
Abstract
Cerebral vasospasm and late cerebral ischemia (LCI) remain leading causes of mortality in patients experiencing a subarachnoid hemorrhage (SAH). This occurs typically 3 to 4 days after the initial bleeding and peaks at 5 to 7 days. The underlying pathophysiology is still poorly understood. Because SAH is associated with elevated levels of endothelin-1 (ET-1), focus has been on counteracting endothelin receptor activation with receptor antagonists like clazosentan, however, with poor outcome in clinical trials. We hypothesize that inhibition of intracellular transcription signaling will be an effective approach to prevent LCI. Here, we compare the effects of clazosentan versus the MEK1/2 blocker U0126 in a rat model of SAH. Although clazosentan directly inhibits the contractile responses
Introduction
Aneurysmal subarachnoid hemorrhage (SAH) is the cause of 7% of all strokes and carries high mortality and morbidity because of rebleeding and late cerebral ischemia (LCI). 1 Angiographic vasospasm can be seen in up to 70% of SAH patients, and is typically found between 5 to 14 days after onset of SAH. However, symptomatic vasospasm is only seen in 30% of patients, whereas LCI occurs in ∼50% of patients with angiographic vasospasm. 2 Treatment of patients have improved because of developments in neurointensive care but specific drug treatments have only achieved modest results.3, 4 In recent years, much effort has been directed to the study of endothelin antagonists in patients with SAH. Four trials using clazosentan and one trial with TAK-044 (both combined ETA and ETB receptor blockers)5, 6 have been carried out. These studies show that endothelin has an important role in the genesis of angiographic vasospasm but the benefit is less on LCI and nonexistent on the overall clinical outcome. Why the drugs reduce vasospasm but fail to improve LCI and outcome is still unclear. 7
We have observed that immediately after SAH there is an early activation of intracellular signaling in cerebrovascular smooth muscle cells, which results in increased expression of a panel of G-protein-coupled receptors mediating constriction and of cytokines, iNOS and MMP-9.8, 9 This occurs via the Ras—Raf—MEK—ERK1/2 pathway and can be blunted with early inhibition of this intracellular pathway. 10 The early SAH-induced activation of the MEK—ERK1/2 pathway depends on the initial rise in intracranial pressure and the accompanying reduction in cerebral blood flow (CBF).11, 12 Thus, although receptor antagonists like clazosentan block specific contractile receptor subtypes directly,13, 14 MEK1/2 inhibition inhibits the transcriptional upregulation of several different vasoconstrictor receptor types. 10
We hypothesize that inhibition of signaling pathways that control upregulation of the entire panel of contractile receptors after SAH will provide a better approach toward improving outcome after SAH than blocking endothelin receptors specifically. The aim of this study was, therefore, to directly compare these two different approaches to treatment in a SAH rat model on mechanisms putatively involved in LCI and on neurologic outcome. We report that endothelin receptor inhibition with clazosentan
Materials and methods
Rat Subarachnoid Hemorrhage Model
All experiments and procedures were performed in full compliance with the guidelines set forth in the European Council's Convention for the Protection of Vertebrate Animals Used for Experimental and other Scientific Purposes, and were approved by the Danish National Ethics Committee (Danish Animal Experimentation Inspectorate license no. 2011/561–2025).
SAH was induced as described in detail before. 15 Male Sprague—Dawley rats (11 to 12 weeks old, 300 g) were anesthetized using 3.5% Isoflurane (Abbott Laboratories, Green Oaks, IL, USA) in atmospheric air/O2 (70%:30%). Rats were orally intubated and artificially ventilated with inhalation of 1% to 2% Isoflurane in N2O/O2 (70%:30%) during surgery. Blood samples were regularly analyzed in a blood gas analyzer (Radiometer AS, Copenhagen, Denmark). Body temperature was kept at 37 °C±0.5 °C with a regulated heating pad. Mean arterial blood pressure (MABP) and intracranial pressure (ICP) were continuously measured via catheters inserted into the tail artery and the cisterna magna, respectively, connected to pressure transducers and a PowerLab and recorded by the LabChart software (all from AD Instruments, Oxford, UK). A laser-Doppler blood flow meter probe was placed on the dura through a hole in the skull drilled 4 mm anterior from the bregma and 3 mm rightwards of the midline. Through a second hole drilled 6.5 mm anterior to the bregma in the midline, a 27 G blunt canula was descended stereotactically at an angle of 30° to the vertical plane toward a final position of the tip immediately anterior to the chiasma opticum. After 30 minutes of equilibration, 250 μL of blood was withdrawn from the tail catheter and injected manually through the canula. The pressure of the blood injections was carefully controlled (manually) aiming at raising ICP to mean arterial blood pressure levels. Subsequently, rats were maintained under anesthesia for another 60 minutes while continuing ICP and CBF recordings. At the end of the procedure, the ICP catheter was cut and sealed 0.5 cm from the tip. However, in rats to be treated with U0126, clazosentan, or vehicle, the ICP catheter was cut 2 cm from the tip and closed with a removable plug to be used for later treatment administration. The tail catheter, needle, and laser-Doppler probe were removed and incisions closed. Rats were revitalized and extubated. At the end of surgery and every 24 hours thereafter, rats received subcutaneous injections of Carprofen (4 mg/kg; Pfizer, Copenhagen, Denmark) and 15 mL isotonic saline.
