
Abstract
Delayed cerebral ischemia (DCI) after aneurysmal subarachnoid hemorrhage (aSAH) has been associated with microthrombosis, which can result from activated hemostasis, inhibited fibrinolysis, or both. We systematically searched the PUBMED and EMBASE databases to identify hemostatic or fibrinolytic parameters that can be used for the prediction or diagnosis of DCI, or that inform on the pathogenesis of DCI and may serve as treatment targets. We included 24 studies that fulfilled predefined criteria and described 39 biomarkers. Only one study fulfilled predefined criteria for high quality. Since no parameter on admission was associated with DCI and in none of the included studies blood was drawn at the time of clinical deterioration, none of the studied parameters can presently be used for the prediction or diagnosis of DCI. Regarding the pathogenesis of DCI, it was shown that compared with patients without DCI those with DCI had higher levels of von Willebrand factor and platelet activating factor in plasma 5 to 9 days after aSAH, membrane tissue factor in cerebrospinal fluid 5 to 9 days after aSAH, and D-dimer in plasma 11 to 14 days after aSAH. Confirmation in high-quality studies is needed to investigate whether these parameters can serve as targets for new intervention studies.
Keywords
INTRODUCTION
Delayed cerebral ischemia (DCI) is one of the most feared complications after aneurysmal subarachnoid hemorrhage (aSAH), occurring in approximately 30% of patients. 1 Patients with DCI develop uni- or multifocal areas of ischemia mostly between days 4 and 14 after the hemorrhage, which are not confined to the arterial supply or borderzone territories. Unlike thrombo-embolic or hemodynamic stroke where the onset is immediate and patients seldomly lose consciousness, in DCI the onset of symptoms is gradual, often waxing and waning, and frequently also involves a decreased level of consciousness.
The prediction and diagnosis of DCI are difficult. Recently, it was shown that absolute risks of DCI-related infarction can be estimated by a simple risk chart that includes several admission characteristics. 2 However, the discriminative ability of the model was far from excellent. The diagnosis of DCI is challenging because clinical deterioration after aSAH can also have other etiologies, such as hydrocephalus, rebleeding, metabolic disturbances, or infections. Computed tomography (CT) perfusion is a promising tool for the diagnosis of DCI, but test characteristics of perfusion thresholds are moderate. 3 In addition, the pathogenesis of DCI has not been elucidated. For long it has been thought that DCI is caused by vasospasm of the arteries of the circle of Willis to such an extent that the term vasospasm was used as a synonym for DCI. Currently, it is assumed that the pathogenesis is multifactorial.4–6 Several studies suggested that besides arterial narrowing, microthrombosis is involved in the pathogenesis of DCI.7–12 Micro-thrombi mostly consist of aggregated platelets and fibrin, often mixed with leukocytes. 8 The formation of these thrombi results from the activation of primary and secondary hemostatic pathways, inhibition of fibrinolysis, or both. Primary hemostasis involves activation of the endothelium with release and exposure of von Willebrand factor (vWF) and subsequent platelet recruitment, activation, and aggregation. Secondary hemostasis involves the stabilization of the platelet plug by a fibrin meshwork mediated by a coagulation cascade. 7 Fibrinolysis involves the breakdown of a fibrin clot.
Because of these challenges in the prediction, diagnosis, and pathogenesis of DCI, the use of biomarkers is appealing. Many studies investigated quantitative differences in hemostatic- and fibrinolytic parameters in plasma and cerebrospinal fluid (CSF) in patients with and without DCI. Our aim was to systematically search the literature to identify hemostatic or fibrinolytic parameters that can be used for the prediction or diagnosis of DCI, or that provide clues on the pathogenesis of DCI and may serve as treatment targets.
MATERIALS AND METHODS
We systematically searched the PUBMED and EMBASE databases and hand-searched citations for studies reporting on hemostatic-and fibrinolytic parameters in plasma and CSF in patients with and without DCI (for search syntax see Appendix 1; last updated 4 March 2013). Manuscripts were included if: (1) ≥ 10 patients with aneurysmal SAH were studied; (2) clinical deterioration due to DCI (defined as a new focal deficit, decrease of consciousness, or both, which could not be attributed to another cause such as rebleeding, hydrocephalus, infection, etc.) 13 or cerebral infarction due to DCI (a new infarct on brain imaging that was not visible on the admission or on early postoperative scan) 13 was reported as an outcome measure; (3) hemostatic or fibrinolytic parameters were compared between aSAH patients with and without DCI; and (4) the study was written in English, French, German, or Dutch. Since considerable inconsistency exists in the use of terms and definitions to describe DCI after SAH, 13 we decided a priori to include studies using the following terms as an outcome measure: delayed ischemic neurologic deficit, delayed ischemic deficit, delayed neurologic deficit, secondary cerebral ischemia, clinical vasospasm, symptomatic vasospasm, symptomatic ischemia, and cerebral infarction. Studies that had ‘vasospasm’ as an outcome measure were only included if it was defined as any kind of clinical deterioration. Studies were excluded if: (1) angiographic or transcranial Doppler (TCD) vasospasm was the only outcome measure; (2) levels of hemostatic/fibrinolytic parameters were likely to be influenced by medical treatment, such as antifibrinolytic drugs; or (3) cerebral infarction due to DCI was the outcome measure but imaging was performed more than 3 months after SAH. All abstracts, and if inconclusive, the full text article was screened for inclusion criteria. The search strategy and manuscript selection was performed by one author (JB). Data extraction was performed by two review authors (JB and MDIV), independent from each other. Differences in extracted data were solved in a consensus meeting. Since most studies did not correct for baseline parameters, we only reported crude values of hemostatic and fibrinolytic parameters. If an included study made distinction between spontaneous DCI and DCI including procedure-related ischemic events, then we only included data on spontaneous DCI. Since the aim of the study was to identify parameters for the prediction, diagnosis, or pathogenesis of DCI, we only included samples that were taken within 14 days after aSAH. If a research group reported on the same parameters in more than one publication and it could not be ruled out that patient populations were overlapping, then we used the study with the largest number of patients.
