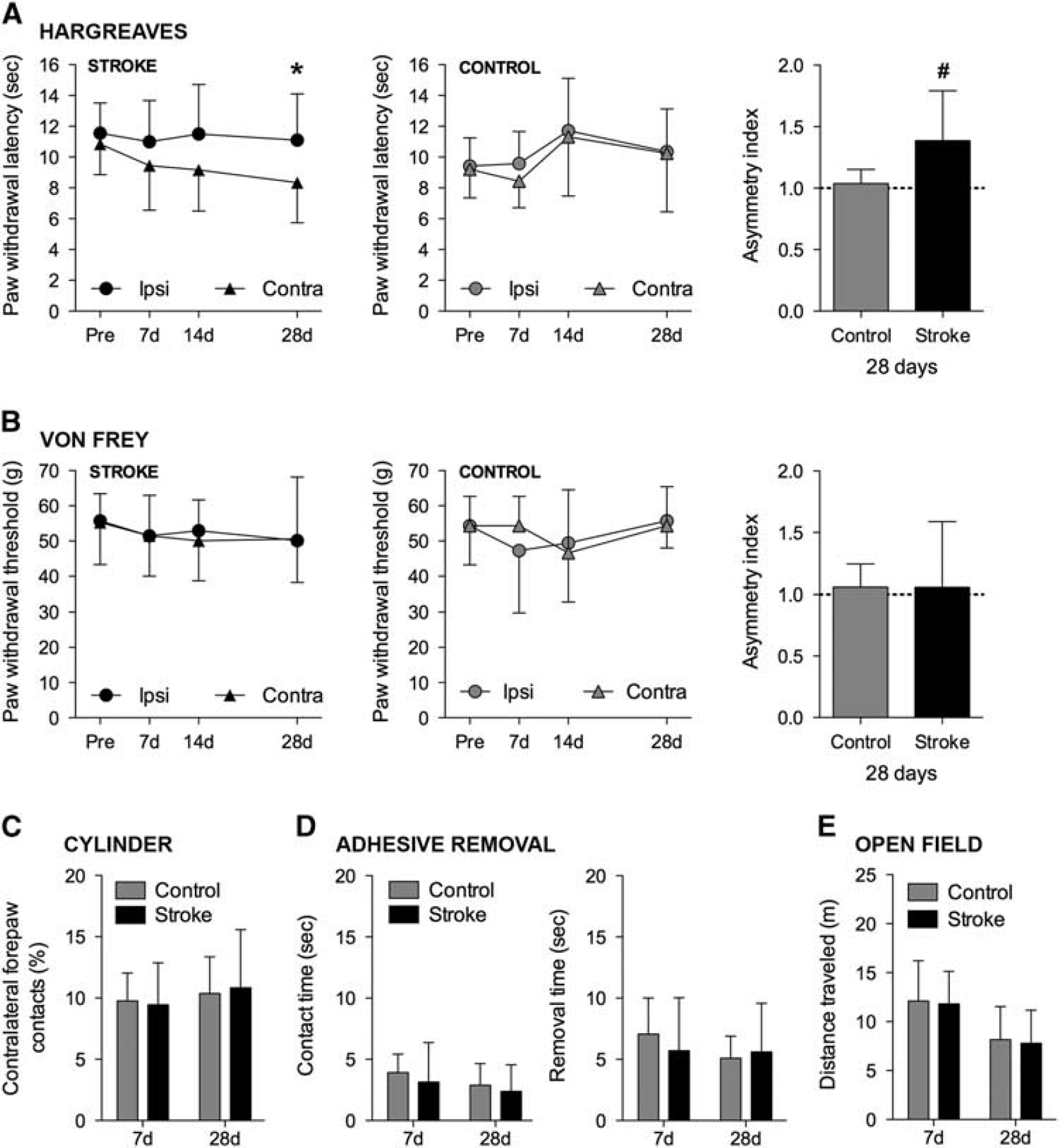
Late-onset thermal hypersensitivity after thalamic stroke. (
Endothelin-1 injection produced a focal infarct in the thalamus (Figure 2), mainly involving the posterior thalamic complex. Ischemic lesion was located within −2.0 and −5.0 mm posterior from bregma, centered between −3.0 and −4.0 mm in all animals. Infarcts were highly focal and reproducible (2.4±0.5 mm3), and affected only ~ 5% of the ipsilateral thalamic volume between the measured antero-posterior range (−2.0 and −5.0 mm). Detailed morphometric analysis showed that the lesion involved 30% to 40% of the total ventral postero-lateral (VPL) and the ventral postero-medial (VPM) nuclear volume, while internal capsule and the adjacent thalamic nuclei were only minimally affected. Indeed, ~70% of the entire lesion was contained within VPL and VPM, with no injury in the cortex, hippocampus, hypothalamus, caudato-putamen, or corpus callosum/external capsule in any of the animals. Vehicle injection did not cause detectable injury.
