
Abstract
Prospective studies on magnetic resonance imaging (MRI)-guided systemic thrombolysis 44.5 hours after stroke onset did not reach their primary end points. It was discussed and observed in
INTRODUCTION
Current clinical stroke research aims at selecting ischemic stroke patients who may benefit from systemic thrombolysis beyond the standard therapeutic window of 4.5 hours. 1 For that purpose, the concept of salvageable brain tissue with critical cerebral blood flow (CBF) reduction has been transferred from positron emission tomography (PET) 2 to magnetic resonance imaging (MRI) 3 to allow therapeutic decisions within routine stroke management. Nowadays, brain tissue with perfusion values below established thresholds, but preserved diffusion in MRI is considered as tissue at risk (MR ‘mismatch’ concept). 3 However, selecting stroke patients on the basis of this MR ‘mismatch’ concept did not improve clinical outcome after systemic thrombolysis3–5 and even for endovascular treatment, conclusive evidence for this MR-based selection strategy remains to be provided. 6 The optimal way to derive quantitative CBF values or time-based variables out of perfusion-weighted (PW) MRI that best describe the ischemic penumbra is still a matter of debate. Technical challenges and a lack of standardization 3 in acquiring PW MR data have contributed to this situation. As a consequence, a more precise target profile to delineate perfusion deficits on MRI was recently proposed for future stroke trials. 7
PET with its ability to detect radiotracers at high sensitivity provides highly accurate quantification of pathophysiologic parameters. Cross-calibration of PW MRI against [ 15 O]H2O PET, an established technique to noninvasively quantify CBF, 8 may help to address the above-mentioned problem. Comparison of PW MRI versus [ 15 O]H2O PET data in acute stroke has so far only been possible on the basis of sequential data acquisition. As acute stroke is a highly dynamic pathophysiologic situation, the significant time delay between both modalities possibly affected accuracy in previous research.
We report results from a series of investigations using for the first time simultaneous [ 15 O]H2O PET/MR brain imaging in acute stroke. We aimed at providing proof of concept for simultaneous PET/MRI both in patients with acute stroke as well as in a recently established ovine stroke model. 9 We were able to directly relate CBF estimates from PW MRI to absolute measurements from PET and could exemplify how the same PW MRI threshold can either correctly classify benign oligemia in some patients or fail to do so in other cases.
MATERIALS AND METHODS
A detailed description of the Materials and Methods is available in the Online Supplementary Methods. Ten patients with symptoms of stroke and contraindication against systemic thrombolysis prospectively underwent simultaneous [
15
O]H2O PET/MRI. The local ethics committee of the University of Leipzig approved the study and waived requirement for informed consent. The study was performed in accordance with the Declaration of Helsinki. Apart from [
15
O]H2O PET/MRI, instead of MR-only examination, basic stroke care remained unchanged. The degree of perfusion disturbance was evaluated immediately on-site by an experienced neuroradiologist using standard non-quantitative perfusion-weighted imaging (PWI) maps (syngo.MR NeuroPerfusion, Siemens Health Care, Erlangen, Germany, not shown). Quantitative maps of cerebral perfusion were calculated
Likewise, three male merino sheep were examined either 4.5 hours, 27 hours, or 14 days after permanent middle cerebral artery occlusion (pMCAO). 9 No follow-up imaging was available in the animal studies. The animal experiments were conducted in accordance with the recommendations of the European Convention for the Protection of Vertebrate Animals used for Experimentation and the current ARRIVE guidelines. The animal experiments were approved by the local animal welfare authorities (Directorate Leipzig, Germany).
RESULTS
Ten patients were prospectively imaged in this proof of concept trial. Supplementary Table 1 provides patient characteristics and imaging findings. Standard stroke MRI data acquisition started 43 ± 11 minutes after the patients' informed consent. [ 15 O]H2O for simultaneous CBF PET and PW MRI data acquisition was available 29 ± 18 minutes later. Total PET/MRI scanning time was 61 ± 16 minutes.