Quality Assessment and Level of Evidence
A quality assessment was performed using an adapted version of a scoring system used in a recent systematic review on prognostic factors for DCI (Table 1). 14 A score of 12 to 17 was considered as a high quality, and a score of < 12 a low quality study. Subsequently, we assessed the level of evidence based on study quality and consistency for each hemostatic and fibrinolytic parameter (Figure 1). Level of evidence was categorized into strong, moderate, weak, low, or inconsistent.
Scoring sheet for quality assessment
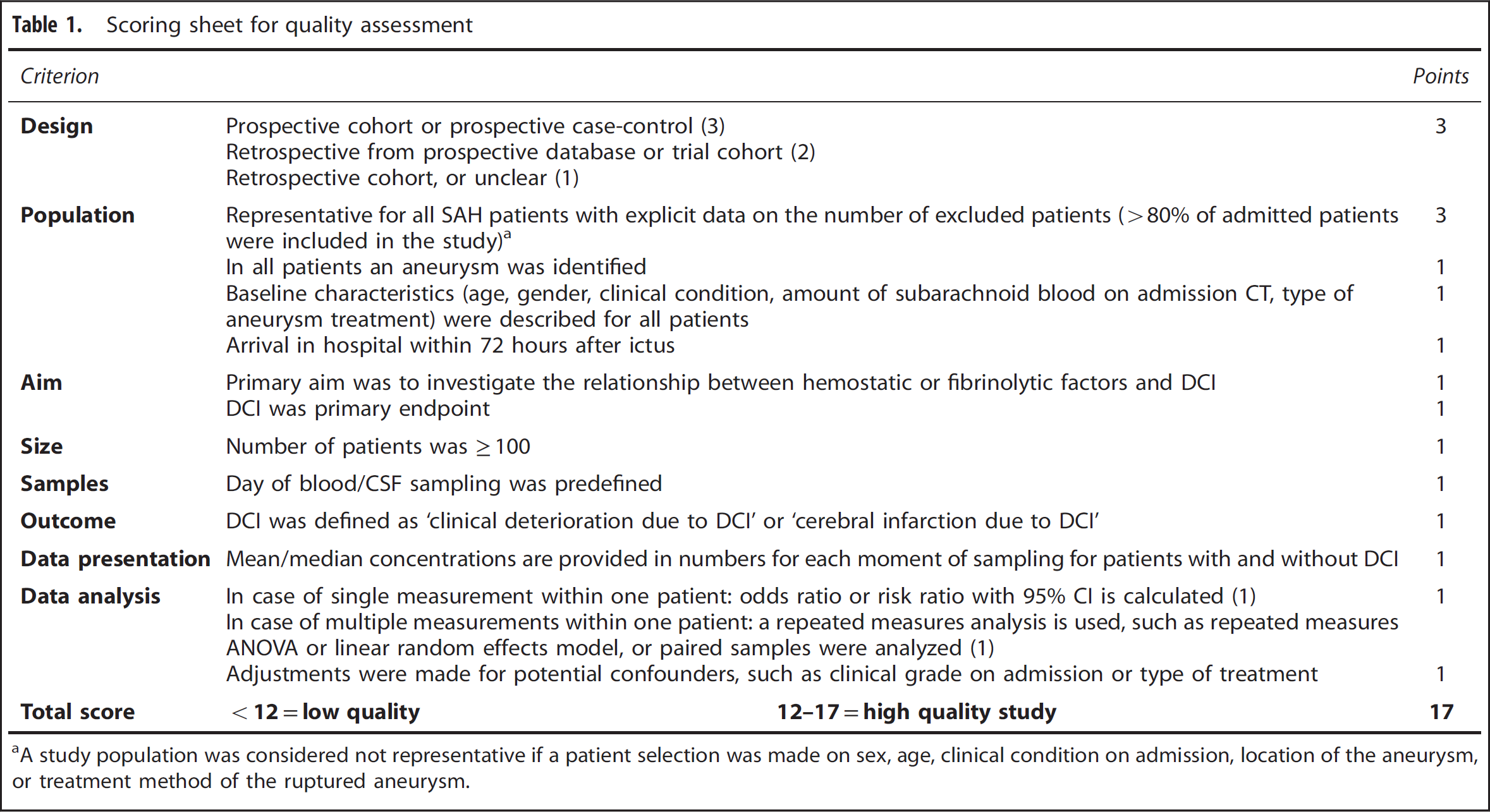
A study population was considered not representative if a patient selection was made on sex, age, clinical condition on admission, location of the aneurysm, or treatment method of the ruptured aneurysm.
