
Abstract
Exercise is a uniquely effective and pluripotent medicine against several noncommunicable diseases of westernised lifestyles, including protection against neurodegenerative disorders. High-intensity interval exercise training (HIT) is emerging as an effective alternative to current health-related exercise guidelines. Compared with traditional moderate-intensity continuous exercise training, HIT confers equivalent if not indeed superior metabolic, cardiac, and systemic vascular adaptation. Consequently, HIT is being promoted as a more time-efficient and practical approach to optimize health thereby reducing the burden of disease associated with physical inactivity. However, no studies to date have examined the impact of HIT on the cerebrovasculature and corresponding implications for cognitive function. This review critiques the implications of HIT for cerebrovascular function, with a focus on the mechanisms and translational impact for patient health and well-being. It also introduces similarly novel interventions currently under investigation as alternative means of accelerating exercise-induced cerebrovascular adaptation. We highlight a need for studies of the mechanisms and thereby also the optimal dose-response strategies to guide exercise prescription, and for studies to explore alternative approaches to optimize exercise outcomes in brain-related health and disease prevention. From a clinical perspective, interventions that selectively target the aging brain have the potential to prevent stroke and associated neurovascular diseases.
Keywords
INTRODUCTION
Strenuous physical activity (e.g., exercise) is the most accessible, effective, pluripotent, and safe intervention to improve and maintain health, as well as treat most modern chronic diseases.1–4 Evidence from randomized controlled trials indicates that exercise is as effective as drug interventions in terms of mortality benefits in the secondary prevention of coronary heart disease, treatment of heart failure and prevention of diabetes, and is more beneficial than drug treatment in stroke rehabilitation. 5 Thus, exercise has a significant role to play in both the prevention and treatment of disease. However, despite its clear benefits, more than one-third of the global adult population, and four-fifths of adolescents, fail to meet current public health guidelines for physical activity6,7 (i.e., ≥ 30 minutes of moderate-intensity exercise on at least 5 days of the week (> 150 min/week), or 20 minutes of vigorous-intensity aerobic exercise training on at least 3 days of the week (≥75 min/week)).8,9 Inactivity appears more prevalent in higher income countries (e.g., 80% of British and 90% of American adults10,11), particularly among the less wealthy, who also comprise the majority of these populations.12,13 Global health statistics highlight ‘physical inactivity’ as a top 10 risk factor for poor health, 14 associated with an increased risk of premature cardiovascular and cerebrovascular mortality.15–18 Therefore, to better harness its health benefits, we need to more effectively establish the underlying mechanisms, and therefore the role of each exercise parameter (intensity, frequency, mode, and duration) in optimizing health and well-being. This knowledge will inform exercise prescription guidelines and allow exploration of alternative approaches to access the health benefits that exercise provides for both healthy and diseased populations.
The benefits of exercise for the brain are becoming increasingly evident but remain poorly understood. Regular exercise promotes angiogenesis, neurogenesis, and synaptic plasticity,19–21 which translate into improved and more efficient cerebral perfusion and metabolism.22,23 Such neural and vascular adaptations contribute to the maintenance of cognitive function, which declines during aging and more markedly in dementia.3,24–26 However, the mechanisms that underpin the neuroprotective benefits of exercise remain to be established, and thus so does the rationalization of exercise parameters. Optimizing exercise to target the aging brain has the potential to prevent stroke and associated neurovascular diseases including dementia, thus reducing the global economic burden associated with the aging population. This is critical given that the societal cost of dementia was estimated at >$600 billion globally in 2010, and in the United Kingdom the cost of dementia alone almost matched the combined costs of cancer, heart disease, and stroke. 27 Urgent implementation of effective countermeasures is critical to fully prepare for the challenges of the world's changing demographics and to create an equitable, affordable, and sustainable aging society for the future. Since there are no curative treatments currently available, major efforts need to focus on prevention, with emphasis on modifiable risk factors such as engagement in physical activity.
CONCEPTUAL FOCUS
In this review, we critically address to what extent high-intensity interval exercise training (HIT) may improve cerebrovascular function, with a focus on the mechanisms and translational impact for patient health and well-being. We begin by highlighting the potential mechanisms by which exercise can improve brain function. Next, we review evidence to illustrate the effectiveness of HIT in healthy and clinical populations associated with impaired brain function. We then discuss the potential danger that HIT may pose to the brain, and how current understanding of cerebral blood flow (CBF) regulation could be used to limit potential risk and inform novel conditioning approaches that target the brain. Finally, we introduce novel interventions that are under investigation as alternative means of accelerating exercise-induced cerebrovascular adaptation, and suggest avenues for future research.
EXERCISE AND THE FUNCTIONAL REGULATION OF CEREBRAL BLOOD FLOW
The regulation of CBF involves complex interactions between brain metabolic and neuronal activity, blood pressure, partial pressure of arterial carbon dioxide (PaCO2), cardiac output, and, perhaps sympathetic nervous system activity
28
(see review by Ogoh and Ainslie
29
). Exercise affects all of these factors and their interactions.