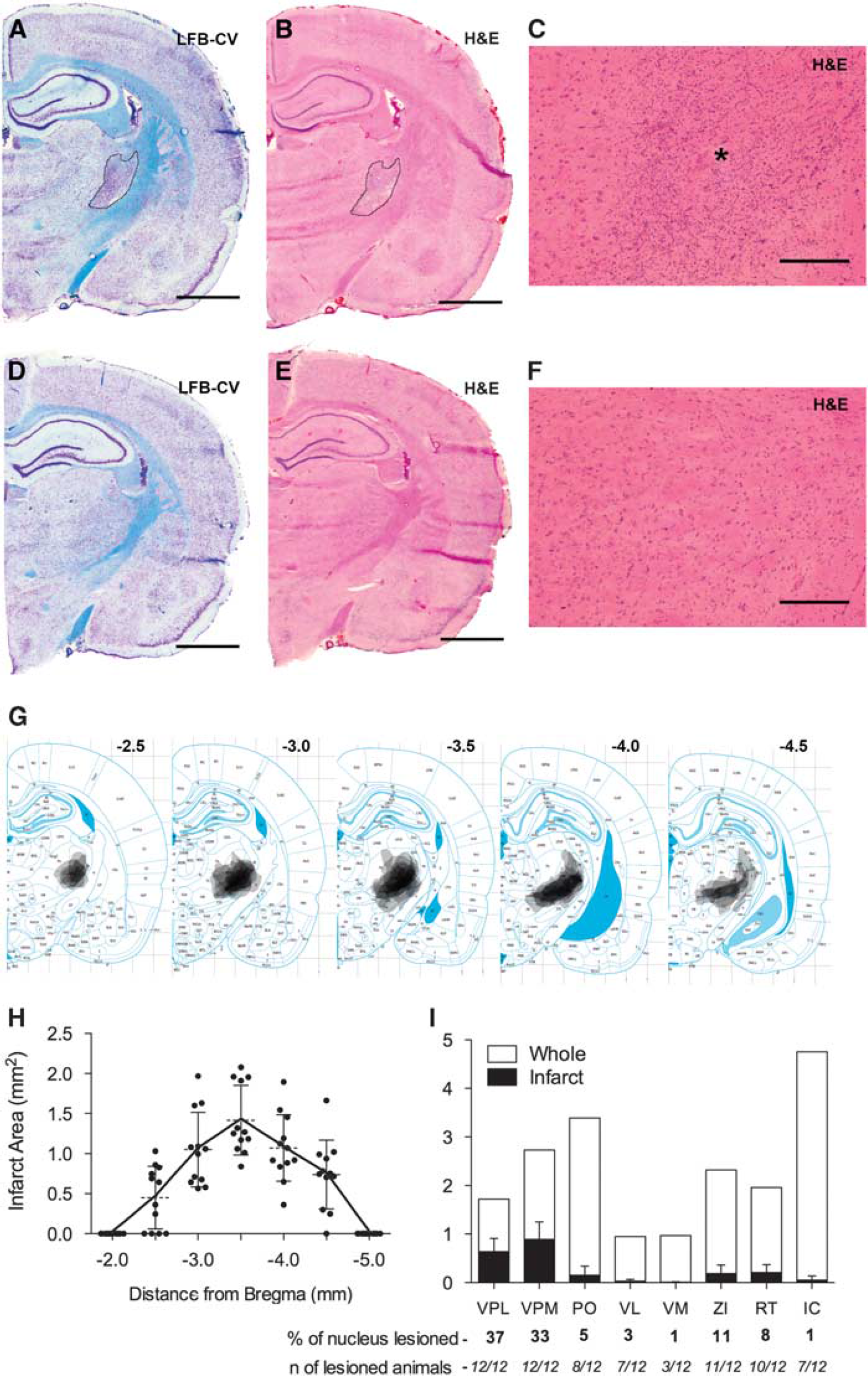
Thalamic infarction 1 month after stroke. (
DISCUSSION
We present a novel experimental model for CPSP after highly focal thalamic infarcts affecting the VPL and VPM nuclei by stereotactic injection of endothelin-1. Stroke rats, but not vehicle-injected controls, develop contralateral thermal hypersensitivity that is progressive over 1 month, without detectable motor or locomotion deficits. The symptom onset and infarct location mimic those commonly observed in CPSP patients.1,4,9,10 Overall, the model recapitulates some of the key-features of human CPSP, and can be useful in facilitating the investigation of CPSP pathophysiology and treatment.
Although neuropathic pain after spinal cord injury has been investigated in the past, CPSP pathophysiology and experimental modeling have received little attention.4,6 Indeed, CPSP after experimental ischemic stroke has never been reported, and previous attempts only featured thalamic hemorrhage or excito-toxic lesions.7,8,15 In thalamic hemorrhage, thermal hypersensitivity was detected at 1 week, the earliest time point tested. Excitotoxic lesions caused hypersensitivity even sooner (24–48 hours). Therefore, results of previous studies were not fully congruent with the clinical observations. Moreover, detailed examination of lesion localization and sensorimotor deficits was not performed, thermal hyperalgesia was not assessed in sham-operated animals, and gait abnormalities were present.