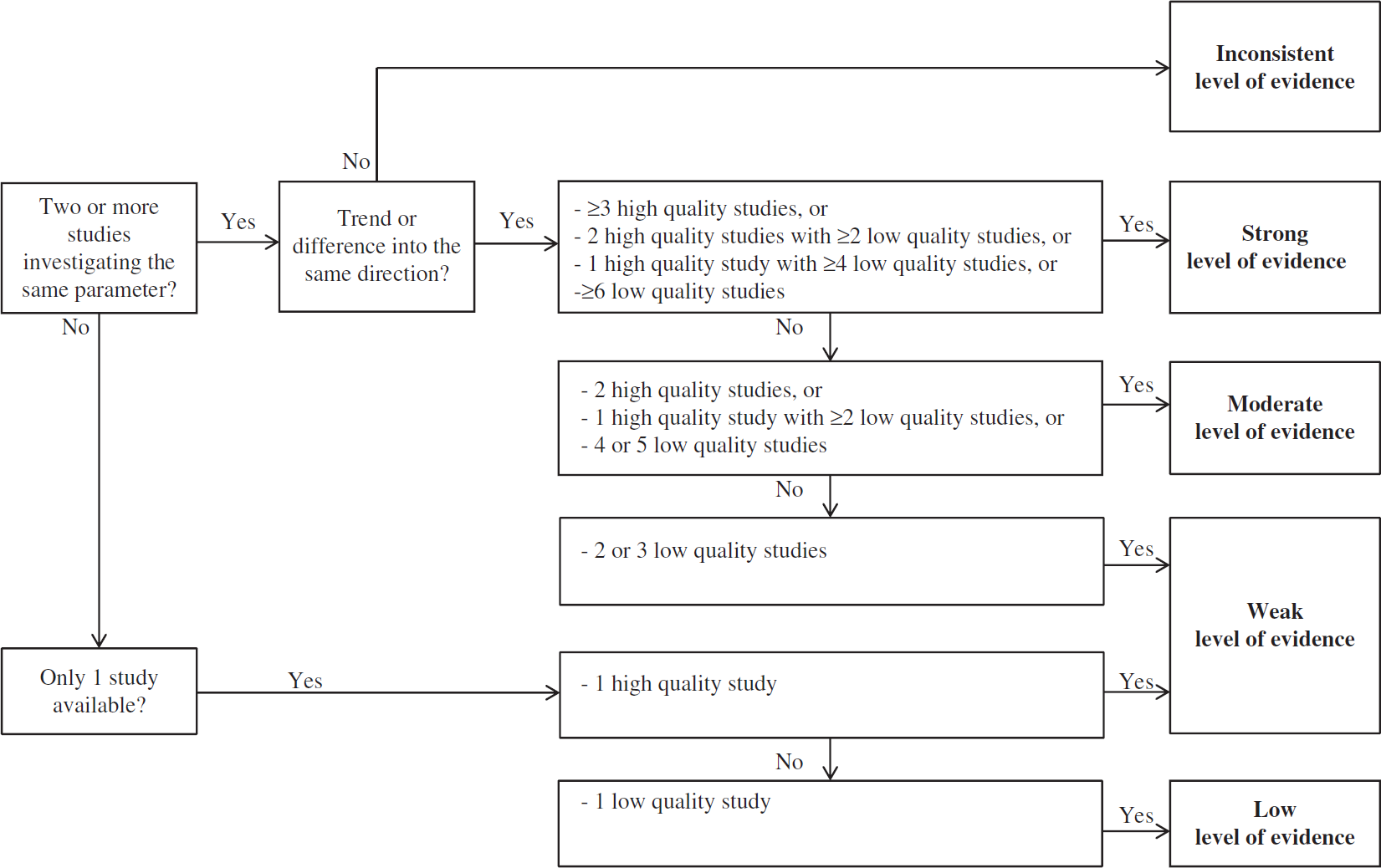
Categories for level of evidence.
Analyses
Hemostatic and fibrinolytic parameters were categorized into parameters of (1) primary hemostasis in plasma; (2) secondary hemostasis in plasma; (3) fibrinolysis in plasma; (4) antiphospholipid antibodies (which interfere with coagulation leading to increased clot formation); and (5) primary hemostasis, secondary hemostasis, and fibrinolysis in CSF. We aimed to perform metaanalyses by pooling data for each parameter with a strong or moderate level of evidence, if analyzed with similar assays, by calculating and comparing means with standard deviations in patients with and without DCI. Separate analyses were performed for prediction, diagnosis, and pathogenesis of DCI. For prediction of DCI, we only included studies investigating hemostatic or fibrinolytic parameters on admission (defined as < 24 hours after admission or at day 0). For diagnosis of DCI, we included studies reporting on blood or CSF samples that were withdrawn at the moment patients started to have symptoms of clinical deterioration due to DCI. For pathogenesis of DCI, we included studies reporting on samples that were drawn during the time course of DCI, defined as 4 to 14 days after SAH.
RESULTS
Overview Included Studies
Our search strategy yielded 362 articles, of which 340 manuscripts were excluded (Figure 2). After screening of reference lists, two additional manuscripts were retrieved so that 24 articles were finally included.15–38 Baseline characteristics of the included studies are described in Table 2. The median number of patients per study was 51 (range 19 to 511). In 7 of the 24 studies the majority of patients was male.15,16,22,25,27,30,35 in all but one study, 33 clipping of the aneurysm was the most commonly used or only modality for aneurysm treatment. Day of aneurysm treatment ranged from a median of day 0 to a median of 7.5 days after SAH. Many different definitions for DCI were used; many studies explicitly stated that DCI was diagnosed after exclusion of procedure-related complications. Timing of blood and CSF sampling differed widely among studies and mostly was not standardized.
