
Abstract
Derangements in cerebrovascular structure and function can impair cognitive performance throughout ageing and in cardiometabolic disease states, thus increasing dementia risk. Modifiable lifestyle factors that cause a decline in cardiometabolic health, such as physical inactivity, exacerbate these changes beyond those that are associated with normal ageing. The purpose of this review was to examine cerebrovascular, cognitive and neuroanatomical adaptations to ageing and the potential benefits of exercise training on these outcomes in adults 50 years or older. We systematically searched for cross-sectional or intervention studies that included exercise (aerobic, resistance or multimodal) and its effect on cerebrovascular function, cognition and neuroanatomical adaptations in this age demographic. The included studies were tabulated and described narratively. Aerobic exercise training was the predominant focus of the studies identified; there were limited studies exploring the effects of resistance exercise training and multimodal training on cerebrovascular function and cognition. Collectively, the evidence indicated that exercise can improve cerebrovascular function, cognition and neuroplasticity through areas of the brain associated with executive function and memory in adults 50 years or older, irrespective of their health status. However, more research is required to ascertain the mechanisms of action.
Introduction
The current worldwide incidence of dementia is more than 50 million people and is expected to treble in the next 30 years.1,2 Dementia is associated with adverse changes in cerebrovascular structure and function, which contribute to a decline in cognition.3–5 The greatest risk factor for developing dementia is advanced age. 1 However, there are various modifiable risks factors that lead to impaired vascular function and contribute to dementia. These include behavioural risk factors (limited educational engagement, physical inactivity and excessive alcohol consumption), metabolic risk factors (obesity, hypertension, dyslipidaemia, hyperglycaemia and homocysteinaemia) and cardiovascular diseases (coronary heart disease, heart failure, arrhythmia, stroke, diabetes and renal disease).6–16 Of these, low-level educational engagement, chronic renal disease, diabetes mellitus, hypertension and physical inactivity account for the largest degree of dementia burden globally, particularly in developed countries such as Australia.2,17 These modifiable risk factors are associated with and characterised by endothelial dysfunction, 18 which can impair cerebrovascular function. This, in turn, may promote the development of cerebral dysfunction, cerebral pathology, impaired cognition (in addition to the age-related decline) and eventually a neurodegenerative disease state such as dementia (Figure 1). 18
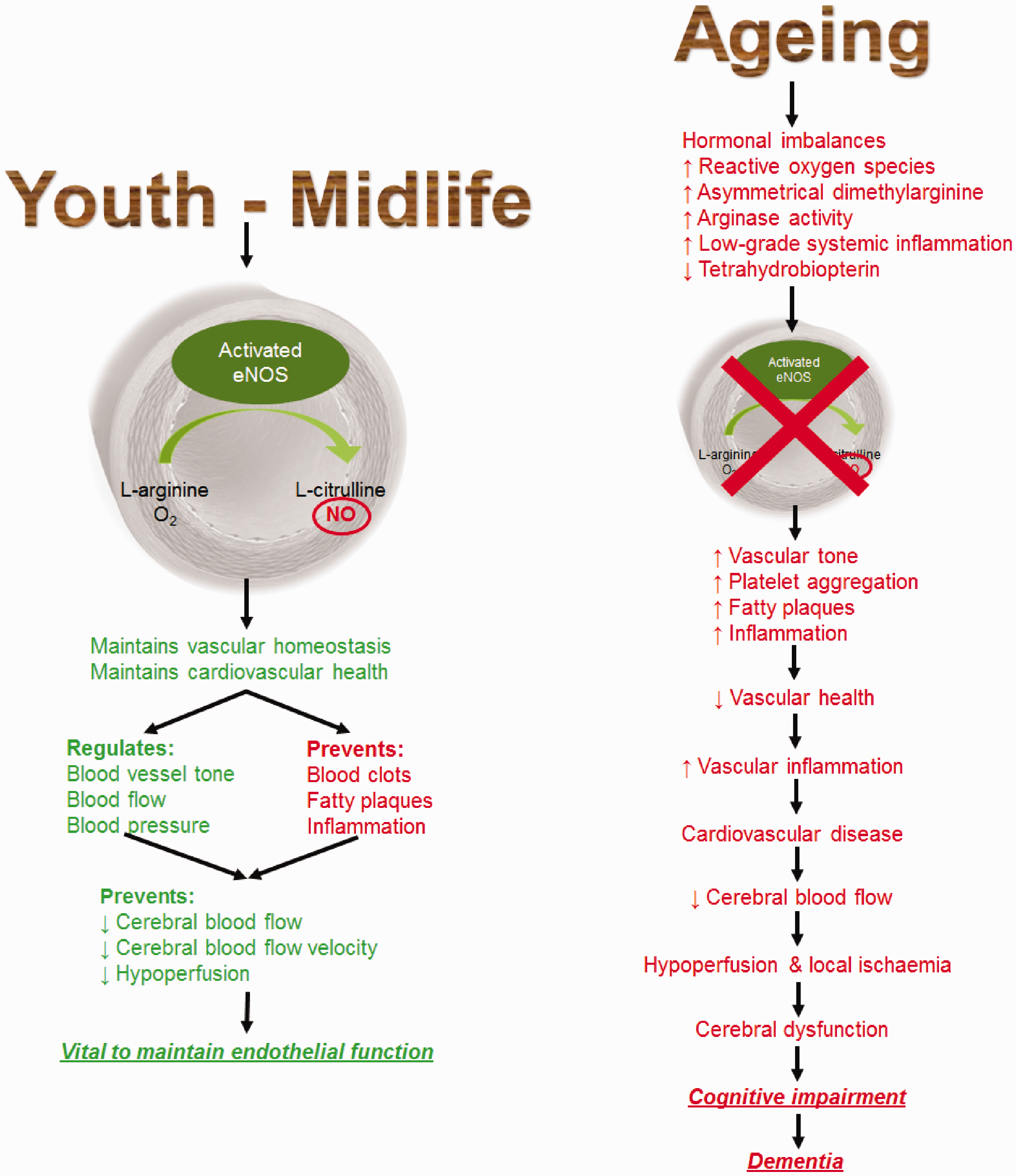
Ageing is associated with hormonal imbalances and increased low-grade systemic inflammation. It is also associated with the increased production of reactive oxygen species (ROS), which may be due to diminished nuclear regulation factor 2 and superoxide dismutase expression and increased expression of nicotinamide adenine dinucleotide phosphate oxidase complexes, resulting in increased mitochondrial superoxide production.
120
Uncoupled endothelial nitric oxide (NO) synthase (eNOS) increases superoxide production by catalysing nicotinamide adenine dinucleotide phosphate, instead of synthesising NO. Increased arginase activity reduces
There is increasing evidence that exercise training may help to maintain optimal cerebrovascular function and thereby prevent or slow the development of cognitive impairment.19–47 Currently, there are limited randomised controlled studies examining the effects of exercise training on cerebrovascular function and its association with cognitive function in middle-aged and older adults, as both should be interpreted together and not as separate functions. The purpose of this review is to examine the benefits of exercise training on cerebrovascular and cognitive function in ageing. Firstly, we will review the impact of ageing on cerebrovascular function, cognition and structural changes within the brain. Secondly, the effects of aerobic exercise training (AT) and resistance exercise training (RT), alone and in combination, on structural adaptations, cerebral blood flow (CBF) and cognition in middle-aged and older adults will be discussed. Thirdly, we will determine if there are any published randomised control trials examining the association between CBF and cognition function in this cohort. Finally, we will discuss why cerebrovascular structure and function and cognition may change following exercise training.
Methods
This review implemented the procedures and following the guidelines outlined in the Peer Review of Electronic Search Strategies: 2015 Guideline Statement. Appropriate literature was searched for systematically using seven databases (PubMed, CINAHL, Cochrane, Science Direct, Web of Science, Scopus and MEDLINE) to explicitly find, select, evaluate and interpret relevant research, as well as Google Scholar as a method to ensure completeness. 48 The inclusion criteria were that original articles must be written in English, peer-reviewed, describe a cross-sectional study or an intervention trial in middle-aged or older adults (≥50 years old) and include the use of exercise (aerobic, resistance or multimodal). In this review, we defined AT as training performed over months and years, which comprises repeated bouts of exercise that primarily utilise energy produced via aerobic respiration, such as running, cycling and swimming. RT is defined as repeated bouts of muscle contraction against an applied force or resistance, which primarily aims to improve muscular strength, endurance, size and definition. Multimodal or combined exercise training (CT) is defined as the combination of at least two different forms of exercise training, such as AT and RT. The search terms used were: exercise (including physical activity or exercise training), ageing, blood–brain barrier (BBB), CBF, CBF velocity (CBFv), cerebral perfusion, cerebral volume (whole brain and specific regions such as the hippocampus), neuroplasticity, cognition, transcranial Doppler (TCD) ultrasonography, magnetic resonance imaging (MRI) and arterial spin labelling (ASL).
The search was completed by April 2019 and included all studies conducted up until this period. An updated search was performed prior to submission of the article in February 2020, with limited results being returned other than those who have published method papers with results still pending. Additionally, a search was performed on the International Clinical Trials Registry Platform. It was found that there were over 34 registered trials in this field of research, which were about to commence, are ongoing or due to be completed by the end of 2020.
After removing duplicates, those identified were screened initially by title then abstract and, if deemed suitable, were read in full and included in the review. Further, the reference lists of suitable articles were screened to ensure completeness. The studies identified for inclusion in the review have had their primary and secondary results tabulated and their primary results described narratively. Knowledge gaps and future directions of research were identified based upon the findings of these studies.
Age-related cognitive decline and structural changes
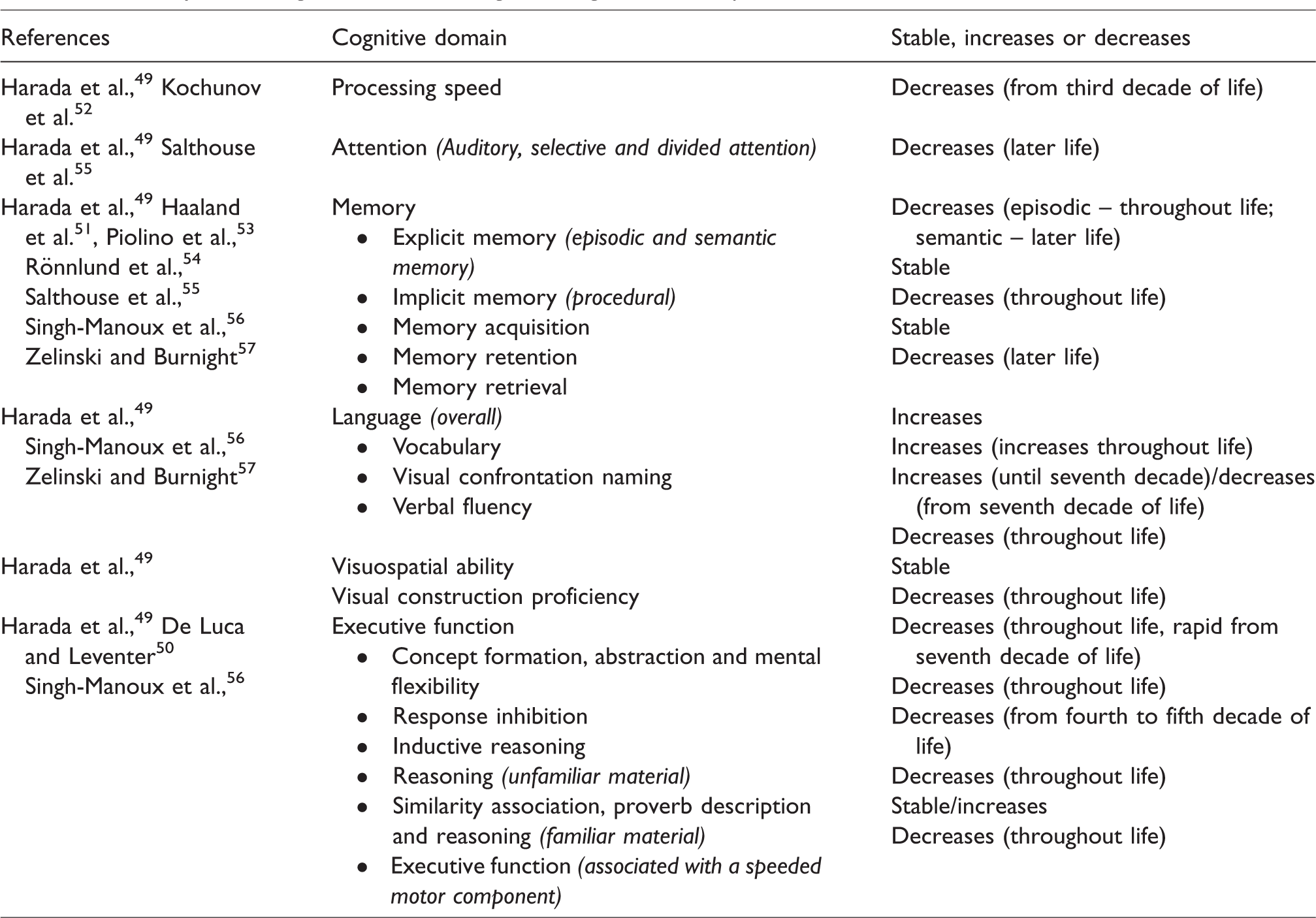
Whilst crystallised intelligence (i.e. acquired knowledge) remains relatively unchanged, our fluid intelligence (ability to respond to novel situations), such as processing speed, attention, memory, language, executive functions and visuospatial ability, and visual construction proficiency decreases with ageing. 49 The changes in these cognitive domains in normal ageing are summarised in Table 1, which indicates that the majority of these abilities decline at some stage throughout the lifespan. The exceptions to this include certain aspects of memory (implicit memory and memory retention), language (vocabulary and visual confrontation naming), visuospatial ability and similarity association and proverb description and reasoning of familiar material (executive function domain).49–57
Summary of the cognitive domain changes throughout the lifespan.
Our understanding of the anatomical and functional changes that occur within the brain during ageing is not well defined. These changes may vary between individuals and populations and are undoubtedly related to modifiable (environmental) and unmodifiable (genetic) changes. They may be affected by a variety of disease states that promote cerebrovascular dysfunction, oxidative stress and inflammation.58–61 Further, actual cognitive changes may lag behind neuroanatomical changes by decades and, therefore, may not correlate. 60 Nonetheless, there appears to be consensus that the brain’s grey matter declines with age in conjunction with expansion of the cerebral ventricles, 62 thus contributing to age-related cortical thinning. Further, the prefrontal, medial temporal and parietal cortices are some of the most vulnerable regions to senescent changes.49,58,60 This is likely a consequence of neuronal death and reduced plasticity due to decreases in synaptic density. 49 Additionally, white matter also decreases with age, but there is limited information about structural changes compared with functional connectivity.49,59 Functional connectivity is reduced within the default mode network, which is comprised of the precuneus and the post cingulate, medial prefrontal and lateral parietal cortices and has been correlated to reduced attention, memory and executive function.58,59 In post-mortem examinations, these anatomical changes are associated with the deterioration of the BBB, thus suggesting that these changes are associated with impaired cerebrovascular function. 62 In support of this, reduced CBF and metabolism are associated with reduced functional connectivity and anatomical changes in healthy individuals and are exacerbated in those with Alzheimer’s disease. 63 Since poor cardiometabolic status intensifies endothelial dysfunction, cerebrovascular dysfunction and cognitive decline, interventions that improve cardiometabolic health, such as regular exercise, may be beneficial in preventing or slowing the progress of the chain of events leading to dementia.5,64
Ageing and cerebrovascular function
As we age, the endothelium’s ability to produce adequate concentrations of nitric oxide (NO) to maintain optimal vascular health and cerebrovascular function decreases. 5 Even in healthy individuals, CBF is estimated to be continually reduced by 0.38–0.45% annually from midlife onwards until age 80 years, after which the trajectory is unknown. 19
The mechanisms that lead to age-related endothelial dysfunction and diminished NO concentrations are complex and are not fully understood. What is clear is that the senescent phenotype favours decreased vasodilator tone, platelet aggregation, vascular smooth muscle cell proliferation and inflammation, which is probably associated with elevated oxidative stress caused by an increase in reactive oxygen species (ROS) production.
65
In animal models, ROS production has been demonstrated to be a key factor leading to endothelial dysfunction, cerebrovascular dysfunction and cognitive impairment.66–68 Further, there is increased uncoupling of endothelial nitric oxide synthase (eNOS) in ageing, resulting from a diminished
Endothelial dysfunction may also be induced by hormonal imbalances and increased angiotensin activity. Both of these are associated with the senescent phenotype and promote vascular inflammation and ROS production. They may also promote increased endothelial expression of endothelin-1, which induces vasoconstriction while suppressing the effects of NO.70,72,73 Additionally, adiposity from mid-to-late life reduces systemic adiponectin concentrations, which may have a role in maintaining cerebrovascular function and reducing vascular inflammation via upregulating eNOS activity.74,75 In any case, NO bioavailability becomes diminished as it reacts with superoxide, resulting in peroxynitrite formation and continuation of the inflammatory cycle leading to endothelial cell dysfunction and the promotion of atherosclerosis and cardiovascular diseases. 5 Ultimately, this impairs or causes a decline in the effectiveness of CBF regulatory mechanisms. The resulting decline in CBF leads to cerebral hypoperfusion, cerebral dysfunction and the development of cognitive impairment, as well as the potential development of leukoaraiosis (i.e. white matter lesions resulting from small blood vessel damage frequently observed as white matter hyperintensities on MRI) and increased amyloid-β production that is characteristic of dementia.3,5
Why exercise training might improve cerebrovascular and cognitive function – evidence from animal studies
Acutely, CBF increases concurrently with cardiac output and oxygen uptake (
Exercise training promotes angiogenesis within areas of the brain that were previously ischaemic, via the upregulation of eNOS and endothelial progenitor cell production in mice and Sprague–Dawley rats.77,78 The reduction in endothelial expressed low-density lipoprotein (LDL) receptor-related protein 1 that occurs during ageing has been linked to decreased cerebral perfusion in animals, and exercise training has been demonstrated to reverse this process, thereby improving cerebrovascular function.75,79,80 These findings suggest that exercise training may improve endothelial function, which would possibly increase cerebrovascular function, which is related to cognition.
In support of this, it was reported that in middle-aged female mice, AT improved cerebrovascular function, peripheral endothelial function as well as favourable neuroanatomical changes, such as decreased hippocampal astrocyte hypertrophy. 81 This was in contrast to the sedentary group who had increased hippocampal astrocyte hypertrophy, reduced vascular and cerebrovascular function and myelin dysregulation. 81 Additionally aged Wistar rats that underwent swimming training for 1 h per weekday for eight weeks demonstrated significantly increased CBF and brain capillary vascularity, in addition to increased brain microvessel vascular endothelial growth factor (VEGF) and eNOS concentrations and reduced plasma malondialdehyde concentration, compared to aged sedentary rats and rats immersed in water for leisure. 82 However, these were still below to be lower than young sedentary rats, thus supporting the notion that CBF decreases with age and that exercise training can improve these outcomes possibly by upregulating VEGF and eNOS and reducing oxidative stress.
In aged animals, there are a lack of studies that directly test the effects of exercise on CBF and cognition. One study using a mouse model of Alzheimer’s disease reported improvements in both CBF and cognition using a pharmaceutical intervention, while another demonstrated that exercise improved neurogenesis and cognition in aged mice.83,84 This suggests that exercise, which can improve both CBF and cognition in animals, may result in improved outcomes associated with the ageing brain. In support of this was another study that reported middle-aged to older female cynomolgus monkeys that underwent AT had improved cognition (determined by the Wisconsin General Testing Apparatus) and vascular volume within the cerebral cortex compared to aged-matched sedentary controls. 85 However, these findings were found to be abolished following a three-month period of physical inactivity, which also suggest exercise is a vital component in maintaining neurovascular function throughout the ageing process.
In summary, these novel animal studies highlight that exercise training improves cerebrovascular function and cognition by improving vascular health, specifically endothelial function. These few novel studies provide insight as to why exercise may improve cerebrovascular and cognitive function in humans, as they improve parameters that are associated with ageing, such as decreased endothelial function leading to reduced cerebrovascular function, BBB integrity and ROS formation.
Results of studies
The effects of exercise training on cerebrovascular function and structure
The studies that have been included in the results have measured and reported cerebrovascular function slightly different from each other or have at least focused on one aspect of cerebrovascular function. Hence, it is important to address terms used throughout the text here. Cerebrovascular responsiveness (CVR) is the ability of the vasculature to respond to cognitive or physiological stimuli.86,87 Specifically, the response of smaller healthy vessels to a stimulus is to dilate, which results in an increase in CBF.86,87 The physiological mechanism that ensures that CBF is maintained and kept constant during changes in systemic blood pressure is referred to as cerebrovascular autoregulation (i.e. cerebrovascular conductance).5,26 This is stimulated by chemical and mechanical stimuli, which induce a myriad of molecular pathways, including those described above, which result in modulating the vascular resistance applied to the cerebral vasculature and, therefore, the CBF. 5 Further, cerebrovascular function can be described as declining if cerebral pulsatility (i.e. cerebral arterial stiffness) increases. 20 This will be observed in conjunction with a decline in CBFV. 20 These functions can be determined by medical imaging systems (e.g. MRI and ASL) and TCD ultrasonography.
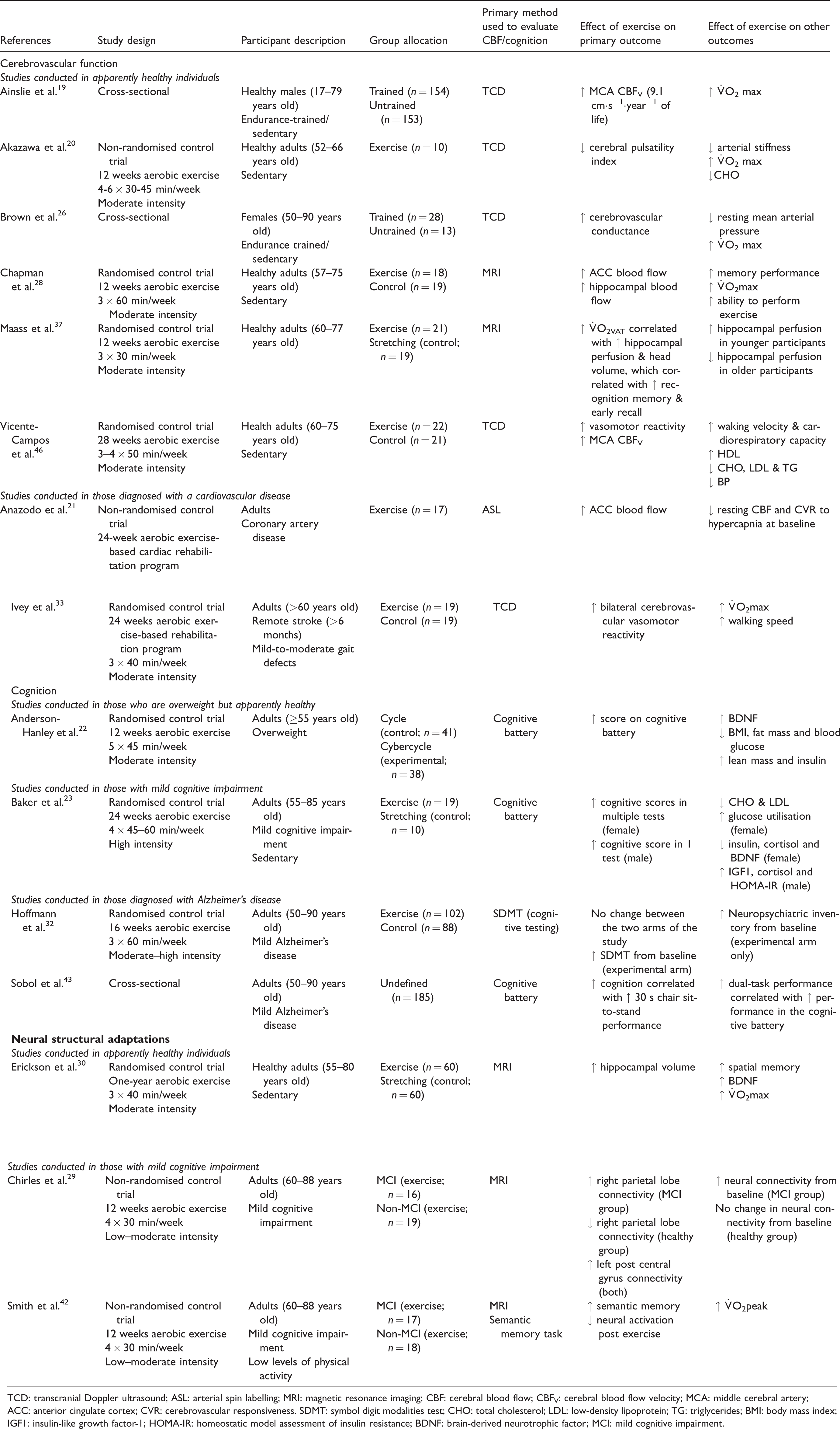
Aerobic exercise training (Table 2)
Ainslie et al.
19
measured CBFV in the middle cerebral artery (MCA) in apparently healthy aerobic exercise trained and sedentary males. Their estimation of the annual decrease in CBFV was 0.45%. However, CBFV remained 17% higher in aerobic exercise-trained individuals compared to their age-matched sedentary counterparts, suggesting a difference in cerebrovascular function of 10 years between the active and sedentary individuals. A major limitation to this study was that CVR was not evaluated. Brown et al.
26
assessed whether higher aerobic fitness was associated with superior cognitive in a group of healthy aerobic exercise trained and sedentary older women. Trained females had a higher
Summary of research that has examined the effects of aerobic exercise training on cerebrovascular function, cognition and neural structural adaptations.
TCD: transcranial Doppler ultrasound; ASL: arterial spin labelling; MRI: magnetic resonance imaging; CBF: cerebral blood flow; CBFV: cerebral blood flow velocity; MCA: middle cerebral artery; ACC: anterior cingulate cortex; CVR: cerebrovascular responsiveness. SDMT: symbol digit modalities test; CHO: total cholesterol; LDL: low-density lipoprotein; TG: triglycerides; BMI: body mass index; IGF1: insulin-like growth factor-1; HOMA-IR: homeostatic model assessment of insulin resistance; BDNF: brain-derived neurotrophic factor; MCI: mild cognitive impairment.
One of the first exercise training studies undertaken evaluated the effects of AT in healthy, sedentary and overweight older adults.
46
CBFv in the MCA in response to breath-holding was higher in the trained group compared to the control group. Additionally, AT decreased blood pressure and improved individual lipid profiles, in addition to increasing exercise performance. This suggested that AT improved cerebral responsiveness by modulating cardiovascular markers, thus contributing to improved cardiovascular health and, consequently, improved endothelial function. This was supported by a recent interventional study that investigated the effects of AT assessing the response of cerebral pulsatility to an acute bout of exercise before and after exercise training in older sedentary adults.
20
The trained group had improvements in CBFV and a decreased PI, as well as lower total cholesterol concentrations and increased peak oxygen uptake (
The benefits of regular AT are also evident in patients with established endothelial dysfunction. Anazodo et al. 21 measured changes in both resting CBF and CVR to hypercapnia in patients with coronary artery disease and healthy patients of the same age, following an AT-based program. At baseline, patients were reported to have lower CBF, reduced CVR to hypercapnia, and some atrophied brain regions compared to their healthy counterparts. Following the exercise intervention, CBF was increased in the anterior cingulate cortex (ACC) in the coronary artery disease patients. In fact, the increase in CBF to this region was equal to the shortfall measured at baseline, i.e. the difference between the exercise intervention group and the control group at baseline.
A similar improvement in cerebral perfusion was also observed in overweight adults, who suffered from a stroke and were at risk of developing mild cognitive impairment (MCI).
33
AT improved bilateral CVR to hypercapnia which were accompanied by a 19% improvement in
A larger study which assigned older sedentary adults to a one-year walking program
30
showed increased hippocampal volume, systemic brain-derived neurotrophic factor (BDNF) concentrations, spatial memory and
The changes elicited in regions of the brain that are responsible for cognition following AT have not been clear. A study that evaluated the effects of AT on hippocampal vascularity in healthy older adults, indicated varied results.
37
Chapman et al. 28 assigned cognitively healthy, sedentary adults to an AT program. Following training, CBF was increased at rest in the ACC, which is responsible for executive functioning and autonomic cardiovascular control. The trained group also demonstrated improved immediate and delayed memory performance, which was associated with a general increase in hippocampal perfusion. The authors suggested that exercise training could assist in diminishing the biological and cognitive consequences of the senescent phenotype in sedentary older adults by increasing neuroplasticity in both the ACC and hippocampus. However, measurements of physical volume of these brain areas were not undertaken. Hence, this study indicates that improvements in cerebrovascular function, particularly within the ACC and hippocampus, following AT are associated with improved cognitive capacity in sedentary older adults and that these changes may diminish the progression of the senescent phenotype described above.
In summary, there is strong evidence that AT improves cerebrovascular function. The studies presented indicate that improved vascular function and health and exercise capacity may be associated with these improvements as well as increased systemic BDNF concentrations.
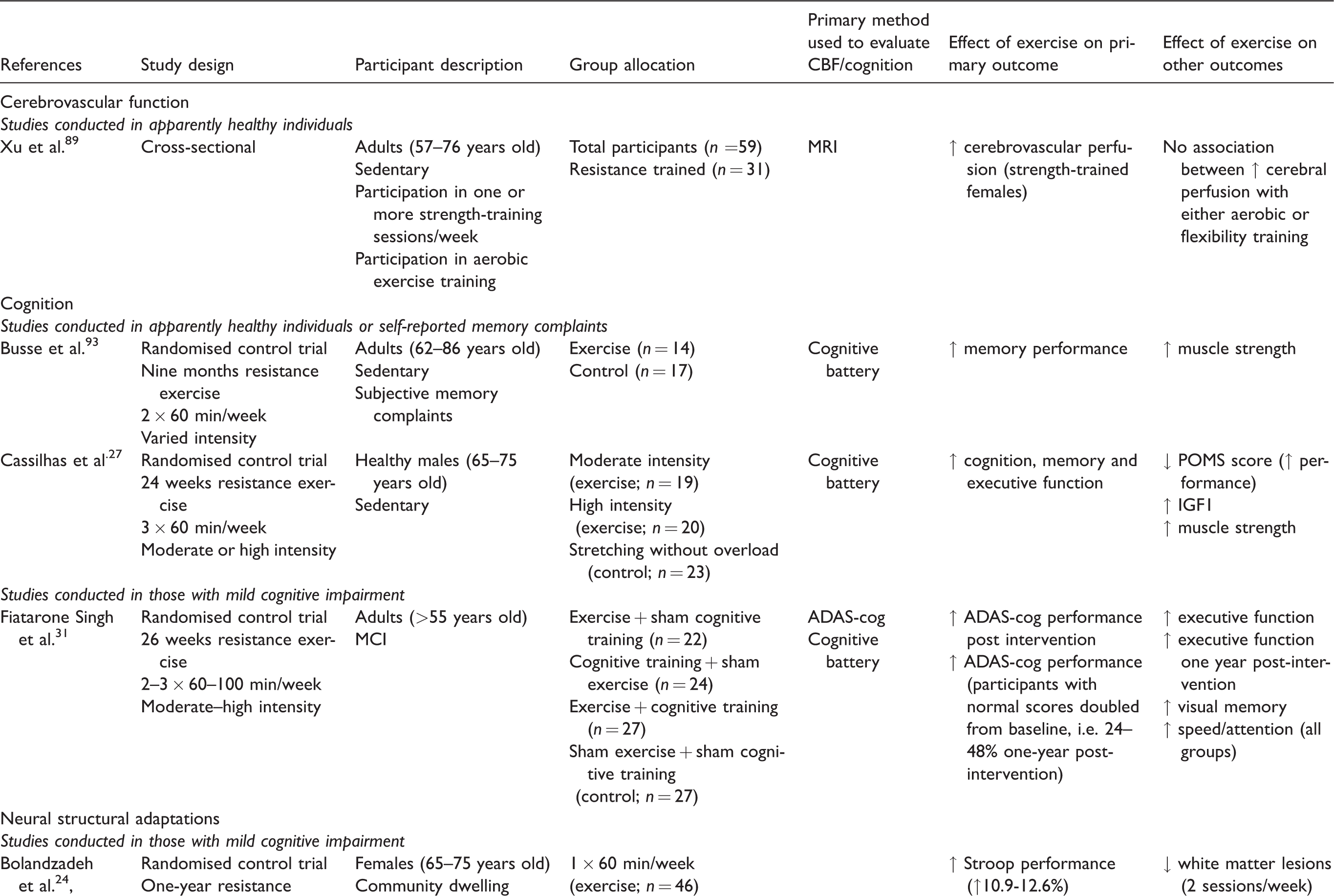
Summary of research that has examined the effects of resistance exercise training on cerebrovascular function, cognition and neural structural adaptations.
MRI: magnetic resonance imaging; ADAS-Cog: Alzheimer disease assessment scale–cognitive subscale; POMS: profile of mood states; RAVLT: Rey’s auditory verbal learning test; IGF1: insulin-like growth factor-1; MCI: mild cognitive impairment.
Resistance exercise training (Table 3)
Xu et al. 89 investigated the impact of flexibility, RT and AT on cerebrovascular perfusion in older adults. It was reported that females who participated in RT had greater cerebrovascular perfusion than those who did not and that this finding remained significant after adjusting for health, educational status and the other types of exercise training performed. It was also reported that there was no association between cerebral perfusion and AT or flexibility training. While interesting, these results were based on self-reported subjective data obtained from a small sample size and did not include the intensity and duration of exercise and should be examined with caution. Additionally, the authors of this study did not offer an explanation or propose a mechanism whereby RT could improve cerebrovascular perfusion. The adaptations to RT and cardiovascular function are not well understood compared to AT. To highlight this, a recent cross-sectional study of nearly 400,000 United States residents aimed to determine whether meeting the current physical activity guidelines for moderate-to-vigorous intensity aerobic physical activity, RT or both were associated with chronic health conditions. 90 It was reported that meeting the guidelines for both forms of physical activity resulted in less risk of developing any cardiovascular disease, including stroke, and that meeting the strength component of the guidelines alone resulted in less risk of cardiovascular disease development than moderate-to-vigorous intensity aerobic physical activity. Hence, it may be plausible that strength training can reduce the incidence of systemic vascular disease and may also reduce cerebrovascular dysfunction, through an unknown and unexplored mechanism.
Other than the longitudinal data presented above, there have been no studies that examine the effect of RT on cerebrovascular function.
The effects of exercise training on cognitive function
Aerobic exercise training (Table 2)
A population-based study examined the relationship between aerobic exercise-trained individuals and executive function at the start of adulthood and the risk of developing cognitive impairment in later life. 41 Over one million young Swedish males who were subject to mandatory conscription examinations between 1968 and 2005 were evaluated to ascertain the risk of developing cognitive impairment. Aerobic fitness and cognitive performance at 18 years of age was associated with an increased risk of developing cognitive impairment in later life. Specifically, those with poor aerobic fitness had a >7-fold increased risk of developing early-onset dementia and early-onset MCI, while those with poor cognitive performance had a >8-fold increased risk compared with those who did not. Another cross-sectional study, which utilised the baseline data from their AT study involving older participants with mild Alzheimer’s disease, reported that a greater performance in the 30 s chair sit-to-stand test correlated with increased cognition. 43 Sobol et al. 43 concluded that there was a strong association between superior cognitive performance, physical function and the ability to carry-out dual tasks, thus suggesting that interventions that improve physical function and the ability to multi-task may impart benefits on improving cognitive outcomes and prevent further deterioration in patients with mild Alzheimer’s disease. Taken together, these studies suggest that physical fitness is strongly associated with cognitive performance and that the former has a positive effect on the latter.19,26,41,43
Smith et al.
42
determined if AT could improve semantic memory activation during fMRI in physically inactive older adults with MCI in comparison to appropriately matched cognitively-intact individuals.
Baker et al. 23 evaluated the impact of AT on cognitive function and biomarkers of Alzheimer’s disease in older adults with amnestic MCI. After training, female participants had improved cognition, cortisol and BDNF concentrations compared to the stretching (control) group. Aerobically trained men, however, had increased insulin-like growth factor-1 (IGF1) and only performed favourably in one of the cognitive battery tests. Hence, this study concluded that AT can improve cognition and that these effects may be greater in women who are at greater risk of developing cognitive impairment than men, possibly due to an altered hypothalamic–pituitary–adrenal axis response. While this may in part be true, these findings and the increased risk of developing MCI in women may also be due to loss of the vasoprotective effects of oestrogen post-menopause. 91 Taken together, these studies20,23,46 suggest that AT improves cognitive function and indicate that improved lipid profiles are important for maintaining vascular health and, therefore, cerebrovascular function. Further, it suggests that there may be a sex difference in responses to exercise training, which should be considered in future studies.
In another intervention study, overweight older adults participated in three-month traditional cycling or cyber-cycling (a cycle ergometer with an attached virtual reality component) training demonstrated increased cognitive performance and systemic BDNF concentrations compared to their baseline results. 22 Cyber-cycling participants had greater increases than those who underwent traditional cycling, resulting in a medium effect size improvement of cognitive performance compared to the control group. This suggested that virtual reality coupled with AT increased neuroplasticity more than standard AT and that cyber-cycling imparts a 23% relative reduction in the risk of MCI development. This study did not have a sedentary control group but relied on improvements from baseline measurements and did not provide details of potential mechanism/s by which a virtual reality component could elicit improved executive functioning, other than suggesting that increased BDNF concentrations may have elicited these results. Hence, this may provide a future direction for researchers to consider when prescribing exercise coupled with a virtual reality program.
A later and larger study evaluated the effects of AT in sedentary older adults with mild Alzheimer’s disease. 32 There were no differences between the control and training groups in cognitive performance. However, participants with over 80% compliance to the exercise program and trained at 70% of their maximal heart rate or greater exhibited improvements in cognitive performance from baseline compared to the control group, thus suggesting a dose–response relationship between AT and cognitive performance. Finally, it was reported that neuropsychiatric scores were improved from baseline in the exercise group compared to the control group, whose scores declined over the course of the program. Hence, it was concluded that AT could impede or slow the progression of neuropsychiatric symptoms and that increased adherence to AT is imperative to improve cognition in those who are already cognitively impaired.
In summary, there is evidence that AT can improve cognitive performance. Again, this appears to be related to improved exercise capacity. However, the mechanism leading to these changes is not clear, but may involve increased systemic BDNF, vascular health and hormonal changes. Further studies are required to determine the mechanism of action leading to improved cognitive performance.
Resistance exercise training (Table 3)
Cassilhas et al. 27 conducted one of the first studies investigating the effects of RT on cognition in healthy, sedentary, older males. A limitation to the exercise protocol used in this study was that no progressive overload, periodisation or adjustments added or made that adjusted for intensity and conditioning to this program. The program may have been completed in this manner for simplicity, since the control group performed the same routine once per week without any overload applied. In any case, both exercise groups demonstrated improved cognition in comparison to the control group. Lean mass, systemic IGF1 concentrations and muscle strength were increased in both of the exercise groups when compared to the control group, with these changes being more prominent in the high-intensity exercise group. Additionally, IGF1 concentrations decreased in the control group suggesting IGF1 may be mediating the change in cognition. These results suggest that RT could improve cognitive function possibly by increased growth factors, which may act as mediators of neurogenic pathways within the brain.27,92 However, no correlational results were generated from this study.
This finding was supported by a later study that investigated the effects of RT on cognitive performance and muscle strength in sedentary older adults with subjective memory complaints. 93 It was found that the exercise group, particularly the women, demonstrated improved memory performance within the cognitive battery administered and increased muscle strength compared to the control group. This finding indicates that RT may improve memory deficits in elderly participants with memory complaints.
Finally, Fiatarone Singh et al. 31 evaluated 26 weeks of either progressive RT, cognitive training or a combination of both on global cognitive function in older adults with MCI. The cognitive training incorporated the COGPACK program, which is a neuro-rehabilitation program incorporating adaptive computerised exercises of memory, executive function, attention and processing speed. 98 Upon study completion, those in the RT group demonstrated improvements to a greater extent than the other groups in the Alzheimer Disease Assessment Scale–Cognitive Subscale (ADAS-Cog), which assesses cognitive decline. In this group, the proportion of participants attaining normal ADAS-Cog scores increased from only 24% at baseline to 48% following one year of training. They also performed 74% higher in executive function testing than the other groups in a 12-month follow-up post-intervention, indicating that the improvements in executive function were sustained for at least one year. Additionally, the RT group demonstrated increased visual memory performance compared to the other groups immediately post-intervention. These findings indicate that progressive RT improves global cognitive and executive functions and that cognitive training prevents any further decreases in overall memory and cognition. Interestingly, combined training did not demonstrate an enhanced benefit compared to RT alone, possibly because it was too challenging for participants to successfully engage for a full 100 min, separating RT and cognitive training may have assisted this. Why cognition was maintained a year after RT cessation was unclear, and biomarkers such as IGF1 and BDNF were not measured.
The cognitive improvements observed by Busse et al. 93 were more evident in females than males and Xu et al. 89 reported that sex differences could account for differences in improvements of cerebral perfusion and cognition induced by RT. Two larger trials examined this finding by investigating the efficacy of chronic exercise training, particularly RT, on executive functions and cognition in elderly females with MCI.24,35,36,39,45 The EXCEL study randomised participants to either AT or RT or to a balance and tone (control) group.39,45 Compared to the control and AT groups, participants in the RT group increased performances in the Stroop test, memory tasks and conflict resolution, as well as enhancing functional plasticity in the right lingual and occipital–fusiform gyri and right frontal pole, assessed by fMRI. The AT group reported a 4% increase in hippocampal volume compared with the other groups but did not show improvement in memory performance to the recall tasks, as one would expect an increase in hippocampal volume to correlate with improved memory function. These findings suggest that RT improves cognitive performance and regional brain plasticity to a greater extent than AT in elderly females at risk of further cognitive decline.
The other large-scale study aimed to determine if performing once or twice weekly RT sessions for one year could improve executive function and cognition in older females compared to balance and muscular toning exercises.24,35,36 Both RT groups improved by 10.9–12.6% in the Stroop test compared with a control group who reported a 0.5% decrease and demonstrated improved executive function compared to the control group. However, only the participants performing two RT sessions per week had increased functional plasticity in the left middle temporal gyrus and left anterior insula, as well as superior performance in the flanker task and muscle power measurements. Additionally, MRI revealed a decrease in whole-brain volume in both groups compared with the control group. The authors of the study cautiously suggest that this may have been due to an increase in amyloid-β removal in conjunction with other neural proteins, as this had been a finding in previous studies that specifically measured and noted reductions in cerebral volume following treatments with pharmaceuticals.94,95 This study did not measure any neurodegenerative or inflammatory biomarkers and could only speculate that this may be the case. In support of this, however, the twice per week RT group experienced a decrease in white matter lesions, which one-third of the participants were reported to possess. These findings warrant further research into the effect of exercise on cerebral volume. In any case, it was concluded that two RT sessions performed twice a week may improve cognition, executive function, selective attention and conflict resolution in older females and that this dosage of exercise could potentially convey favourable functional plasticity changes in a manner similar to AT.
Taken together, these studies indicate that RT improves cognitive performance. However, none of these studies offer an insight as to why RT appears to exert a greater effect in women than men. Future studies might benefit from measuring different hormones, such as androgens and oestrogens. It has been suggested that phytoestrogens, such as resveratrol, increase central oestrogen receptor activity, while promoting upregulation of eNOS and, therefore, NO production, thus leading to improvements in cerebrovascular function. 91 Further, these studies did not investigate possible effects of changes in body composition, as it is well known that a result of RT is increased lean mass. Any increase in tissue, whether positive or negative, demands increased capillarisation and recruitment of the existing vasculature, which is largely mediated through VEGF, a protein that promotes angiogenesis and potentiates the effects of NO. Specifically, central VEGF concentrations and increased cerebral capillarisation have been demonstrated in animal studies to be upregulated centrally via the centrally derived lactate receptor hydroxycarboxylic acid receptor 1 (HCAR1) following increased plasma lactate concentrations and shear stress.96,97
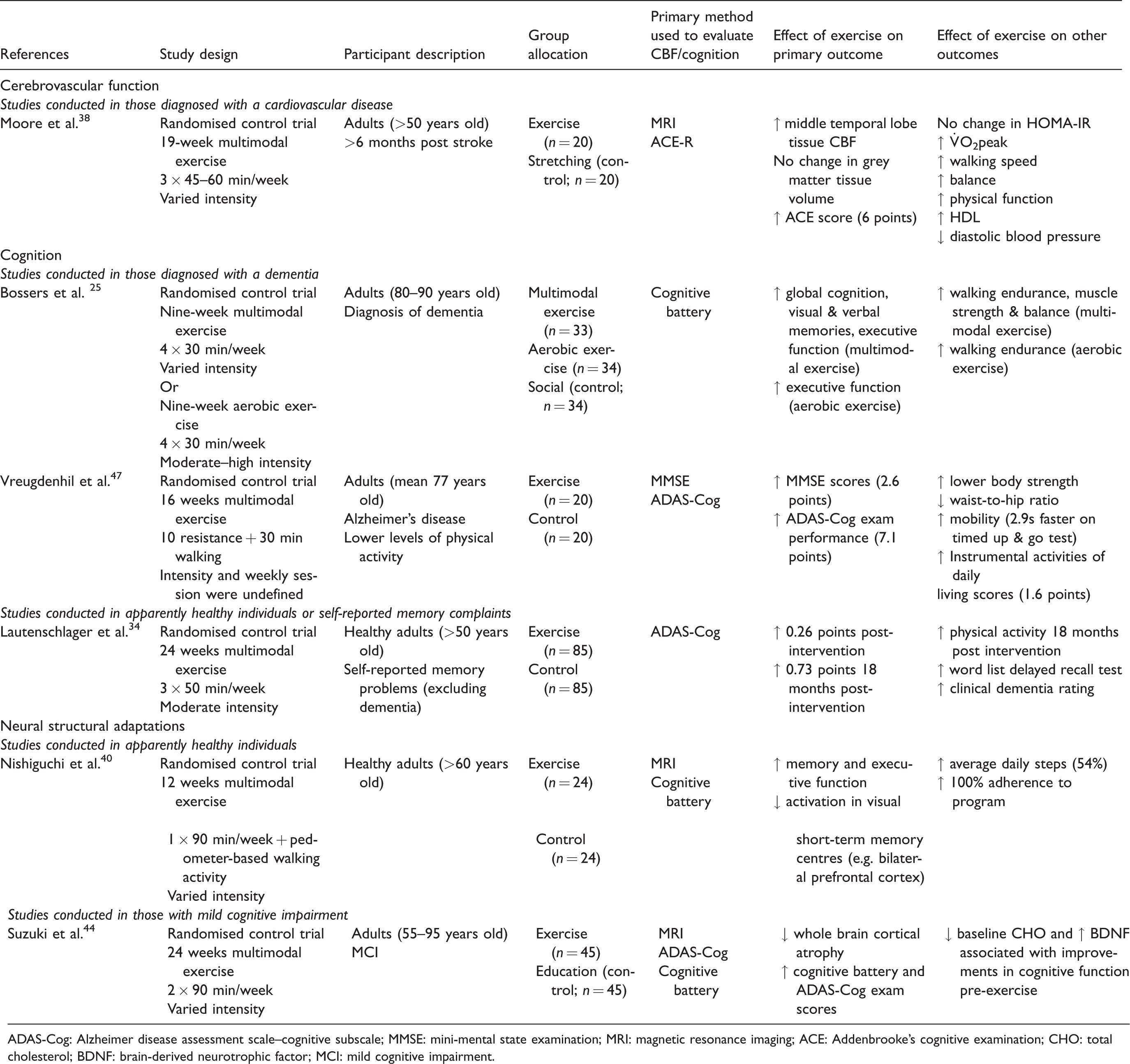
The effects of multimodal exercise training on cerebrovascular function, structure and/or cognition (Table 4)
One of the first intervention studies examined the effects of CT (of the participants’ choice) on cognition in older participants with self-reported memory problems. 34 The rate of cognitive decline (evaluated using ADAS-Cog exam) improved by 0.26 points post-intervention, while the control group had declined by 1.04 points, both of which were considered as clinically significant. Eighteen months post-intervention, the intervention group had improved by a further 0.73 points, whilst the control group improved 0.04 points from the previous ADAS-Cog examination. The intervention group also reported a modest improvement in a word list delayed recall test and clinical dementia rating. These findings were supported by a later study that investigated the effects of CT on cognition in physically inactive older Alzheimer’s disease patients. 47 It was reported that exercise training improved mini-mental state examination (MMSE) scores by 2.6 points and ADAS-Cog by 7.1 points. Taken together, these studies suggest that CT improves both cognitive and physical function in elderly individuals with either self-reported memory issues or Alzheimer’s disease. However, the latter study did not define intensity, dose or progression, thus it is unknown if there was a dose–response relationship in relation to the study outcomes.
Summary of research that has examined the effects of multimodal exercise training on cognition and neural structural adaptations.
ADAS-Cog: Alzheimer disease assessment scale–cognitive subscale; MMSE: mini-mental state examination; MRI: magnetic resonance imaging; ACE: Addenbrooke’s cognitive examination; CHO: total cholesterol; BDNF: brain-derived neurotrophic factor; MCI: mild cognitive impairment.
Bossers et al. 25 compared the effects of either CT or AT on cognitive and motor function in institutionalised elderly adults with dementia. Post-intervention, the CT group demonstrated increased global cognition, visual and verbal memories and executive function compared with the control group, while the AT group only demonstrated increases in executive function compared to the control group. Eighteen weeks post-intervention, there was a decline in cognitive function towards baseline values. Hence, it was concluded that a combined exercise program is more effective than AT alone in reducing cognitive and motor function decline in patients with dementia.
Suzuki et al. 44 assigned older adults with MCI to a CT program. Memory function and whole brain cortical atrophy all improved after training compared to controls. Further, lower total cholesterol and higher BDNF concentrations were associated with increased cognitive function and memory in patients with MCI at baseline than those who had higher total cholesterol and lower BDNF concentrations. However, it was not determined how having higher or lower baseline concentrations of these biomarkers impacted the results throughout the course of the study, or if participants with more favourable concentrations of these biomarkers responded better to the exercise intervention compared with those who had a less favourable profile. Interestingly, these biomarkers were not measured upon completion of the study, as this could have provided a mechanism or possibly explained the improved response to exercise. This study provides further evidence that exercise training improves cognitive function and was supported by Nishiguchi et al. 40 who evaluated the effects of CT on cognition and brain activation efficiency healthy older adults. The exercise group had improvements in memory and executive function when compared to the control group, but they had less activation in regions of the brain, such as the prefrontal cortex, that were associated with short-term and visual memory. Hence, it was concluded that the combined exercise increased the activation efficiency of the brain during cognitive tasks and that this was associated with improved memory and executive function.
Moore et al.
38
examined a CT program in older participants who had previously suffered from a stroke six months prior or longer. Medial temporal lobe tissue CBF increased in the exercise group without incidence of grey matter atrophy compared to the control group, who reported a decrease in grey matter atrophy. Further, exercise training improved cognition by 6 points. Training increased
In summary, there is evidence that CT improves both cerebrovascular function and cognitive performance, particularly in those that have been diagnosed with stroke, MCI or dementia. The mechanism of action is, again, not clear, but likely involves improved vascular function and health leading to increased CBF, increased exercise capacity and structural adaptations within the brain that lead to improved brain activation efficiency.
Why does cerebrovascular and cognitive function change following exercise training?
It is evident from this review that exercise training improves cerebrovascular structure and function and cognition. It is also evident that the mechanisms that lead to these improvements in humans are poorly defined. The link, or the associations, between the two do not appear clear. Very few studies have performed correlation analyses on the results generated from their studies or undertaken perturbation studies to understand the mechanisms involved. Erickson et al.
30
analysed associations between hippocampal volume and
Mechanistic evidence observed in animal studies
What occurs centrally after exercise training is poorly defined in humans. Centrally in mice there is an increase in oxidative enzyme synthesis, suggesting that exercise may improve central oxidative capacity.82,98–104 Therefore, it may be plausible that some of the adaptations that are described in skeletal muscle may also occur centrally, thus leading to improvements in cerebrovascular and cognitive functions. Specifically, chronic exercise in animal enhances endothelial function, upregulates eNOS expression and activity thereby increasing NO production and reduces ROS production. These changes reduce vascular inflammation and inhibit endothelial dysfunction. Additionally, exercise training enhances mitochondrial biogenesis via upregulating transcription factors, such as peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α). 105 Specifically, PGC-1α upregulates oestrogen-related receptor alpha-α, which subsequently upregulates lactate dehydrogenase (LDH) B and indirectly inhibits LDH A, thus leading to increased lactate oxidation during exercise. 106 This process increases the oxidative capacity of skeletal muscle and improves an individual’s exercise capacity, as well as contributing to reducing ROS production, chronic inflammation, angiogenesis and the loss of muscle atrophy and function that is associated with the senescent phenotype.105,106 However, further studies are required in order to demonstrate this.
The clinical studies described indicate that specific growth factors may have a role in conferring improvements in cerebrovascular and cognitive functions in at risk populations. Acute exercise results in increased arterial shear stress, enhanced synthesis of growth hormone and NO, as well as increased β-hydroxybutyrate and lactate production, all of which either stimulate increased IGF1 synthesis, promote increased BDNF expression and synthesis and/or HCAR1-induced VEGF upregulation, respectively.96,97,107–111 BDNF and IGF1 are expressed centrally and systemically and when produced systemically cross the BBB and augment the response of their centrally derived counterparts.97,112 These factors promote increased neuroplasticity, neurogenesis, neural repair, synaptogenesis and angiogenesis, in addition to possibly promoting the removal of amyloid-β.96,97,105,107,108,110–115 BDNF and IGF1 may also enhance glutamate synthesis centrally, via upregulating synapsin-1, thus contributing to improved cognition. 114 Additionally, VEGF promotes angiogenesis and potentiates the effects of NO via phosphatidylinositol-4,5-bisphosphate hydrolysis, which subsequently activates the calmodulin and protein kinase B and C pathways, thus resulting in eNOS upregulation.82,96,110
In older animal models, ageing increases ROS production and chronic low-grade inflammation, resulting in arterial stiffening.82,101 Exercise training decreases inflammation and ROS production, modulates arterial structure and increases NO bioavailability, thus reducing arterial stiffness and improving endothelial function (reviewed in detail in Ref.116). This has also been suggested to occur in older physically inactive adults. 101 Hence, it would be expected that exercise-induced improvements in endothelial function, which leads to increased CBF, would also improve the ability of these neurotrophic factors to reach the smaller cerebral vessels and potentiate growth, maintenance and efficiency of the areas of the brain that are responsible for cognitive and executive functioning, such as the hippocampus. While this hypothesis seems plausible and may assist in providing an explanation as to why exercise studies note changes in brain volume, plasticity and neural efficiency, future studies are required in order to validate this.
Summary
There is evidence that AT can improve CBF, cognition and neuroplasticity through areas of the brain associated with executive function and memory in older adults but there is still much to explore regarding the effect of RT and how both of these work in concert. This is largely due to the limited studies performed on the effects of RT on cerebrovascular function and cognition. Improvements in cognitive performance and structural adaptations have been reported with RT which, in some studies, was indicated to be superior to AT. There is some evidence that CT may be superior to AT or RT alone. While this seems logical given the systemic health benefits that CT imparts compared with a single exercise modality, more studies are needed to determine whether benefits also occur centrally. It is also evident that improved cerebrovascular function may act to prevent or slow the progress of cognitive impairment and ultimately dementia. There is currently limited literature that has researched the effects of exercise training on cognition in conjunction with cerebrovascular function, general health and well-being. There are also limited human studies that have aimed to determine the mechanisms by which exercise improves these parameters. While it appears that neurotrophic factors increase in an older population in parallel with exercise, no studies have directly attempted to measure cerebrovascular, inflammatory and metabolic markers that may act to increase their production and reduce ROS production by the potential pathways that we have summarised in Figure 2, which have been based on the current evidence and studies conducted in animal models. In any case, we can conclude that exercise training can improve CBF, cognition and neuroplasticity through areas of the brain associated with executive function and memory in older adults and this message should be promoted to the general public.

A summary of the potential mechanisms that may be elicited by exercise in improving cerebrovascular function and cognition. CBF: cerebral blood flow; eNOS: endothelial nitric oxide synthase, NO: nitric oxide; BHB: beta-hydroxybutyrate; GH: growth hormone; VEGF: vascular endothelial growth factor; BDNF: brain-derived neurotrophic factor; IGF1: insulin-like growth factor-1; PGC-1a: peroxisome proliferator-activated receptor gamma coactivator 1-alpha.
Future directions
At present, there are several significant gaps in our understanding of the benefits of exercise training on cerebrovascular and cognitive functions in ageing.
Few of the studies cited indicate a dose–response relationship between exercise training, in particular AT, on cerebrovascular and cognitive function in ageing. This is an important step because we do not know whether more is better or if something is better than nothing given that older adults are not meeting the current physical activity guidelines. Further, we do not know whether meeting these guidelines, especially by those who are physically inactive or sedentary, will benefit cerebrovascular and cognitive function in ageing. Randomised clinical trials that vary the frequency and/or duration of exercise would be beneficial in determining if some exercise is better than none. This raises the question as to whether it may be easier for the general public to participate in exercise of shorter duration, higher intensity and more frequently, especially if there are physiological benefits associated with this. High-intensity interval training has significantly grown in popularity and has numerous benefits that are either comparable to or exceed those elicited by more traditional exercise programs, such as steady-state moderate-intensity AT. These may be due to reduced perceived exertion and excess post-exercise Finally, it is currently unknown if lifelong exercise training of any kind is required to maintain cerebrovascular function and prevent the development of dementia or if participating in exercise later in life can mirror the benefits of lifelong exercise and potentially decrease the likelihood of dementia development. As indicated above, there is limited research that has longitudinally assessed data providing any an insight into the trajectory of cerebrovascular function and cognition with exercise training throughout the lifespan, as well as how the type, duration, frequency and intensity of exercise training may impact these parameters. Future studies that incorporate these aspects will undoubtedly provide novel information and assist in determining the mode, intensity and duration of exercise required to elicit benefits with regard to cerebrovascular function and cognition.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Acknowledgements
The authors would like to acknowledge the University of Southern Queensland for assistance in funding the production of this manuscript.
Declaration of conflicting interests
The author(s) declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.