According to visual inspection, there was good correspondence between perfusion[PET] and perfusion[MRI] in four patients. In two patients, perfusion[MRI] deficits were detected, which were not evidenced by perfusion[PET], but could correctly be classified as non-critical hypoperfusion with a Tmax >6 seconds. In two patients, unilateral discrete hypoperfusion according to perfusion[PET] was not mirrored in perfusion[MRI]. In one patient, critical hypoperfusion was observed in both perfusion[PET] and (less severe) perfusion[MRI]. In this case, no infarct growth was seen over time because of spontaneous recanalization of the obstructed MCA. Severe head motion prohibited perfusion[MRI] analysis in one patient, whereas perfusion[PET] did not reveal a perfusion deficit in this case. A typical patient with an MCA infarction is presented in Figure 1. In this case, the final infarction on FLAIR follow-up was almost equally well predicted by perfusion[PET] and perfusion[MRI] (choosing a Tmax >6 seconds as threshold). A case of transient diffusion restriction in which reversibility was correctly predicted by both perfusion[MRI] and perfusion[PET] is illustrated in Supplementary Figure 1.
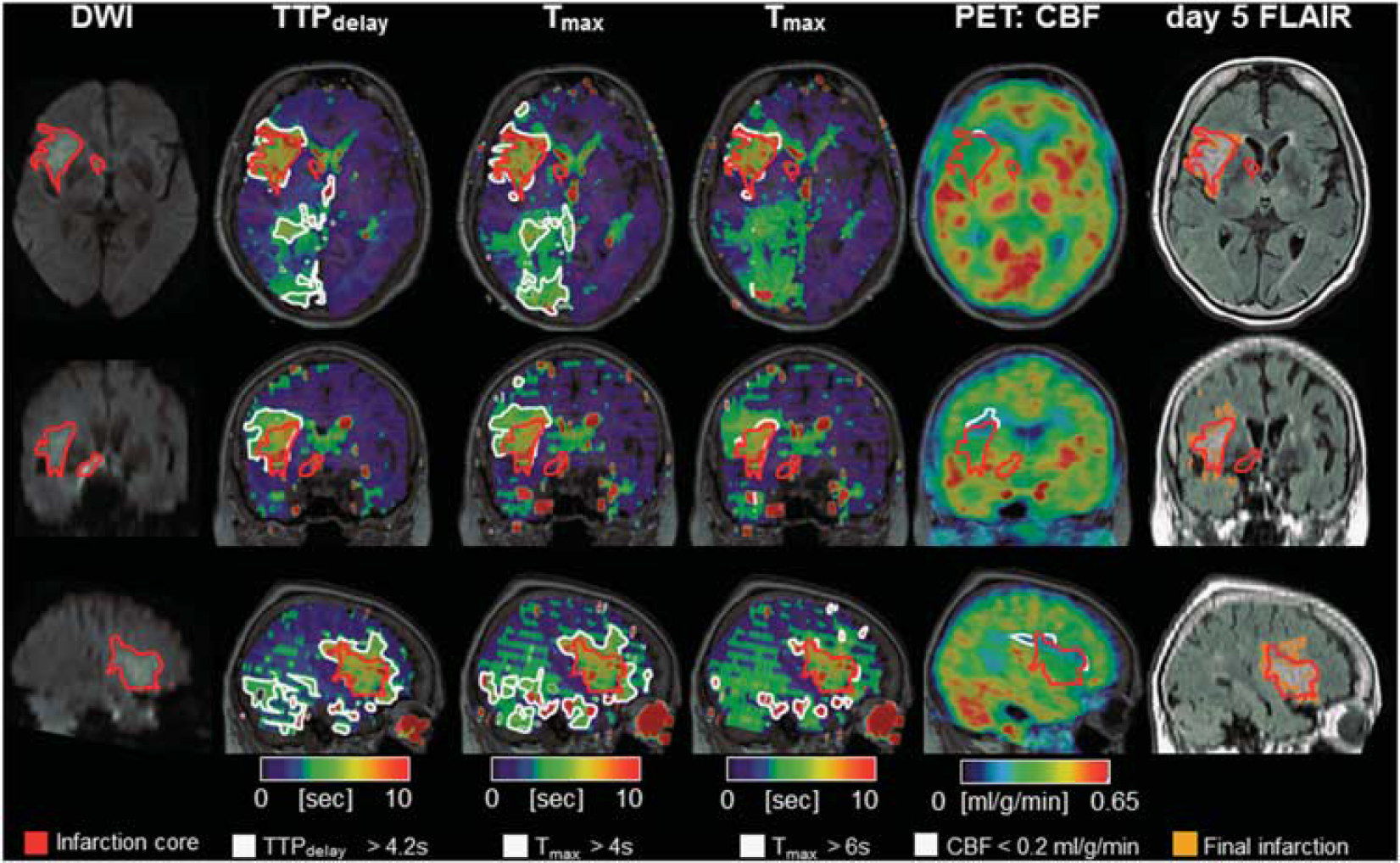
[ 15 O]H2O PET/MRI in a typical human MCA infarction. A 78-year-old, right-handed woman with left hemiparesis and dysarthria upon waking up. Diffusion-weighted MRI showed a disturbance in the right MCA territory (red-bordered area, 22 mL). Perfusion[MRI] flow delays in the right PCA territory did not result in a perfusion restriction according to PET and may thus indicate sufficient collateral flow secondary to the MCA occlusion. Perfusion[MRI] indicated a penumbral volume (white-bordered areas) of 42 mL for Tmax 46 seconds. According to perfusion[PET] (17 mL, white-bordered area) a smaller penumbral volume was predicted that corresponded better with the follow-up infarct size according to T2 FLAIR (infarct growth of 7.5 mL) on day 5. Note: a slight change to time-based variables (TTPdelay >4.2 seconds, Tmax >4 seconds; see Supplementary Methods) leads to misclassification and overestimation of the penumbra (79 mL and 121 mL, respectively). MCA, middle cerebral artery; MRI, magnetic resonance imaging; PCA, posterior cerebral artery; PET, positron emission tomography.
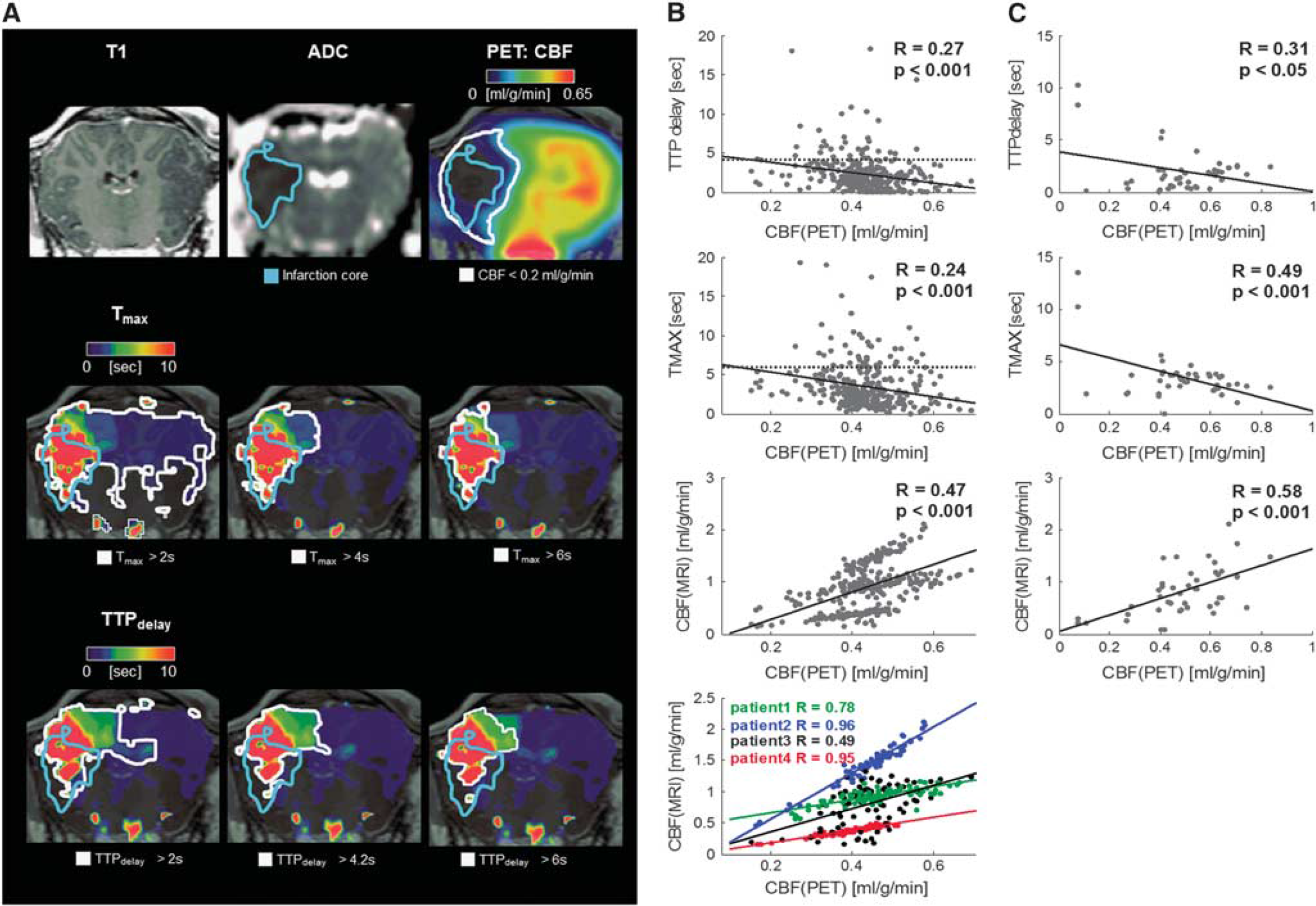
In addition, three merino sheep with pMCAO underwent simultaneous [ 15 O]H2O PET/MRI. Perfusion[PET] and perfusion[MRI] image data 4.5 hours after pMCAO in a sheep are provided in Figure 2. Here, a considerable difference between the PET penumbra and the MR penumbra was observed, and the application of alternative PW MR thresholds did not lead to perfusion[MRI] maps similar to the perfusion[PET] maps.
(
Supplementary Figures 2 and 3 provide an overview on the individual image data obtained in sheep and humans. In four human patients, arterial cannulation allowed to establish an arterial input function for full kinetic modeling of the dynamic PET data for absolute perfusion[PET] quantification. The CBF values in the unaffected cerebral hemispheres were 0.43 ± 0.03 mL/g per minute for gray matter and 0.23 ± 0.03 mL/g per minute for white matter. On a regional brain level, linear relation between pooled perfusion[PET] and perfusion[MRI] in stroke patients was weak to moderate for Tmax/TTPdelay/CBF (
DISCUSSION
We were able to demonstrate for the first time that simultaneous [ 15 O]H2O PET/MRI is feasible in a large animal stroke model and in a clinical acute stroke setting without significantly delaying diagnostic MRI routines and without compromising standard MRI diagnosis. Compared with sequential studies, the comparability of perfusion[MRI] and perfusion[PET] is not only improved by simultaneous data acquisition, but also by the inherent spatial image data match. Gray matter and white matter CBF values as measured by the PET component of the integrated PET/MRI system were in good agreement with values reported in the literature.11–13 Furthermore, the diagnostic quality of the obtained MRI data was not affected by the concurrent PET data acquisition.
Notably, we observed limited correspondence between perfusion[PET] and perfusion[MRI] on an pooled basis with a higher variability of MRI-based blood flow estimates as compared with the gold standard PET-based CBF values in human patients and sheep. In pooled regression analyses of PWI CBF and PET CBF in prior sequential PET/MRI studies,
The grouped quantitative differences observed in this study cannot anymore be related to a different disease state after an imaging delay ~1 hour between sequential PET and MRI perfusion measures.10,14–16 These differences must solely be because of the different nature of the imaging modalities and are potentially related to the nonlinear relation between signal intensity and the concentration of the contrast agent in MRI and to the fact that gadolinium is an intravascular contrast agent, whereas [ 15 O]H2O is freely diffusible. Both shortcomings can lead to an incorrect patient selection for late thrombolysis in PW MRI. 8 Arterial spin labeling (ASL), a more recently developed MRI perfusion measurement technique as compared with PW MRI, better corresponds to [ 15 O]H2O PET CBF and has recently been shown to correlate well with the PET CBF measure in healthy young humans. 17 However, exact ASL measurements require prior knowledge about the degree of perfusion disturbance, which makes it hard to implement in the diseased brain. Future translational studies in larger cohorts will have to elucidate the exact relationship between perfusion[PET] and perfusion[MRI] and to possibly correct perfusion[MRI] by factors obtained from this head-to-head PET versus MRI comparison. In our view, simultaneous PET/MRI studies could possibly deliver a nonlinear correction function to derive a pseudo-CBF from time-based MR variables in the future.
As a limitation of this present study, the PET attenuation correction (see Supplementary Methods), as currently implemented in this hybrid PET/MR system, is still suboptimal and can lead to underestimations of the PET signal in the vicinity of cortical bone. 18 Further, in the sheep data, spatial distortion of perfusion [MRI] and DWI was present but was not corrected in this pilot study. This may have affected region of interest overlap and quantitative results in the animal experiments. Moreover, we mainly examined mildly affected patients at relatively late time points after stroke onset at which penumbral tissue cannot necessarily be expected anymore. Moreover, the variety of disease etiologies, ranging from, e.g., lacunar infarctions over cerebral bleeding to typical MCA territory infarctions, poses another drawback. This may have contributed to the correlations found in this present study, which are not stronger between perfusion[PET] and perfusion[MRI] as compared with those reported in prior sequential studies with more homogenous patient collectives.10,15 Further, it would be desirable to measure the oxygen extraction fraction (OEF) as the gold standard PET technique to delineate the ischemic penumbra by means of PET 2 also in a simultaneous PET/MRI environment. Because of the fact that an MR-compatible multitracer administration equipment, which needs to be operated close to the patient to achieve OEF measurements, is currently not available, we focused our research on one—if not the (with regard to pathogenesis and therapy decisions) decisive aspect of ischemic stroke pathophysiology, i.e., measuring CBF. It will remain the task of future investigations with more advanced technical opportunities to relate the PW/DW mismatch MRI penumbra concept against simultaneous OEF CBF PET measurements. Those investigations will then, by providing the full picture, potentially offer the optimization of stroke MR imaging, for instance by the introduction of PW MR CBF correction factors.
Taken together, combined PET/MRI is a promising tool for validating MR-based stroke imaging concepts and provides excellent preclinical stroke imaging opportunities to improve the assessment of novel diagnostic and therapeutic concepts. As such, hybrid PET/MRI provides the opportunity to obtain synergistic PET data during standard stroke MRI, which then may guide individual treatment decisions, for instance within therapeutic trials, more precisely.
DISCLOSURE/CONFLICT OF INTEREST
HB and OS served as consultants and speakers for Bayer Healthcare and Piramal Imaging. OS served as primary investigator for Bayer Healthcare, Piramal Imaging, Siemens Healthcare, and GE Healthcare. HB and OS received speaker honoraria from Siemens Healthcare. K-TH served as speaker for Bayer Healthcare and Bracco.
Footnotes
ACKNOWLEDGMENTS
The authors thank Julian Klingbeil for patient recruitment. The authors are particularly grateful for the invaluable support of Torsten Böhm, Tanja Uhlisch, and Tanja Winkler in patient preparation and PET/MRI data acquisition. The cyclotron and radio-pharmacy staff of the Department of Nuclear Medicine is greatly acknowledged for radiotracer production.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.