29
Traditionally, CBF during exercise was thought to be unchanged from rest;30,31 however, more recent studies utilizing technologies with greater temporal resolution (e.g., transcranial Doppler and magnetic resonance imaging) have showed that global CBF increases with exercise intensity up to ~ 70% of maximal aerobic power (i.e.,
Increased blood flow elevates mechanical shear stress within blood vessels, which has a beneficial effect on the endothelium via Akt-(protein kinase B) dependent expression of endothelial nitric oxide synthase, NO generation, and complementary improvement of antioxidant defences (reviewed in Bolduc et al 37 ). The increase in vascular NO bioavailability is considered as a key factor in the maintenance of cerebrovascular function and optimal regulation of CBF. While in humans much of this premise has been inferred from studying shear stress-mediated improvement in endothelial function of the systemic vasculature (e.g., via flow-mediated dilation of the brachial artery), 43 extrapolating this to the cerebrovasculature seems reasonable, although with some caveats specific to high-intensity exercise as will be discussed below. Evidence from animal-based and cell-culture studies provides strong support for shear stress-mediated adaptation of the cerebrovasculature (see review by Bolduc et al 37 ). Further, Padilla et al 44 have proposed that alternative signals (i.e., circumferential stretch (cyclic strain), circulating humoral factors) to chronic exercise may act independently or synergistically with shear forces in the modulation of systemic endothelial adaptations in noncontracting tissues (e.g., the cerebrovasculature). Nevertheless, the role of different exercise parameters—and thus blood flow rate/profile—on cerebrovascular endothelium has not been studied. In the systemic vasculature of humans, however, an exercise intensity-dependent response is evident acutely; 45 severe HIT 46 as well as moderate-intensity continuous exercise training (MICT) 47 can improve flow-mediated dilation, and MICT increases arterial compliance whereas resistance exercise reduces it.47,48 Whether such effects translate to the cerebrovasculature is, however, complicated by other effects of intense exercise (see below).
Another key component of exercise is the increased neural activation associated with generating movement. While elevated neuronal activity will increase perfusion to meet metabolic demand (i.e., neurovascular coupling) 49 and thus have an influence in shear stress-mediated adaptation, exercise also activates the expression of genes associated with neuroplasticity and stimulates neurogenesis.50,51 These processes may thus represent a primordial constituent in the positive relationship between exercise and brain health. Different exercise parameters may influence the rate and magnitude of the neural activation, which in turn may alter the vascular response and potentially the signalling stimulus for adaptation (vascular and neural).
Understanding the cellular and molecular basis of exercise-induced neuroprotection is vital for optimizing exercise to improve brain health. Research to date has revealed several key exercise-induced mediators of neurogenesis, synaptic plasticity, and brain angiogenesis (e.g., brain-derived neurotrophic factor (BDNF), VEGF, insulin-like growth factor 1 (IGF-1)), along with their gene-level and humoral modulators (e.g., tropomyosin receptor kinase B, protein kinase C, GluR5, synapsin I, fibronectin type III domain containing 5, irisin; for recent reviews, see Voss et al. 51 and Phillips et al. 52 ). Figure 1 illustrates such proposed local and humoral mediators of exercise-induced adaptation of brain structure and function. Much of the evidence for these cellular and molecular pathways necessarily comes from animal work, thus translation to the human remains speculative. Nevertheless, the role of exercise intensity has received very little attention even in these models, let alone in humans.
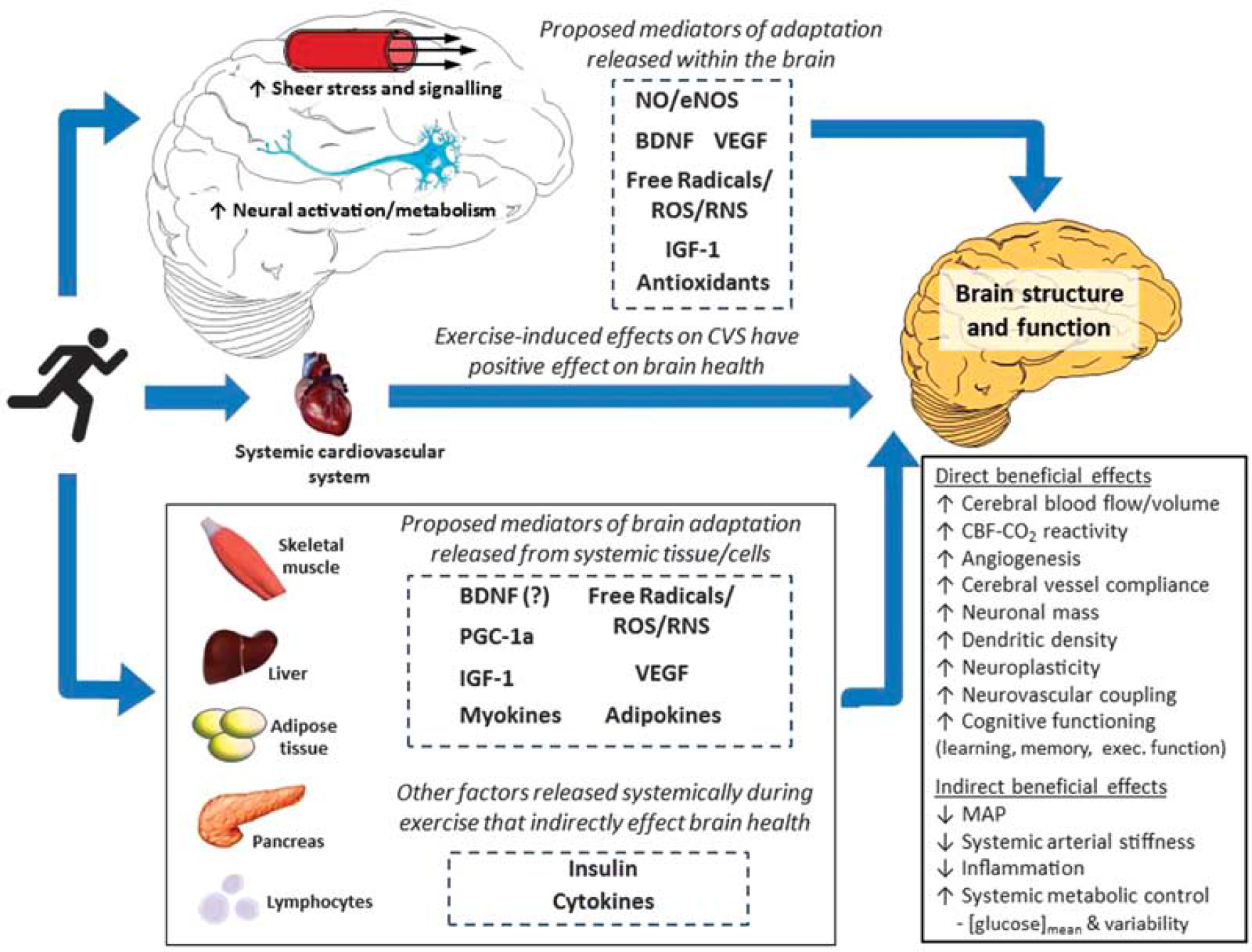
Schematic summarizing proposed mechanisms by which exercise training may alter brain structure and function as well as lower the risk of brain-related dysfunction and disease via alterations in systemic function. BDNF, brain-derived neurotrophic factor; CBF, cerebral blood flow; CO2, carbon dioxide; eNOS, endothelial nitric oxide synthase; IGF-1, insulin-like growth factor 1; MAP, mean arterial blood pressure; NO, nitric oxide; PGC-1α, peroxisome proliferator-activated receptor-γ coactivator; ROS, reactive oxygen species; RNS, reactive nitrogen species; VEGF, vascular endothelial growth factor.