In comparison, our model has several advantages. It mimics the late onset of CPSP in the clinical setting, is not associated with other neurological deficits, and lesions are mainly restricted to VPL and VPM, sparing brain areas that may confound behavioral outcome (i.e., cortex, hippocampus, striatum, and other thalamic nuclei). In addition, because ischemic mechanisms account for > 85% of all strokes, our approach may provide a translational advantage over CPSP models involving hemorrhage or excitotoxic lesions. Our study has limitations as well. We assessed behavioral outcome only for 4 weeks after stroke, and did not characterize cold or chemical hypersensitivity, or allodynia. Although we focused only on the hindlimb in this study, forelimb, torso, head, and whisker pad are probably affected as well considering the involvement of both VPL and VPM. Finally, we didn't observe mechanical hypersensitivity in our model. It is possible that longer follow-up may have been necessary for mechanical hypersensitivity to emerge, the lesion may have affected neuronal networks mediating thermal more than mechanical nociception, or the wide force difference between 26 and 60
In conclusion, we developed a novel animal model of thalamic ischemic stroke characterized by late-onset thermal hypersensitivity. This model may facilitate preclinical investigation of the mechanisms underlying CPSP and thus provide a new experimental medium to test therapeutic interventions targeting recovery and pain management after thalamic stroke.
AUTHOR CONTRIBUTIONS
FB and CA designed the study; FB, FH and CA collected, analyzed and interpreted the data; FB and CA wrote the manuscript; FB, FH, SW, JM and CA revised the manuscript for important intellectual contents.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest