
Abstract
As it is often assumed that delayed cerebral ischemia (DCI) after subarachnoid hemorrhage (SAH) is caused by vasospasm, clinical trials often focus on prevention of vasospasm with the aim to improve clinical outcome. However, the role of vasospasm in the pathogenesis of DCI and clinical outcome is possibly smaller than previously assumed. We performed a systematic review and meta-analysis on all randomized, double-blind, placebo-controlled trials that studied the effect of pharmaceutical preventive strategies on vasospasm, DCI, and clinical outcome in SAH patients to further investigate the relationship between vasospasm and clinical outcome. Effect sizes were expressed in pooled risk ratio (RR) estimates with corresponding 95% confidence intervals (CI). A total of 14 studies randomizing 4,235 patients were included. Despite a reduction of vasospasm (RR 0.80 (95% CI 0.70 to 0.92)), no statistically significant effect on poor outcome was observed (RR 0.93 (95% CI 0.85 to 1.03)). The variety of DCI definitions did not justify pooling the DCI data. We conclude that pharmaceutical treatments have significantly decreased the incidence of vasospasm, but not of poor clinical outcome. This dissociation between vasospasm and clinical outcome could result from methodological problems, sample size, insensitivity of clinical outcome measures, or from mechanisms other than vasospasm that also contribute to poor outcome.
Introduction
Delayed cerebral ischemia (DCI) is a common complication of aneurysmal subarachnoid hemorrhage (SAH). Delayed cerebral ischemia can be reversible or it may progress to cerebral infarction. Cerebral infarction is associated with poor clinical outcome and death (Rabinstein et al, 2004). As vasospasm is strongly associated with DCI and clinical outcome, clinical trials in the last few decades focused on prevention of vasospasm with the aim to improve clinical outcome (Fergusen and Macdonald, 2007; Rosengart et al, 2007). Progress has been made. Meta-analysis of population-based studies of aneurysmal SAH found that mortality decreased by 50% in the last 2 decades, mostly due to improved in-hospital care (Lovelock et al, 2010). However, outcome remains poor, and some clinical trials designed to decrease vasospasm or DCI have not improved outcome after SAH (Macdonald et al, 2008). One reason for this may be that the role of vasospasm in the pathogenesis of DCI and clinical outcome is smaller than previously assumed, although the role of drug side effects and insensitive outcome measures has not been ruled out (Kreiter et al, 2009). To further investigate the relationship between vasospasm and clinical outcome, we pooled all randomized placebo-controlled trials that investigated pharmaceutical interventions as a preventive strategy in SAH patients.
Materials and methods
For this systematic review, the Cochrane Collaboration format was used (Higgins and Green, 2008).
Selection Criteria
Results
The initial search yielded 733 articles, of which 697 were excluded after review of titles and abstracts. Publications were usually excluded because the study was not a randomized trial or it did not include the relevant outcome events. The remaining 37 studies were randomized, double-blind, placebo-controlled trials of pharmaceutical preventive strategies in patients with aneurysmal SAH, although some studies included patients with spontaneous SAH and no identified source of hemorrhage. Finally, 14 trials with 4,235 patients had radiographic vasospasm, DCI, and clinical outcome as outcome events and were included in the analysis (Chou et al, 2008; Findlay et al, 1995; Haley Jr et al, 1993a, b , 1997; Kassell et al, 1996; Macdonald et al, 2008; Neil-Dwyer et al, 1987; Ono et al, 1984; Petruk et al, 1988; Philippon et al, 1986; Shibuya et al, 1992; Springborg et al, 2007; Tseng et al, 2005, 2007; Vergouwen et al, 2009). A total of 2,612 patients were randomized to pharmaceutical treatment and 1,623 patients to placebo. Funnel plots were not suggestive of publication bias (data not shown). Characteristics of the included studies are listed in the Table 1.
Characteristics of included studies
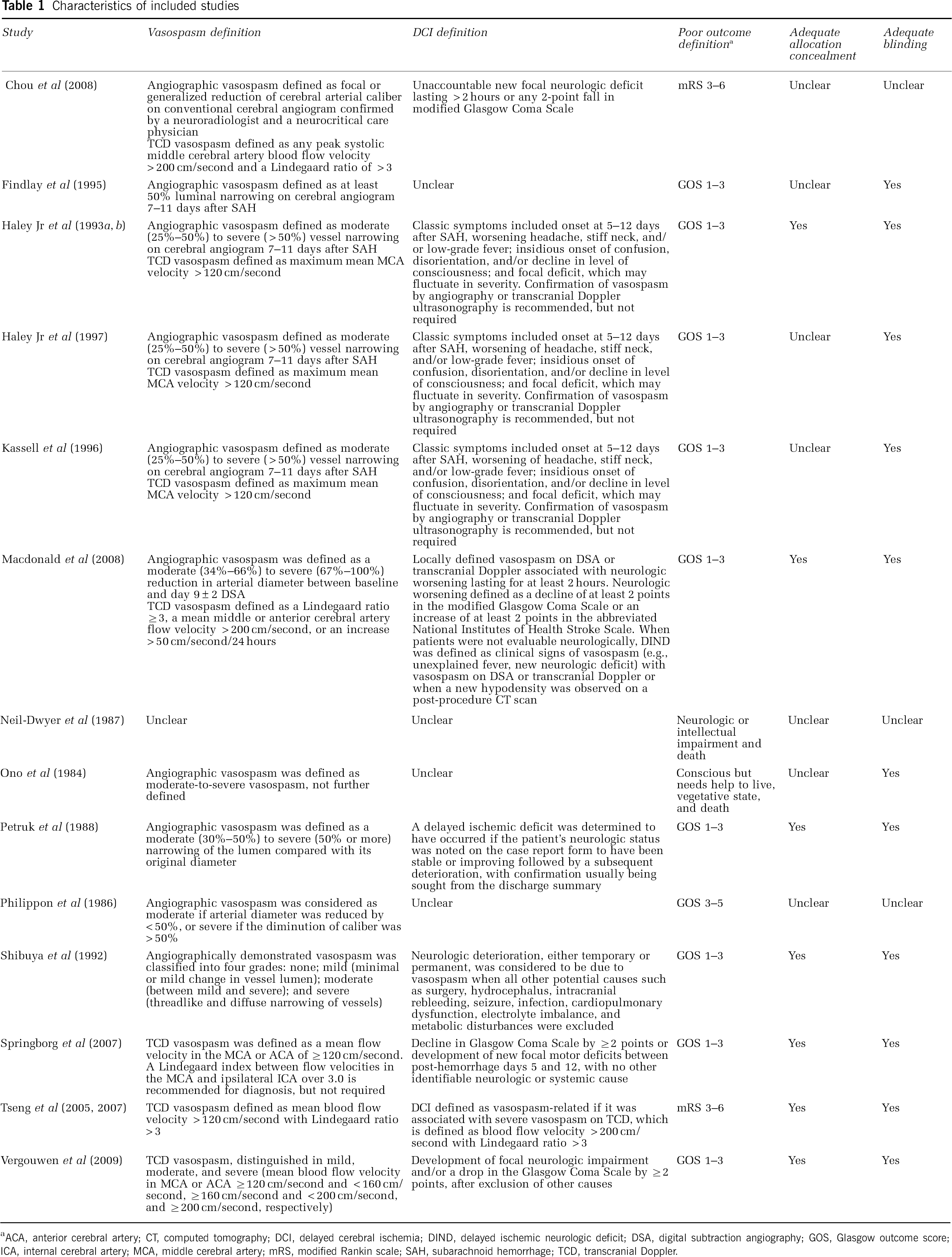
ACA, anterior cerebral artery; CT, computed tomography; DCI, delayed cerebral ischemia; DIND, delayed ischemic neurologic deficit; DSA, digital subtraction angiography; GOS, Glasgow outcome score; ICA, internal cerebral artery; MCA, middle cerebral artery; mRS, modified Rankin scale; SAH, subarachnoid hemorrhage; TCD, transcranial Doppler.
Analyses
Of 14 studies eventually included in the meta-analysis, three reported on TCD vasospasm only (Springborg et al, 2007; Tseng et al, 2005; Vergouwen et al, 2009), five on both TCD and angiographic vasospasm (Chou et al, 2008; Haley et al, 1993b, 1997; Kassell et al, 1996; Macdonald et al, 2008), five on angiographic vasospasm only (Findlay et al, 1995; Ono et al, 1984; Petruk et al, 1988; Philippon et al, 1986; Shibuya et al, 1992), and in one study it was unclear (Neil-Dwyer et al, 1987). For TCD vasospasm, various definitions and cutoff values were used for mean and peak blood flow velocity, with or without a Lindegaard ratio > 3 (Chou et al, 2008; Haley Jr et al, 1993b, 1997; Kassell et al, 1996; Macdonald et al, 2008; Springborg et al, 2007; Tseng et al, 2005; Vergouwen et al, 2009). In addition, for angiographic vasospasm, various definitions with different cutoff values and classifications for luminal narrowing and vasospasm severity were used (Table 1; Chou et al, 2008; Findlay et al, 1995; Haley Jr et al, 1993b, 1997; Kassell et al, 1996; Macdonald et al, 2008; Petruk et al, 1988; Philippon et al, 1986; Shibuya et al, 1992). The definition of vasospasm was unclear in two studies (Neil-Dwyer et al, 1987; Ono et al, 1984).
For the analysis of radiographic vasospasm, data from 2,819 patients were available (1,783 patients randomized to pharmaceutical treatment and 1,036 to placebo). The overall number of patients with radiographic vasospasm was 634 in the group of patients randomized to pharmaceutical treatment and 516 in the placebo group. Our meta-analysis including 14 trial arms demonstrated a significant and favorable effect of treatment, compared with the placebo, on angiographic vasospasm (pooled RR 0.80; 95% CI, 0.70 to 0.92). Heterogeneity between the trials was high (
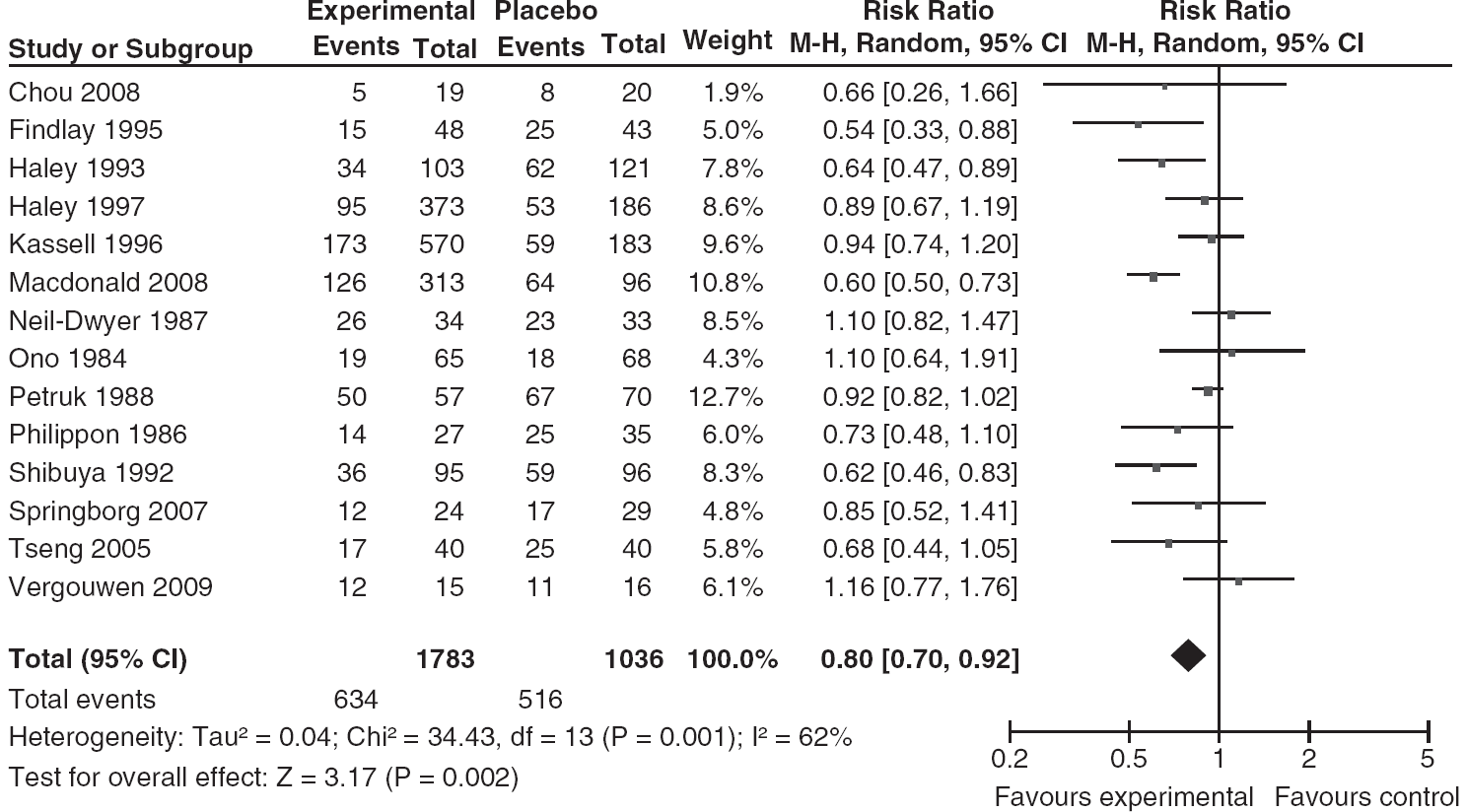
Pooled RR estimates for patients on pharmaceutical treatment found to have radiographic vasospasm.
Regarding DCI, there was a wide variation of definitions (Table 1). This variety of definitions did not justify pooling the DCI data.
For clinical outcome, most studies used the GOS (Findlay et al, 1995; Haley Jr et al, 1993a,
b
, 1997; Kassell et al, 1996; Macdonald et al, 2008; Petruk et al, 1988; Philippon et al, 1986; Shibuya et al, 1992; Springborg et al, 2007; Vergouwen et al, 2009) or mRS (Table 1; Chou et al, 2008; Tseng et al, 2005; Tseng et al, 2007). One study used an inverted GOS (Philippon et al, 1986). For the meta-analysis of poor clinical outcome, data from 4,211 patients were available (2,597 patients randomized to pharmaceutical treatment and 1,614 to placebo). The overall number of patients with poor outcome comprised 778 in the pharmaceutically treated group and 518 in the placebo group. Our meta-analysis including 14 trial arms did not show a significant effect of treatment, compared with the placebo, on poor clinical outcome (pooled RR 0.93; 95% CI, 0.85 to 1.03). Heterogeneity between the trials was not significant (
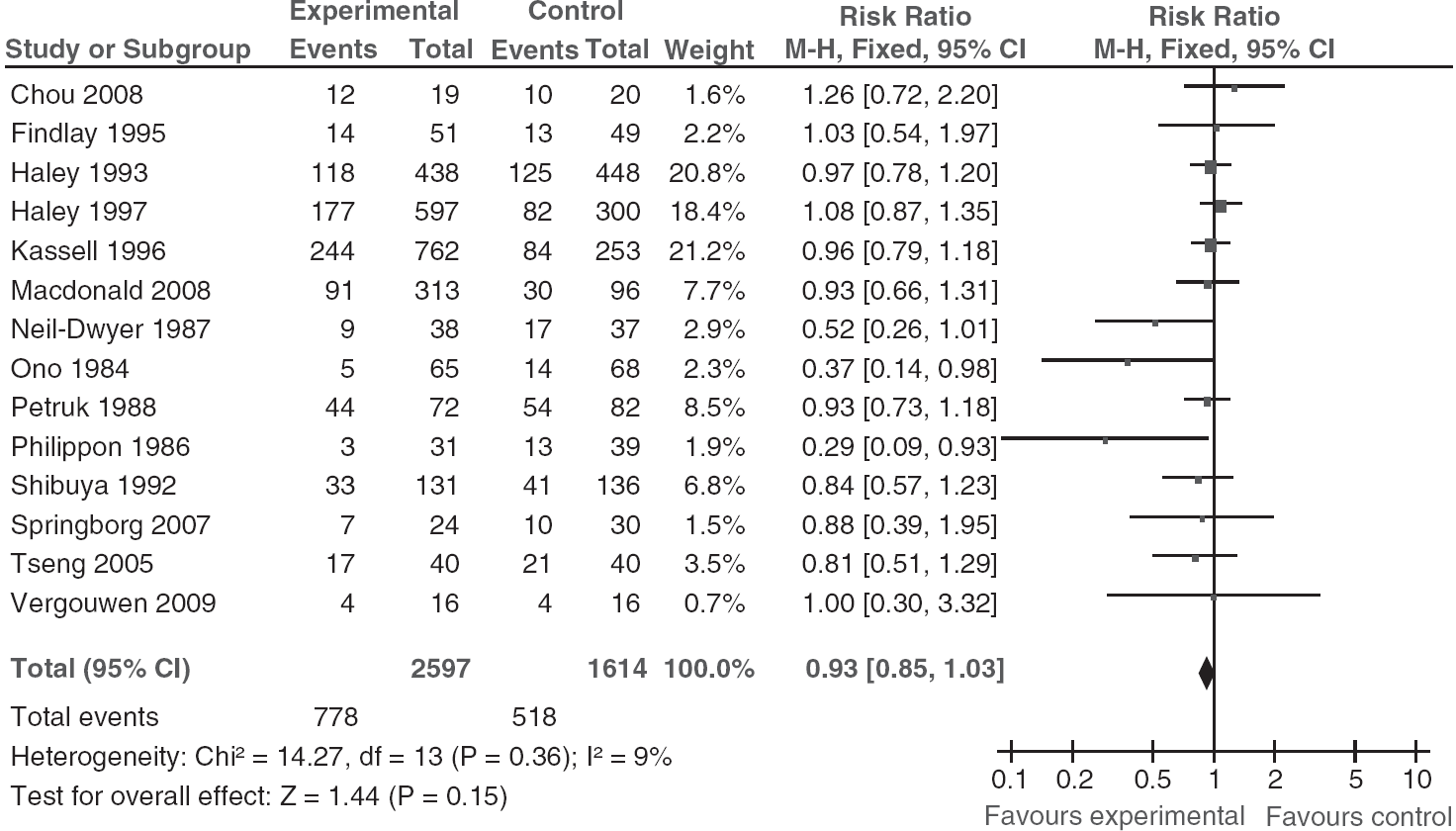
Pooled RR estimates for patients on pharmaceutical treatment found to have poor clinical outcome.
Risk of Bias Assessment
For allocation concealment, risk of bias was low in seven studies (Haley Jr et al, 1993a, b ; Macdonald et al, 2008; Petruk et al, 1988; Shibuya et al, 1992; Springborg et al, 2007; Tseng et al, 2005, 2007; Vergouwen et al, 2009) and unclear in seven studies (Table 1; Chou et al, 2008; Findlay et al, 1995; Haley Jr et al, 1997; Kassell et al, 1996; Neil-Dwyer et al, 1987; Ono et al, 1984; Philippon et al, 1986). For blinding, risk of bias was low in 11 studies (Findlay et al, 1995; Haley Jr et al, 1993a, b , 1997; Kassell et al, 1996; Macdonald et al, 2008; Ono et al, 1984; Petruk et al, 1988; Shibuya et al, 1992; Springborg et al, 2007; Tseng et al, 2005, 2007; Vergouwen et al, 2009) and unclear in 3 studies (Chou et al, 2008; Neil-Dwyer et al, 1987; Philippon et al, 1986). High risk of bias was not observed in any of the studies. The authors of this systematic review acknowledge potential risk of bias, because they are authors of two of the studies included in this systematic review (Macdonald et al, 2008; Vergouwen et al, 2009).
Discussion
This systematic review found that despite a decreased incidence of radiographic vasospasm, pharmaceutical treatment after SAH did not improve clinical outcome. A sensitivity analysis in which only those studies were included that had angiographic vasospasm as an outcome measure, and not TCD vasospasm, did not change our findings. The variety of definitions for clinical deterioration due to DCI did not justify pooling the DCI data.
Previous meta-analyses have questioned the relationship between vasospasm and clinical outcome (Dorhout Mees et al, 2007; Kramer and Fletcher, 2009; Zhang et al, 2010). However, most of these analyses focused on classes of drugs, and therefore the results might be related to pharmacological properties of the type of drug studied. The present systematic review differs from previous studies because we pooled all studies that analyzed the effect of any pharmaceutical intervention, regardless of the type of drug (Weyer et al, 2006). A systematic review that investigated the efficacy of the dihydropyridine calcium antagonist nimodipine showed that nimodipine reduces the incidence of DCI and improves clinical outcome without a statistically significant effect on vasospasm (Feigin et al, 1998). Potential explanations are that, in the nimodipine studies confirmation of vasospasm was not obtained when DCI developed, or that nimodipine exerts its beneficial effect through profibrinolytic properties or conversion of cortical spreading ischemia to cortical spreading hyperemia (Dreier et al, 1998; Vergouwen et al, 2007). Similar to the results of the present study, endothelin receptor antagonists reduced vasospasm and DCI, but not poor clinical outcome (Kramer and Fletcher, 2009). The effect of endothelin receptor antagonists on DCI is not unexpected as the included studies required radiographic confirmation of vasospasm in the diagnosis of DCI (Vergouwen, 2009). Tirilazad mesylate reduced DCI, but not cerebral infarction and poor clinical outcome (Zhang et al, 2010). Statin treatment had no effect on vasospasm, DCI, and clinical outcome (Vergouwen et al, 2010a). However, the statin treatment meta-analysis included only 190 patients, which makes it difficult to draw definitive conclusions about efficacy of statins and their effects on vasospasm, DCI, and clinical outcome.
There are several explanations for the observed dissociation between radiographic vasospasm and clinical outcome in this meta-analysis. First, the pharmaceutical treatments for vasospasm could have detrimental effects that counterbalance any benefits that they might have on clinical outcome (Kramer and Fletcher, 2009). Pulmonary complications, anemia, and hypotension occur more frequently after treatment with endothelin receptor antagonists and nicardipine, and these complications are independently associated with poor outcome (Kahn et al, 2006; Wartenberg et al, 2006). In addition, rescue therapy such as the induction of hypervolemia and hypertension can lead to cardiovascular complications, possibly resulting in worse clinical outcomes. Balloon angioplasty for treatment of vasospasm can lead to complications such as arterial dissection, rupture, stroke, and death. However, if rescue therapy or balloon angioplasty is actually effective, then it could obscure the beneficial effects of drug treatment by being used more in the placebo groups, and one would never show an association between prevention of vasospasm and outcome. Meta-analysis of trials of endothelin receptor antagonists found that these drugs increased side effects such as hypotension and pulmonary edema (Kramer and Fletcher, 2009). Second, sample sizes may be too low to show a statistically significant effect on clinical outcome. It has been estimated that > 5,000 patients are needed to show a treatment effect size of 50% on the mRS at 3 months after SAH, assuming β = 0.80 andα = 0.05 (two-tailed; Kreiter et al, 2009). Third, the dichotomous GOS or mRS may be insensitive to clinically important effects of pharmaceutical treatments on outcome (Al-Khindi et al, 2010; Scott et al, 2010). Deficits in memory, executive function, and language are common cognitive sequelae of SAH and important contributors to poor functional outcome (Al-Khindi et al, 2010; Scott et al, 2010). Deficits in cognitive and functional performance are further complicated by depression, anxiety, fatigue, and sleep disturbances. Nevertheless, these sequelae are often not investigated in SAH studies. Fourth, there may not be a strong causal relationship between vasospasm and functional outcome. There is growing evidence that the pathogenesis of DCI is multifactorial. Microthromboembolism, cortical spreading ischemia, delayed effects of acute SAH-induced brain injury, and impaired cerebral autoregulation have been suggested to have a role in clinical outcome (Dreier et al, 2006; Vergouwen et al, 2008; Yundt et al, 1998).
In the studies that were included in the present systematic review, many different definitions for clinical deterioration due to DCI were used, which did not justify to aggregate and pool the studies in a meta-analysis. Often, included studies combined radiographic evidence of vasospasm with clinical features of cerebral ischemia, while multiple factors might contribute to DCI. Recently, a uniform definition of DCI has been proposed with the aim to standardize end points for clinical trials, simplify comparisons between studies, and aggregate study results in meta-analyses (Vergouwen et al, 2010b).
This study has some limitations. Angiography often was only performed in selected patients, a practice that would decrease the correlations among vasospasm, DCI, and clinical outcome. The definition and grading of radiographic vasospasm varied throughout the studies, and TCD as a diagnostic tool to measure vasospasm might add inaccuracy (Carrera et al, 2009). However, a sensitivity analysis that included studies with angiographic vasospasm only did not change the results. Finally, clinical outcome was measured with various scales and cutoffs for poor clinical outcome, and the timing of follow-up measurements differed among the included studies. However, these factors will have minimal effect because the GOS and mRS give almost identical results in patients with SAH (Macdonald et al, 2008). The timing of outcome assessment only matters if there is a change in the rates of recovery in the treated and untreated groups, which seems unlikely given that the treatments being applied are in the acute stage.
In conclusion, pharmaceutical treatments may decrease radiographic vasospasm in patients with SAH, but there is no effect on the clinical outcome. Future studies need to determine whether this dissociation between vasospasm and clinical outcome is due to methodological problems, sample size, insensitivity of clinical outcome measures, the effect of therapeutic strategies such as endovascular therapy, or because of mechanisms other than vasospasm also contributing to poor clinical outcome.
Footnotes
Nima Etminan is financially supported by an unrestricted grant from the Wilhem-Tönnis Foundation, Germany. Mervyn DI Vergouwen is financially supported by an unrestricted grant from the Niels Stensen Foundation, The Netherlands, and by a grant from the Netherlands Thrombosis Foundation (2010-4). Nima Etminan and RL Macdonald received research support from the Physicians Services Incorporated Foundation. Dr RL Macdonald is a consultant for Actelion Pharmaceuticals and Chief Scientific Officer of Edge Therapeutics.