Exercise perturbs redox homeostasis transiently within cells and tissues. While exercise-induced formation of free radicals and reactive oxygen (ROS) and nitrogen (RNS) species was originally suggested to cause structural tissue damage, recent evidence has shown that in physiologically controlled, albeit undefined concentrations, they serve as critical signalling molecules that mediate adaptation.53,54 Radical species upregulate antioxidant enzymes 55 and increase neurotropic factors, such as BDNF, VEGF, and IGF-1.56,57 The Janus Face of exercise-induced oxidative-nitrosative-inflammatory stress reflects a fundamental concept known as hormesis: 58 a toxicological term characterizing a biphasic dose-response encompassing a low-dose stimulation or beneficial effect and a high-dose inhibitory or toxic effect; 59 thus quantifying the impact of each exercise parameter on radical species may be a crucial step in determining the best exercise strategy for optimizing brain structure and function. Accordingly, people with higher baseline oxidative-nitrosative-inflammatory stress (e.g., older or diseased) might benefit from a different prescription of exercise with respect to this mediator of (mal) adaptation.
While this review is focused on the effects of exercise on the brain, an important point to be made is that exercise confers systemic metabolic and immunomodulatory benefits. Indeed, hyperglycemia and diabetes are important risk factors for dementia, 60 and systemic low-grade chronic inflammation is evident in populations with mild cognitive impairment and Alzheimer's disease. 61 Numerous exercise training studies, including those using models of HIT (discussed next), have shown the efficacy of exercise as a tool to lower blood glucose levels, improve insulin sensitivity, and overall glycemic control, as well as reduce neuro-inflammation (see Figure 1).
HIGH-INTENSITY INTERVAL EXERCISE TRAINING; AN EMERGING PARADIGM
There is a burgeoning interest in HIT as an alternative means of improving health, motivated in part by the need to combat the perceived and frequently reported ‘lack of time’ barrier associated with traditional exercise guidelines, which promote MICT.62,63 There are various forms of HIT,64,65 but it generally involves repeated bouts of relatively brief intermittent exercise, often performed at an intensity close to (~85% to 95%) or beyond maximal aerobic power.66,67 Two examples of the HIT profile are illustrated in Figure 2.
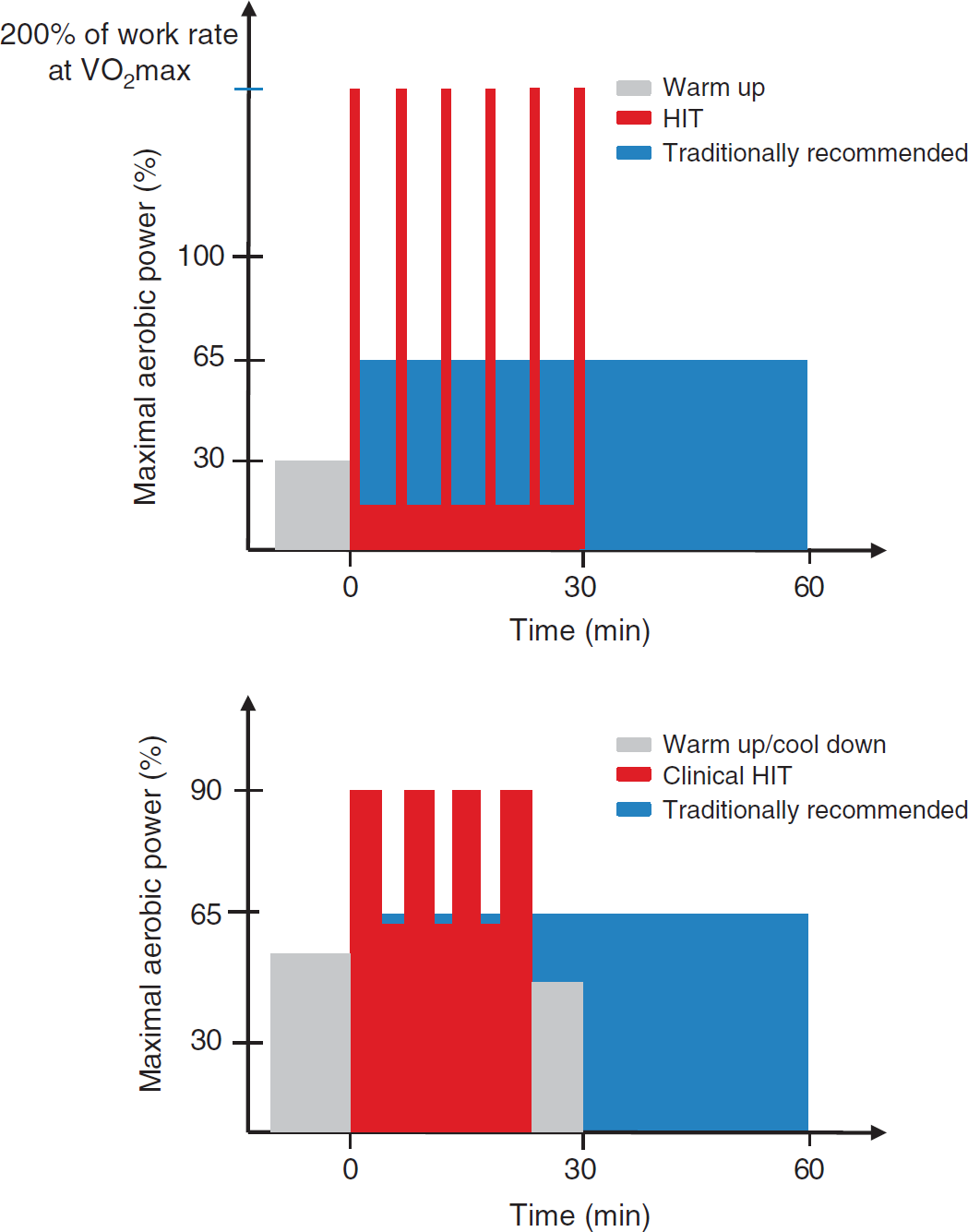
Top panel: Schematic comparing high-intensity interval exercise training (HIT) against traditional exercise guidelines recommended by leading health agencies (e.g., World Health Organization
8
and American College of Sports Medicine
9
). The HIT protocol illustrated here consists of 6 × 30-second all-out cycling efforts separated by 4.5 minutes of active recovery at very low intensity (e.g., 30 W). This HIT protocol is typically performed three times per week, while exercise training under the traditional model consists of continuous moderate intensity cycling at 65% of maximal aerobic power (
Compared with traditional MICT, emerging evidence indicates that HIT provides equivalent if not indeed superior metabolic, cardiac, and systemic vascular adaptations, thereby supporting more time-efficient approaches to optimize metabolic and cardiovascular health (e.g.;64,68–77 see Figure 3). Such studies have provided mechanistic support for the epidemiologic observations that intensity of exercise appears more important than its duration in preventing cardiovascular disease.78,79 High-intensity interval exercise training has also been shown to be more effective than traditional exercise interventions for cardiac function in various diseases for which there was major concern regarding its safety and appropriateness.64,72 The evidence to date in the cardiac rehabilitation setting indicates a low risk for acute adverse cardiovascular events during HIT, albeit perhaps ~ 5 times higher than that observed during MICT (1 event per 23 182 hours of HIT exercise versus 1 event per 129 456 hours of MICT
80
). Further, a recent meta-analysis of HIT studies in patients with lifestyle-induced chronic cardiometabolic disease (coronary artery disease, heart failure, hypertension, metabolic syndrome, and obesity) reported no adverse events related to the exercise training, and revealed that HIT provided almost twice the improvement in cardiorespiratory fitness (i.e.,
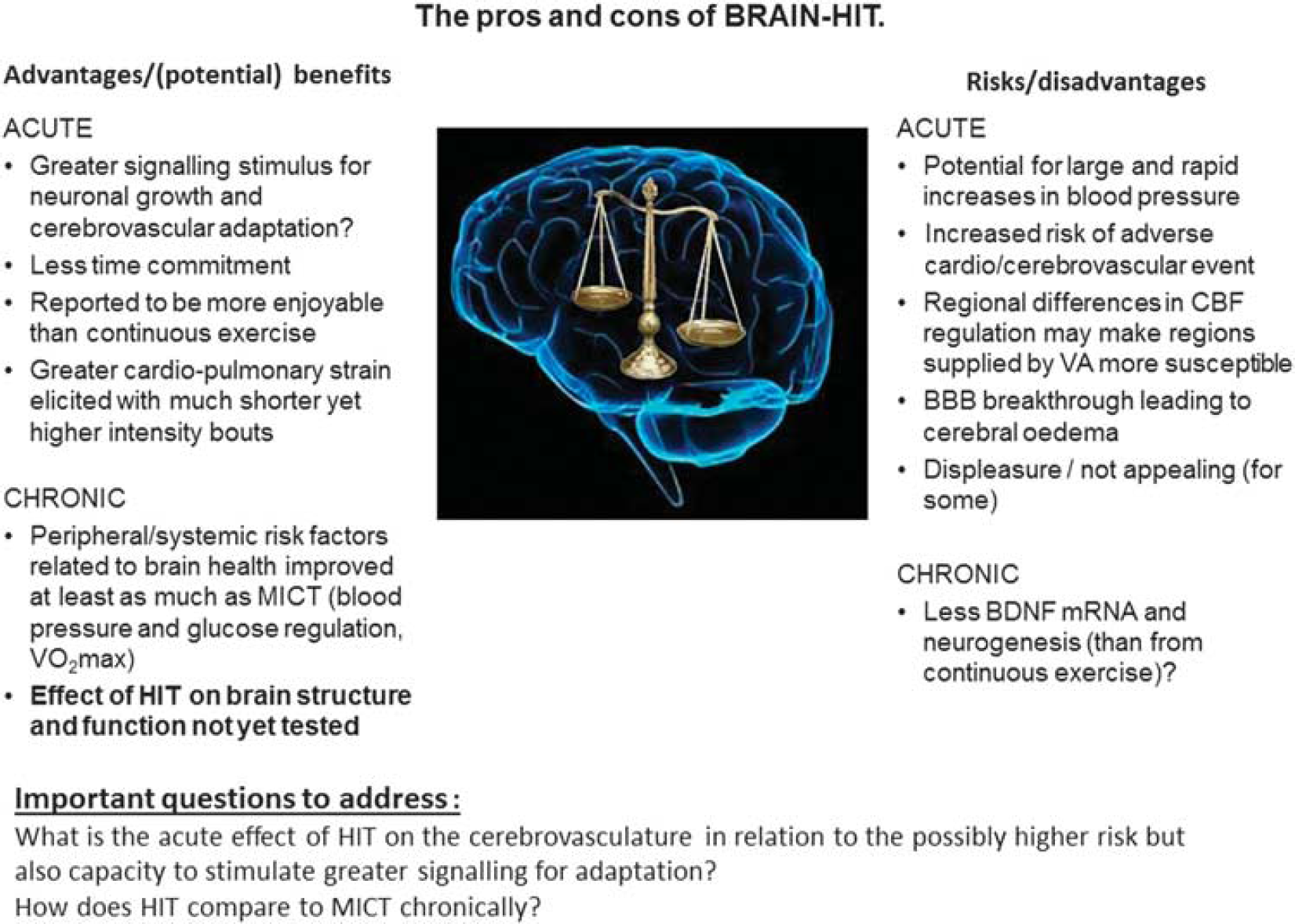
The pros and cons of BRAIN-HIT. BBB; brain–blood barrier; BDNF, brain-derived neurotrophic factor; CBF, cerebral blood flow; HIT, high-intensity interval exercise training; MICT, moderate intensity continuous exercise training; VA, vertebral arteries;
DOES HIGH-INTENSITY INTERVAL EXERCISE TRAINING POSE A DANGER TO THE BRAIN?
Exercise is not risk free; elevated exercise intensity in unscreened and potentially ‘at risk’ populations carries an increased risk acutely, particularly in sedentary adults.81,82 As mentioned above, this is a large proportion of the population in many countries. Furthermore, while a functional diagnostic 12-lead electrocardiogram exercise stress test exists to screen for cardiovascular abnormalities, an equivalent, universally-accepted screening process for the cerebrovasculature is lacking; thus, the development and clinical implementation of a brain-specific test could further optimize both health and safety for the brain before undertaking any exercise training program, let alone HIT.
The potential dangers of HIT to the brain are not trivial since high-intensity exercise has the capacity to elicit rapid and potentially damaging increases in systemic blood pressure that may be transmitted to the brain.83,84 Unless countered by the neuroprotective influences of sympathetic activation or cerebral autoregulation (CA; see later), this potentially increases the risk of hyperperfusion injury predisposing to stroke or blood–brain barrier (BBB) breakthrough. 85 This risk has been well publicized in the media in the United Kingdom recently, due to a high-profile clinical case of a BBC journalist claiming that the stroke suffered was caused by ‘HIT’ while exercising on a rowing ergometer.86,87 While certainty about cause-and-effect is difficult to establish, a clinical case study such as this highlights the potential safety issues associated with the HIT paradigm for the brain.
Without evidence examining the effects of HIT on the brain, any answer to the question of safety can be supported only by case studies and speculation. Ironically, the metabolic and cardiovascular efficacy of HIT was implied from studies with animals and healthy individuals mostly before being tested in metabolic- and cardiovascular-diseased populations, whereas patients with brain-related pathology have already begun using HIT-based protocols despite the lack of evidence of its cerebrovascular efficacy; e.g., in stroke rehabilitation (reviewed in Boyne et al. 65 ) and Parkinson's disease. 88 While no adverse events have been reported in studies assessing HIT for stroke rehabilitation (no events in 294 recorded HIT exercise hours among 41 patients with stroke; see Boyle et al. 65 ), there are too few studies to make firm conclusions supporting the clinical implementation of HIT for stroke rehabilitation, let alone other brain-related pathologies. Nevertheless, the functional benefits (e.g., improved gait speed, stride length and cadence) reported by such studies are encouraging—some of which show greater improvement than traditional MICT protocols. 89 Further, given the relationship between heart disease and stroke (heart disease in ~ 75% of patients who suffer a stroke 90 ), the implementation of HIT in cardiovascular disease populations means that patients with potentially undiagnosed cerebrovascular pathology may already be benefiting from HIT, if indeed it is beneficial for cerebrovascular function.
In summary, the obvious and exciting positive effect(s) that HIT has shown for metabolic and cardiovascular adaptations has led to promotion of this exercise strategy among the general population and use in some clinical populations. While in general, any form of physical activity should be encouraged, it seems premature to promote HIT for better whole-body health without clear and comprehensive supporting evidence, particularly given the lack of research focused toward cerebrovascular adaptation. Nevertheless, while there is limited information documenting the impact of HIT on acute and chronic brain health, given the clear metabolic and cardiovascular benefits shown in healthy and diseased populations, abandoning or delaying the implementation of such a potentially effective strategy to optimize health is equally misplaced. Indeed, even with the potential elevated risk of an acute cardiovascular or cerebrovascular event, the health gains and cost savings in the longer term arguably outweigh potential risks, at least on a population-wide scale. Figure 3 presents a summary of the ‘pros and cons’ of HIT for the brain. Notwithstanding the absence of clear evidence examining the impacts of HIT on the brain at the moment, current knowledge of CBF regulation can be applied to help optimize strategies for cerebrovascular adaptation and brain safety during training.
OPTIMIZING CEREBROVASCULAR ADAPTATION AND SAFETY FOR HIGH-INTENSITY INTERVAL EXERCISE TRAINING
In the context of HIT, it is important to note that the response of the cerebrovasculature to exercise is different from that of the peripheral vasculature.
91
While increased perfusion during high-intensity exercise is one likely mediator of improved systemic vascular function (as detailed above), exercising above ~ 70%
It is important to note that this constrictive effect triggered by hyperventilation-induced hypocapnia during higher exercise intensities may differ depending on the brain region. Sato et al.
97
identified that flow in the posterior circulation (measured via the vertebral artery (VA)) increased further at 80% than at 60%
The effect of the systemic circulation on CBF is also important to consider.83,91 CA requires ~ 5 seconds to initiate its protective influence; 101 therefore, explosive HIT protocols could expose the cerebrovasculature to potentially damaging increases in perfusion pressure, particularly in diseased populations with impaired autoregulation (e.g., diabetes, 102 hypertension, 103 and Alzheimer's disease 104 ). Furthermore, intense exercise can increase BBB permeability subsequent to a free radical-mediated impairment in CA, rendering the brain more susceptible to overperfusion and extracellular (vasogenic) edema; which has been shown to occur even in response to a more graduated incremental exercise test to exhaustion. 85
The direct effect of sympathetic nervous activity (SNA) on the cerebrovasculature remains controversial28,105,106 and is further complicated in humans by the common inference of global SNA measures reflecting cerebral effects (e.g., via microneurography of SNA in the peroneal nerve versus noradrenaline spillover measurements 107 ). In fact, studies in sheep have indicated an inverse relationship between global and cerebral SNA;108,109 thus, increases in muscle SNA may be reflected in a lowering of cerebral SNA. 110 Nevertheless, HIT will presumably elicit large increases in cerebral SNA that may act to restrict rapid increases in CBF as a consequence of the surge in blood pressure associated with high-intensity exercise. 111 The asymmetrical CBF changes in response to acute hypertension compared with acute hypotension have been attributed, in part, 112 to a SNA-mediated role in CBF regulation.108,113,114 Such a role may be vital in limiting hyperperfusion injury during HIT before CA is effective, particularly in populations with autonomic dysfunction who display impaired CBF regulation. 115 With this knowledge at hand, a graduated increase in exercise intensity over the first 10 seconds may limit this hyperperfusion risk by ‘priming’ the cerebrovasculature. Indeed, the HIT exercise used in the stroke rehabilitation studies reviewed by Boyne et al. 65 used an incremental ramp during the initial 1 to 2 minutes of the bout. Whether the prolonged nature of this increase in intensity influences the adaptive processes, notably mechanical shear stress or consequent signalling, is unknown. Regional differences in CA have also been reported,116,117 with that of the VA being lower than the ICA and MCA (reviewed in Ainslie and Brassard 118 ). Therefore, impaired buffering of blood pressure during high-intensity exercise may further explain why flow is elevated in the posterior circulation during high-intensity exercise. Regions of the brain directly supplied by the VAs (e.g., midbrain and cerebellum) may therefore be more susceptible to hyperperfusion injury during HIT.
Sato et al.
97
also showed that the high intensity-induced reduction in ICA flow was correlated to both the relative hypocapnia and the increased flow in the external carotid artery.
97
This redistribution to the external carotid artery was suggested to illustrate that brain and head thermoregulation have higher priority for CBF regulation during heavy exercise, which is in contrast with what happens at rest during passive heating, where no regional differences are apparent and the reduction in anterior flow is mediated by reductions in end-tidal PCO2 and unrelated to increased external carotid artery flow.
119
From a teleological perspective, this thermoregulatory mediated response may also serve as a neuroprotective mechanism during HIT, diverting a proportion of the elevated blood flow away from the cerebral tissue, thus attenuating the increased cerebral perfusion pressure and risk of injury to the brain. Clearly this may also have consequences for oxygen and nutrient delivery to the neurons supplied by the ICA; however, the interconnectedness between the posterior and anterior cerebral circulations via the Circle of Willis may mean that some of this reduction in ICA flow is compensated for by the VA.
97
Whether such differential responses occur during short HIT bouts is unknown (Sato et al. used 5-minute steady-state intensities up to 80%
One more factor that can influence CBF during intense exercise is the Valsalva maneuver (VM), which initially raises blood pressure and CBF 120 (identified as phase I of the maneuver) and thus raises the risk of an adverse event; hence the clinical recommendation to avoid VMs during resistance training. 121 Paradoxically, however, the VM may also help protect against hyperperfusion injury when large abrupt increases in blood pressure are expected (e.g., ‘super HIT exercise’ for very short (~5 to 10 seconds) durations), as recently demonstrated for CBF velocity responses during load-dependent increases in blood pressure during weightlifting exercise 122 and with graded VM alone. 123 Though hyperperfusion may be constrained while performing the VM (phase I), presumably via elevated intracranial pressure ‘clamping’ the cerebral vessels, releasing the VM elicits cerebral hypoperfusion and increases the risk of fainting, particularly if upright. 124 Alternatively, this transient hypoperfusion and resultant hypoxemia may stimulate further adaptation via activation of oxygen-sensitive genes orchestrated by hypoxia-inducible factor 1-α that serve to salvage cerebral oxygen transport. Therefore the many factors affecting CBF during intense exercise are complex for both acute risks and adaptive stimuli.
Finally, avoiding certain exercise modes for HIT may limit the risk of cerebrovascular injury. For example, rowing elicits stroke-by-stroke fluctuations in blood pressure and CBF,
125
and the biomechanical motion of rowing provokes changes in respiratory mechanics including timing of breaths during the stroke,
126
which has been shown to uncouple the CBF response from the normal hyperventilation-induced hypocapnic lowering of CBF above 70%
OPTIMIZING CEREBROVASCULAR ADAPTATION THROUGH BRAIN-TARGETED TRAINING INTERVENTIONS
Can interventions be tailored to maximize cerebral perfusion and optimize adaptation? In this final section, we consider strategies and discuss emerging interventions with the capacity to maximize cerebrovascular adaptation.
Elevations in shear stress can be stimulated by simple maneuvers such as repeated squat-to-stand maneuvers, which result in oscillating blood flow within a safer (i.e., lower) autoregulatory range of blood pressure as well as potentially stimulating a mechanical stress-mediated adaptive response for the cerebrovascular endothelium (see above). Recently this concept has been illustrated via water immersion, where CBF increases in a similar magnitude to that obtained during land-based exercise, 128 and more so when water immersion was combined with exercise. 129 How this then translates to longer-term effects (i.e., after a training intervention) has not yet been reported, but the combined strategy may result in greater improvements in cerebrovascular function than previously reported from a standard land- and aerobic-based training study. 130 Such a training strategy may be a powerful adjunct to increase the shear-stress stimulus for clinical populations with impaired mobility as a consequence of injury (e.g., hip fracture) or large body mass (e.g., obese).
The neurovascular coupling relation within the brain means that particular movements can stimulate region-specific increases in CBF, that when combined could optimize global CBF (if performed at an appropriate intensity); e.g., combining handgrip exercise with lower-limb cycling. This neurovascular effect need not be restricted to motor output for various muscles, with somatosensory input potentially contributing to even greater elevations in CBF (particularly from those areas with greater representation in the cortex; e.g., face and hands). Consistent with this concept, a recent Cochrane Review has argued that a combined multimodal (aerobic and motor) intervention may compound cerebrovascular adaptation and improve cognitive function. 131 Using such an approach, Vaughan et al. 132 showed medium-to-large improvements in cognitive function, relative to the smaller effects reported from previously-employed single or bimodality exercise interventions.
This larger-scale activation type of approach makes intuitive sense given that motor fitness training requires additional sustained mental effort and the corresponding cognitive load is inherently greater. This is likely to engage higher-order cognitive processes that activate the prefrontal cortex, an area of the brain that is especially vulnerable to early declines associated with aging and inactivity. 133 Whether such improvements are coupled with increased CBF and vascular reactivity are unknown. A higher CBF and vascular reactivity outcome seems tenable given the established links between habitual physical activity, improved cognition, and increased availability of neurotrophins and growth factors in the brain that facilitate neurogenesis, synaptic plasticity, and angiogenesis,134,135 which as outlined above, may underpin the improved brain vascular function. 136 Further, recent findings in both young 137 and older 138 adults indicate that vascular reactivity may mediate the positive exercise-cognition relation. Interestingly, in the context of this review, a dose-response relationship between exercise intensity and cognitive function has been reported,139,140 which provides some rationale to test the hypothesis that HIT may prove an optimal strategy to improve cognitive function.
Thus, a different approach may be necessary when ‘training the brain’ to optimize vessel adaptation and improve function. There is an urgent need to develop optimal and appropriate interventions that will target key mechanistic pathways linked to improved vascular and brain function; interventions that could supplement or indeed replace current exercise-based conditioning practices for whole-body health. High-intensity interval exercise training may prove one such strategy though the safety concerns and its mechanistic basis requires a great deal more scientific and clinical support (see Figure 3). While we have suggested some alternatives here, this list is by no means exhaustive of potential alternative or adjunct conditioning strategies. Other possibilities include: heat and hypoxia conditioning, repetitive brain stimulation (e.g., via transcranial magnetic stimulation), as well as combined nutritional and exercise-based protocols (e.g., flavonoid containing products). Future research is required to test the efficacy and effectiveness of such approaches on brain health (and whole-body health).
Figure 4 illustrates how exercise and other conditioning strategies may lead to beneficial adaptation of brain structure and function. A vital concept highlighted within this figure is the link between the stress imposed by an intervention and the physiologic strain that it induces. Specifically, it is the resultant strain from the stimulus (or combination of stimuli) that mediates the release of humoral and metabolic signals from various cells, tissues, and organs (see Figure 1) that then drives the molecular sensing and transcription that underpins the exercise-induced adaptation of brain structure and function. Research is needed to identify the optimal dose and combination of stimuli, as well as the processes that mediate the adaptation for such interventions. We have suggested some possible candidates that may be involved in this process based on cell culture and animal-based studies (mentioned above), as well as human-based work examining the mechanistic underpinning of vascular adaptation in the systemic circulation. Work is required to establish whether these are the pathways through which exercise and other conditioning strategies bring about positive adaptation for brain structure and function, as well as determining which intervention or combination of stimuli bring about optimal changes in brain health and which may be different depending on age, clinical status, and/or genetics. Clearly, this is a difficult but important field for future research, which may produce some unusual lifestyle interventions for optimizing brain health.
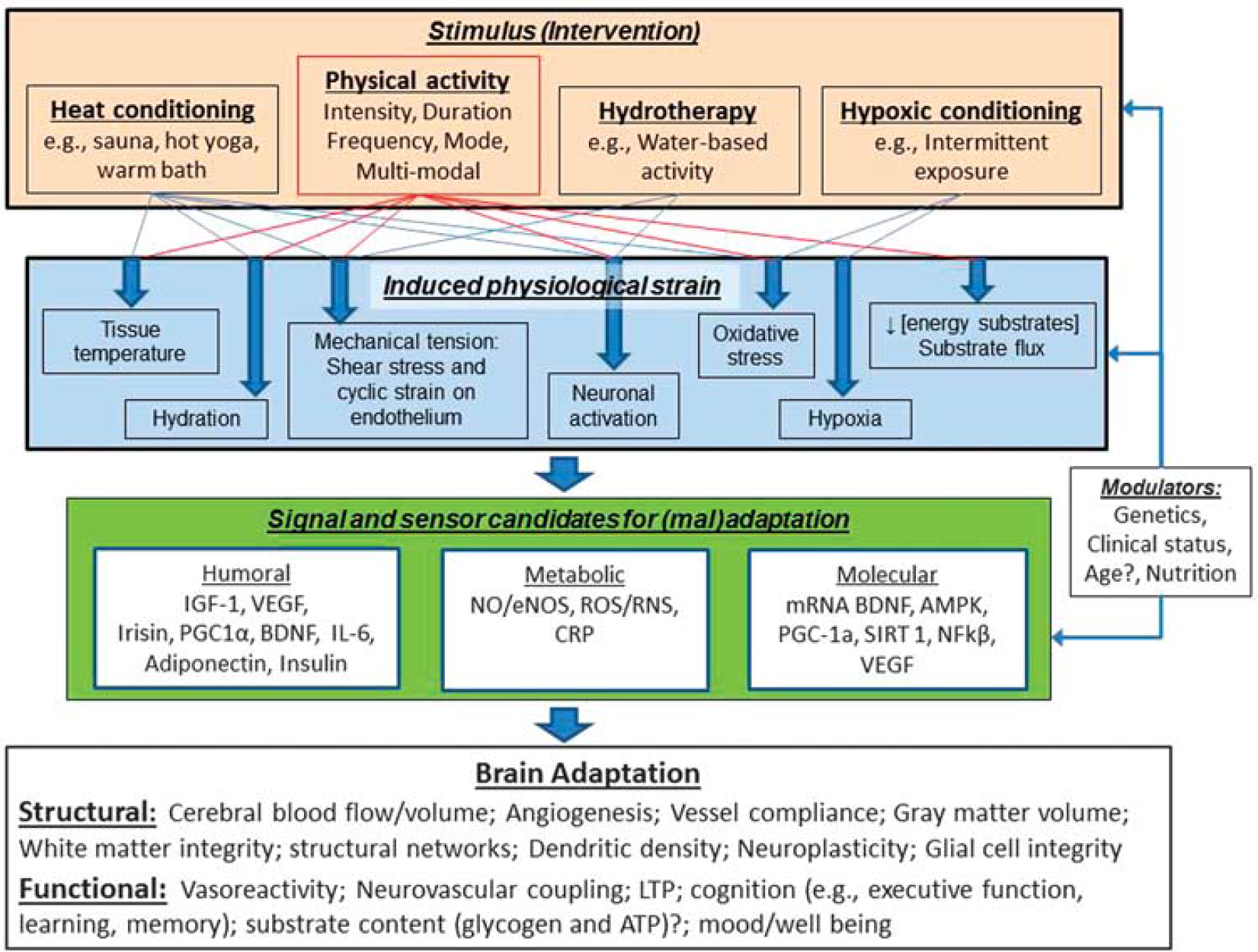
This figure illustrates the potential pathways through which the components of physical activity (intensity, duration, mode, and frequency) as well as other conditioning strategies may lead to beneficial adaptation of brain structure and function. Note that the interventions/stimuli can be applied individually or in combination, and the induced physiologic strain and integration of humoral, metabolic, and molecular signalling, sensoring and transcription may be modulated by individual characteristics (age, sex, and clinical status) and/or other factors (e.g., nutritional supplements) to influence the nature of brain structure and function adaptation. AMPK, AMP-activated protein kinase; BDNF, brain-derived neurotrophic factor; CRP, C-reactive protein; eNOS, endothelial nitric oxide synthase; IGF-1, insulin-like growth factor 1; IL-6, Interleukin 6; LTP, Long-term potentiation; NFkβ, nuclear factor kappa B; NO, nitric oxide; PGC-1α, Peroxisome proliferator-activated receptor-γ coactivator; RNS, reactive nitrogen species; ROS, reactive oxygen species; SIRT 1, Sirtuin 1; VEGF, vascular endothelial growth factor.
CONCLUSIONS AND RECOMMENDATIONS FOR FUTURE RESEARCH
High-intensity interval exercise training for metabolic and cardiovascular health appears generally comparable if not indeed superior to the gains incurred after traditional low-to-moderate intensity continuous exercise interventions. However, to what extent HIT impacts cerebrovascular function acutely or adaptively and the corresponding implications for cognitive function remain unknown. Research is urgently needed to address this imbalance and provide clinical practitioners with objective, evidence-based recommendations to promote safe practice and effective conditioning strategies to optimize brain health. Ideally, this evidence would come in the form of randomized controlled trials examining the effectiveness of HIT versus MICT in the short term. Overall, research is required to establish the optimal exercise strategy for the brain as well as the usefulness of alternative and adjunct strategies that might mediate beneficial adaptation, and the underlying mechanisms involved, to optimize brain function across the lifespan. Optimizing interventions that target key mechanistic pathways linked to improved vascular and brain function could ultimately protect against and/or treat cognitive decline and brain vasculature-related neurodegenerative diseases, and thus reduce the looming global economic burden that is projected to cost billions in the years to come.
AUTHOR CONTRIBUTIONS
SJEL, JDC, PB, and DMB all contributed to the drafting of the manuscript and made critical revisions thereof. All authors have read and approved the final manuscript.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.