Baseline characteristics of included studies
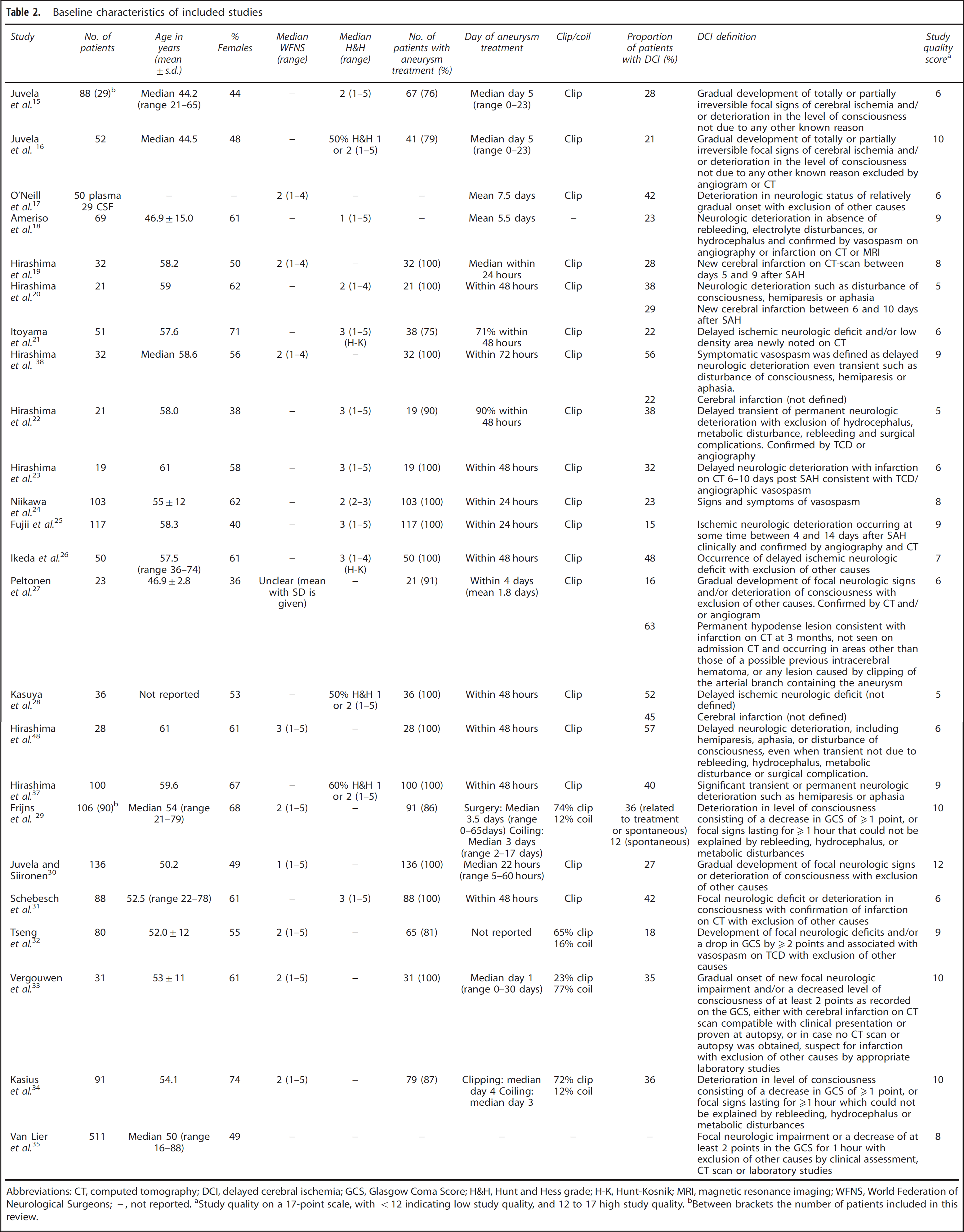
Abbreviations: CT, computed tomography; DCI, delayed cerebral ischemia; GCS, Glasgow Coma Score; H&H, Hunt and Hess grade; H-K, Hunt-Kosnik; MRI, magnetic resonance imaging; WFNS, World Federation of Neurological Surgeons; −, not reported.
Study quality on a 17-point scale, with <12 indicating low study quality, and 12 to 17 high study quality.
Between brackets the number of patients included in this review.
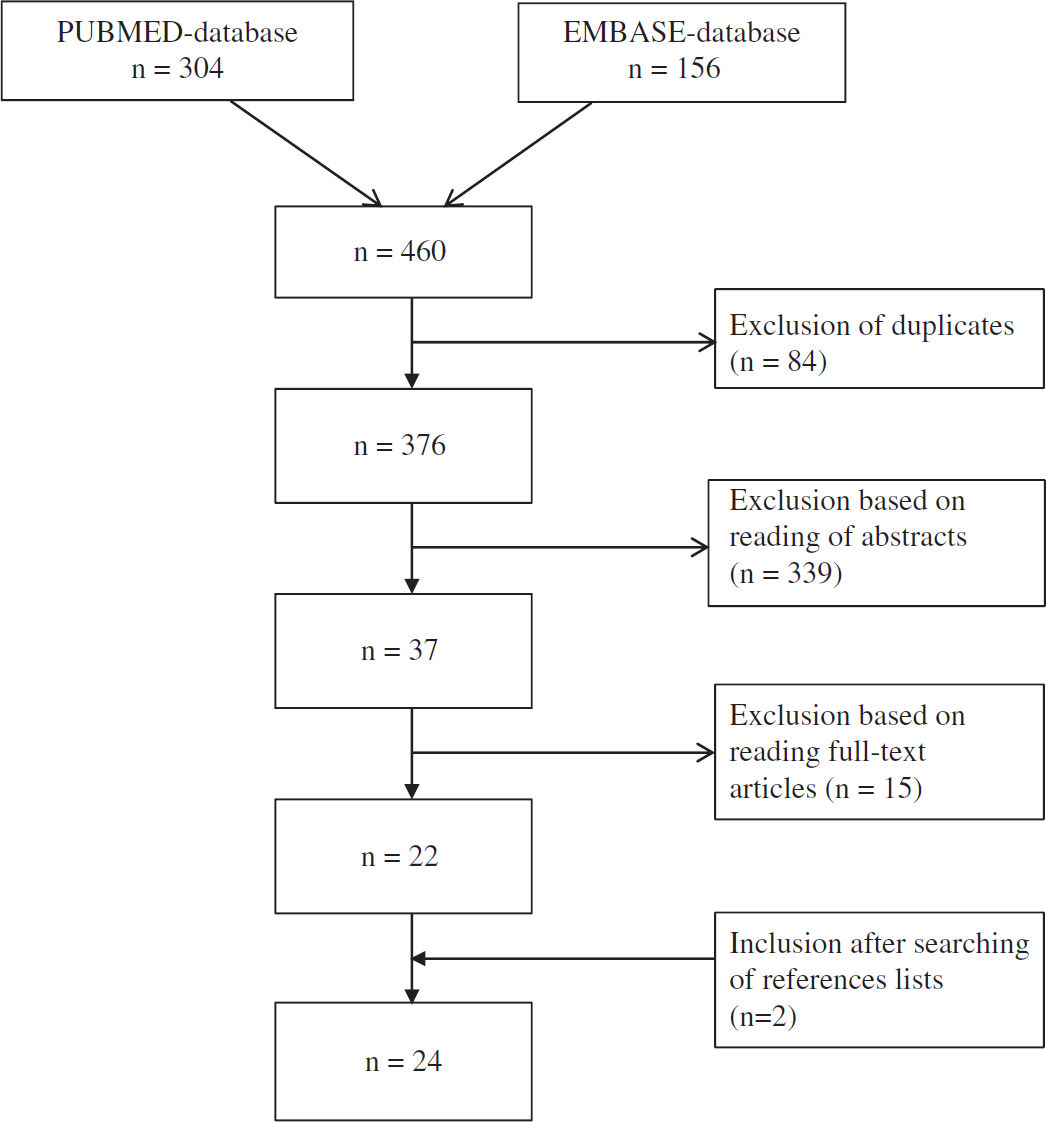
Study selection.
Quality Assessment
Study quality was high (12 points) in only one study (Table 2). 30
Meta-Analysis
The relationship with DCI was studied in 11 studies with low quality on parameters of primary hemostasis in plasma (Table 3),15,16,19,21,24,25,29,31,33,34,37 in eight studies with low quality on parameters of secondary hemostasis in plasma (Table 4),17,18,21,22,25–27,32 in seven studies, including one high quality and six low quality studies, on fibrinolytic parameters in plasma (Table 5),18,21,25–27,30,32 in four low quality studies on antiphospolipid antibodies in plasma (Table 6),18,19,35,38 and in six low quality studies on hemostatic and fibrinolytic parameters and DCI in CSF (Table 7).17,19,23,26,28,36 Meta-analyses were not performed since no parameters were found with a moderate or strong level of evidence. In addition, different assays were used to measure hemostatic and fibrinolytic parameters. Therefore, results of studies are descriptively summarized.
Plasma parameters of primary hemostasis in patients with DCI compared with patients without DCI
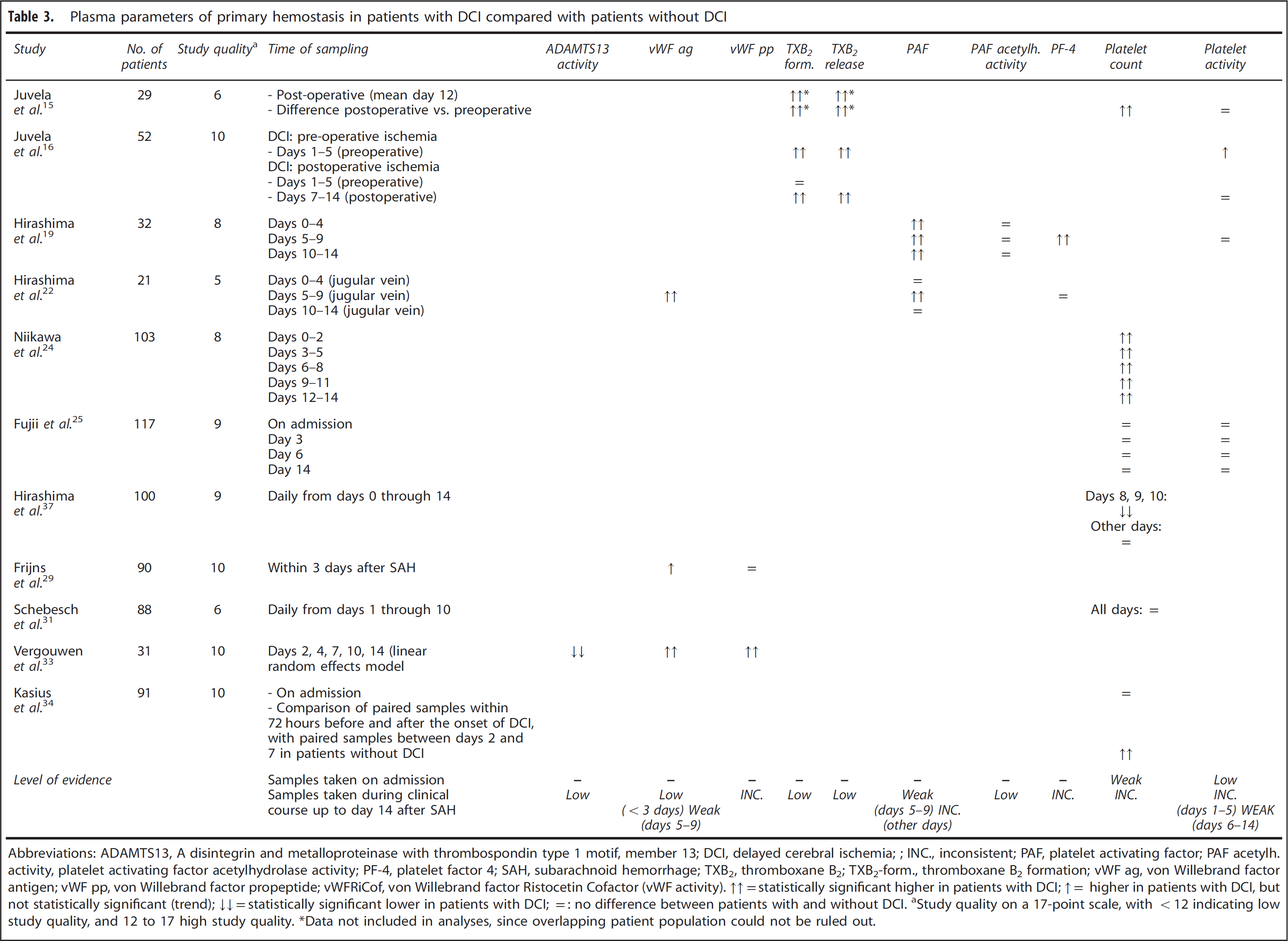
Abbreviations: ADAMTS13, A disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; DCI, delayed cerebral ischemia;; INC., inconsistent; PAF, platelet activating factor; PAF acetylh. activity, platelet activating factor acetylhydrolase activity; PF-4, platelet factor 4; SAH, subarachnoid hemorrhage; TXB2, thromboxane B2; TXB2-form., thromboxane B2 formation; vWF ag, von Willebrand factor antigen; vWF pp, von Willebrand factor propeptide; vWFRiCof, von Willebrand factor Ristocetin Cofactor (vWF activity).
statistically significant higher in patients with DCI;
higher in patients with DCI, but not statistically significant (trend);
statistically significant lower in patients with DCI;
no difference between patients with and without DCI.
Study quality on a 17-point scale, with <12 indicating low study quality, and 12 to 17 high study quality.
Data not included in analyses, since overlapping patient population could not be ruled out.
Plasma parameters of secondary hemostasis in patients with DCI compared with patients without DCI
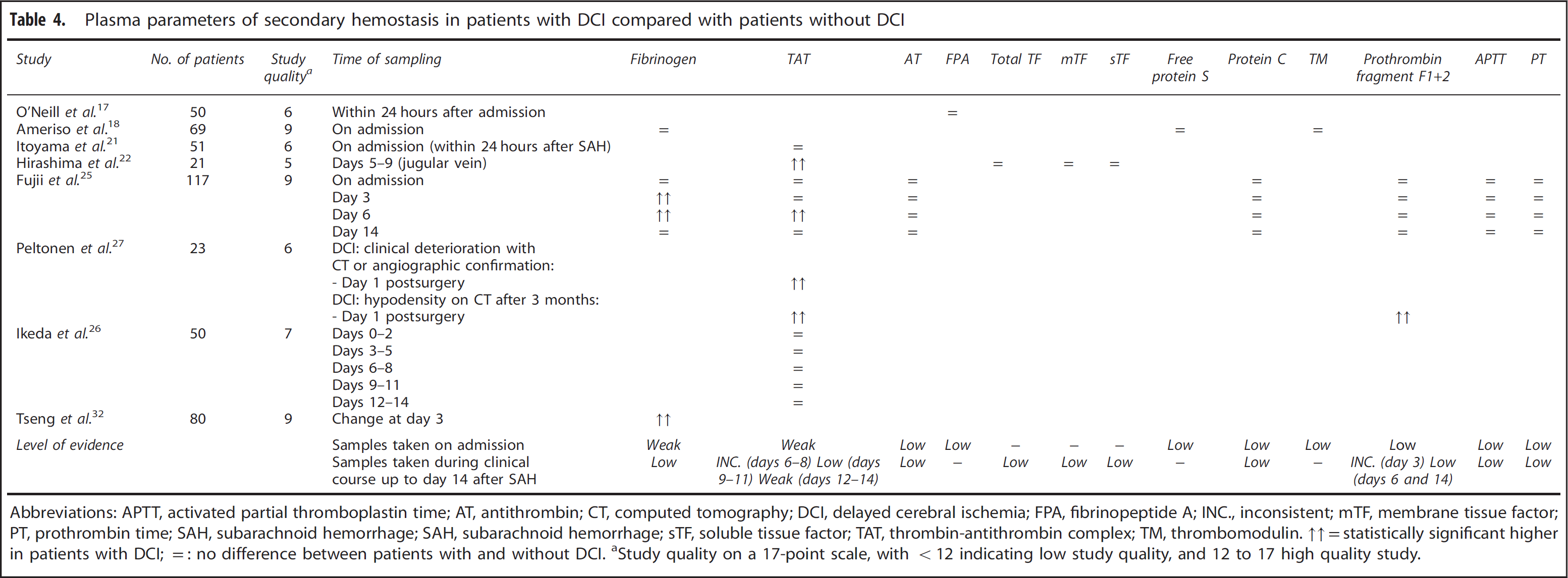
Abbreviations: APTT, activated partial thromboplastin time; AT, antithrombin; CT, computed tomography; DCI, delayed cerebral ischemia; FPA, fibrinopeptide A; INC., inconsistent; mTF, membrane tissue factor; PT, prothrombin time; SAH, subarachnoid hemorrhage; SAH, subarachnoid hemorrhage; sTF, soluble tissue factor; TAT, thrombin-antithrombin complex; TM, thrombomodulin.
statistically significant higher in patients with DCI;
no difference between patients with and without DCI.
Study quality on a 17-point scale, with <12 indicating low study quality, and 12 to 17 high quality study.
Plasma parameters of fibrinolysis in patients with DCI compared with patients without DCI
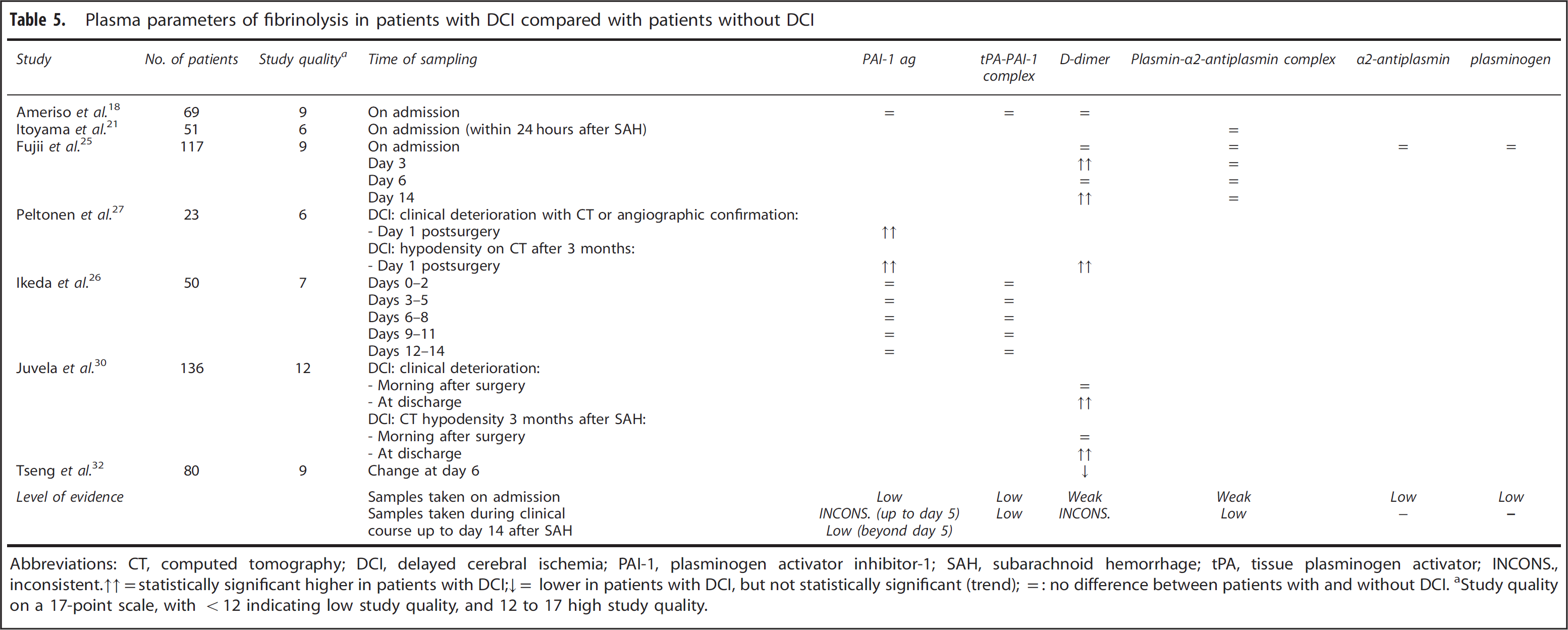
Abbreviations: CT, computed tomography; DCI, delayed cerebral ischemia; PAI-1, plasminogen activator inhibitor-1; SAH, subarachnoid hemorrhage; tPA, tissue plasminogen activator; INCONS., inconsistent.↑↑=statistically significant higher in patients with DCI;↓= lower in patients with DCI, but not statistically significant (trend); =: no difference between patients with and without DCI.
Study quality on a 17-point scale, with <12 indicating low study quality, and 12 to 17 high study quality.
Plasma antiphospholipid antibodies in patients with DCI compared with patients without DCI
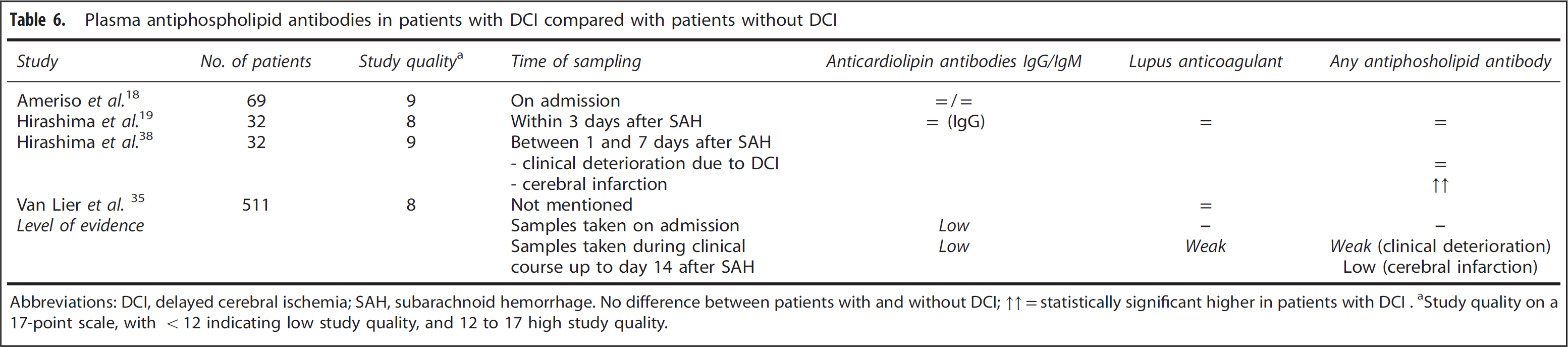
Abbreviations: DCI, delayed cerebral ischemia; SAH, subarachnoid hemorrhage.
No difference between patients with and without DCI; ↑↑=statistically significant higher in patients with DCI.
Study quality on a 17-point scale, with <12 indicating low study quality, and 12 to 17 high study quality.
Cerebrospinal fluid parameters in patients with DCI compared with patients without DCI
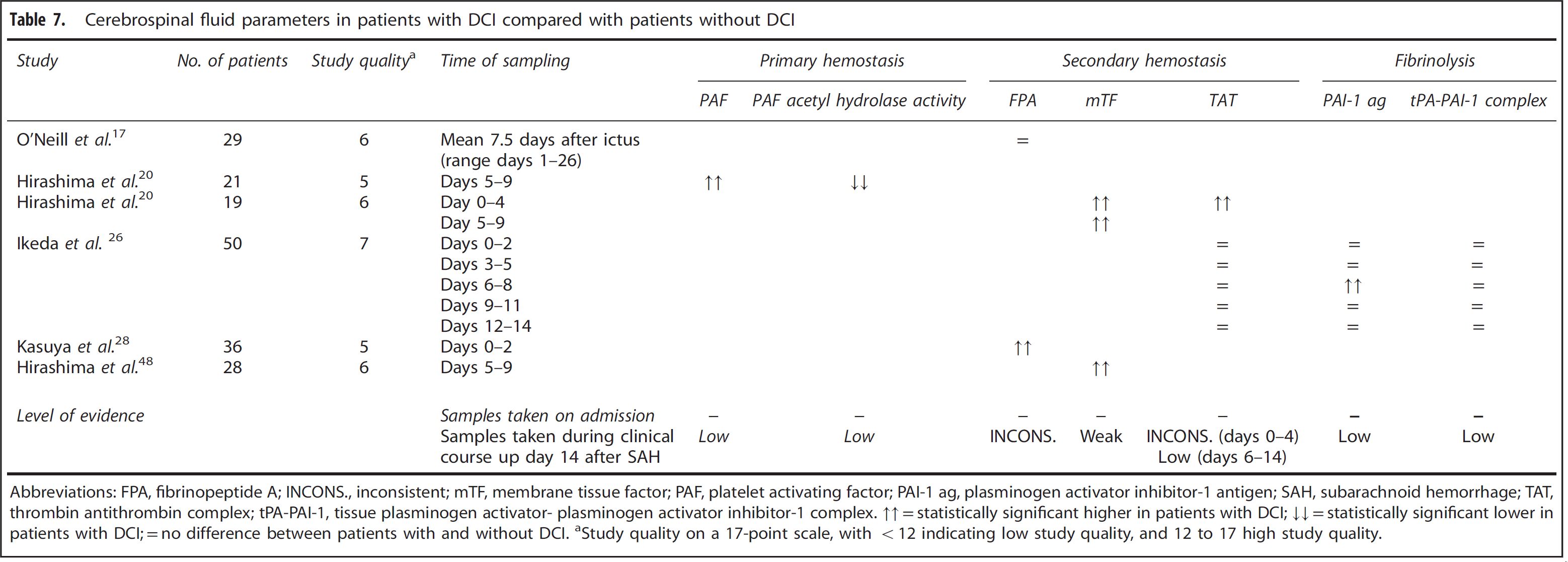
Abbreviations: FPA, fibrinopeptide A; INCONS., inconsistent; mTF, membrane tissue factor; PAF, platelet activating factor; PAI-1 ag, plasminogen activator inhibitor-1 antigen; SAH, subarachnoid hemorrhage; TAT, thrombin antithrombin complex; tPA-PAI-1, tissue plasminogen activator- plasminogen activator inhibitor-1 complex.
statistically significant higher in patients with DCI;
statistically significant lower in patients with DCI;
no difference between patients with and without DCI.
Study quality on a 17-point scale, with <12 indicating low study quality, and 12 to 17 high study quality.
Prediction of Delayed Cerebral Ischemia
No association was found between any hemostatic or fibrinolytic parameter in plasma on admission with later development of DCI (low or weak level of evidence) (Tables 3, 4, 5, 6).17,18,21,25 None of the studies analysed CSF parameters on admission in relationship with DCI (Table 7).
Diagnosis of Delayed Cerebral Ischemia
In none of the included studies blood or CSF was withdrawn at the moment patients started to have symptoms of clinical deterioration due to DCI.
Pathogenesis of Delayed Cerebral Ischemia
A weak level of evidence was found for involvement of vWF and platelet activating factor in plasma 5 to 9 days after aSAH (Table 3), membrane tissue factor in CSF 5 to 9 days after aSAH (Table 7), and D-dimer in plasma 11 to 14 days after aSAH (Table 5). For other parameters either an association was found with a low level of evidence, no association was found, or conflicting data were available (Tables 3, 4, 5, 6, 7).
DISCUSSION
The results of this systematic review show that none of the studied parameters can presently be used for the prediction or diagnosis of DCI. Regarding the pathogenesis of DCI, it was shown that patients with DCI have higher levels of vWF and platelet activating factor in plasma 5 to 9 days after aSAH, membrane tissue factor in CSF 5 to 9 days after aSAH, and D-dimer in plasma 11 to 14 days after aSAH, compared with patients without DCI. However, because of the poor study quality and the small number of studies investigating these relationships, the level of evidence for these associations was weak.
We are aware of only one other systematic review addressing the relationship between laboratory hemostatic parameters with DCI, which also found that platelet count was not predictive for the development of DCI. 14 No other laboratory parameters related to hemostasis and fibrinolysis were included in the previous review.
Regarding the pathogenesis of DCI, our data showed that patients with DCI have higher levels of vWF and platelet activating factor 5 to 9 days after SAH, compared with patients without DCI. These data suggest that treatments affecting platelet aggregation hold promise. In clinical studies, antiplatelet drugs tended to decrease the proportion of patients with DCI. 39 However, this beneficial effect was offset by more hemorrhagic complications. 39 Therefore, treatments that affect platelet aggregation without increasing the risk of hemorrhagic complications might be more promising. Two recent studies showed that recombinant ADAMTS13 reduces microthrombosis and brain injury after experimental SAH.40–41 ADAMTS13 rapidly cleaves ultralarge vWF multimers, reduces platelet adhesion and aggregation, and downregulates inflammation and thrombus formation.42–45 In stroke models, recombinant ADAMTS13 did not affect bleeding rates.41,46,47 Previously, it was shown that treatment with a platelet activating factor antagonist is safe in patients with aSAH; however, no randomized controlled trials have been performed with this drug. 48
Our data also showed that patients with DCI have higher levels of membrane tissue factor in CSF 5 to 9 days after aSAH, compared with patients without DCI. It has been hypothesized that the adventitial surface of cerebral arterioles releases tissue factor in response to an inflammatory response in the subarachnoid space after aSAH, and that sufficient tissue factor activation causes a focal type of disseminated intravascular coagulation. 9 Since direct inhibition of the tissue factor pathway might result in more bleeding complications, 49 indirect inhibition through suppression of the inflammatory response in the subarachnoid space might be more promising.
The significance of the increased D-dimer level 11 to 14 days after SAH in patients with DCI remains unclear. This parameter becomes elevated in plasma when a blood clot is degraded by fibrinolysis. Since increased D-dimer is a rather nonspecific measure for both increased thrombosis and fibrinolysis, this finding does not provide information that can be used for specific treatment targets.
Some limitations need to be addressed. First, since most of the studies had a retrospective design and included small numbers of patients with DCI, it is unlikely that these studies had sufficient power to detect significant differences in hemostatic and fibrinolytic parameters between patients developing DCI and those without DCI. Second, the included articles used many different terms and definitions to describe DCI. A proposal for a uniform definition of DCI was only published in 2010, 13 and since most included articles in this review were published before that time we decided not to use that definition for this review. Although definitions differed between studies, it does not affect internal validity within studies. In addition, since no pooling of data was performed, this probably did not affect our results considerably. Third, in none of the included studies blood or CSF was withdrawn at the moment patients started to have symptoms of clinical deterioration due to DCI. Therefore, it remains to be studied whether biomarkers can be used as a diagnostic tool to distinguish DCI from other causes of clinical deterioration. Fourth, in a third of the studies there was a male predominance, which suggests inclusion bias. Finally, selective reporting of data and publication bias could not be ruled out.
Implications for clinical practice are that presently no biomarkers related to hemostasis and fibrinolysis can be used for the prediction or diagnosis of DCI. Implications for research are that high-quality studies are needed, using a uniform definition of DCI, to confirm the association of several parameters with DCI and to investigate whether these parameters can serve as targets for new intervention studies.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.