Sham-operated rats went through the same procedure with the exception that no blood was injected intracisternally. We did not perform intracisternal saline injections in the sham animals, which if performed would have induced a pronounced acute increase in ICP in the sham animals similar to the ICP rise induced by intracisternal blood injection in the SAH animals. This choice of sham procedure was motivated by two earlier studies in which we carefully evaluated the importance of the acute rise in ICP during the induction of SAH for the process of vasoconstrictor receptor upregulation.11, 12 These studies demonstrated that both the acute ICP rise and the presence of subarachnoid blood contributes to initiating the process of vasoconstrictor receptor upregulation, and, therefore, sham animals receiving intracisternal saline injections would not serve as an appropriate control situation.
U0126 treatment
Animals in the U0126 treatment group were treated with 0.05 mL/kg body weight of a 10−5 M solution of U0126 ethanolate (Sigma-Aldrich, St Louis, MO, USA; yielding a final dose of 0.37 μg/kg body weight) diluted in isotonic saline plus 0.1% dimethyl sulfoxide. Animals in the vehicle group were treated with 0.05 mL/kg body weight isotonic saline plus 0.1% dimethyl sulfoxide. Treatment was administered at 6, 12, and 24 hours post SAH intracisternally through the ICP catheter in the cisterna magna. Animals were then left untreated until termination at 72 hours post SAH.
Clazosentan treatment
Animals in the clazosentan treatment group were treated with 0.05 mL/kg body weight of a 10−5 M solution of clazosentan (RO 61–1790, Actelion, Allschwill, Switzerland; yielding a final dose of 0.38 μg/kg body weight) diluted in isotonic saline plus 0.1% dimethyl sulfoxide. This dose was chosen with the aim of obtaining a concentration of 10−7 M in cerebrospinal fluid, at which the drug has been shown to specifically inhibit the ETA receptor in cerebral arteries
Neurologic Function
All neurologic tests were performed by personnel masked with regard to experimental groups of the animals. Tests and observations were done in the morning to minimize diurnal rhythm variation.
Spontaneous activity
Spontaneous activity of the rats was quantified by placing the rats individually in a test cage with fresh bedding and nesting material for 20 minutes. All intervals spent moving around in the cage (locomotion), sitting, or lying in the same place (no movement), rearing, grooming, or eating were recorded by an observer with a timer.
Rotating pole test
Gross sensorimotor function was evaluated as the ability of the animals to balance and to coordinate their movements when traversing a horizontal pole, which can be either steady or rotating (3 r.p.m.). 16 In one end of the pole (45 mm in diameter and 150 cm in length), a cage with bedding material from the home cage of the rat being tested and with an entrance hole facing the pole was placed. Performance of the rats was scored according to the following definitions: score 1, unable to balance on the pole and falls off immediately; score 2, balances on the pole but has severe difficulty crossing the pole and moves <30 cm; score 3, embraces the pole with paws and does not reach the end of the pole but does manage to move >30 cm; score 4, traverses the pole but embraces the pole with paws and/or jumps with hind legs; score 5, traverses the pole with normal posture but with >3 foot slips; score 6, traverses the pole perfectly with <3 foot slips. On the day before surgery, all animals were trained until they obtained a score of 5 to 6. On each day after SAH, animals were tested twice on the static pole, once with rotation to the left and once with rotation to the right.
[14C] Iodoantipyrine Method for Measurement of Cerebral Blood Flow
Global cortical CBF was measured by the [14C] iodoantipyrine method originally described for autoradiographic measurements of CBF 17 and later modified for direct scintillation on brain tissue. 18 In brief, rats were anesthetized with 3.5% Isoflurane in atmospheric air/O2 (70%:30%), intubated, and kept artificially ventilated and anesthetized with 1% to 2% Isoflurane in N2O/O2 (70%:30%). Respiration was regulated according to regular analyses of blood gases, and body temperature was kept at 37 °C±0.5 °C with a regulated heating pad. Mean arterial blood pressure was continuously measured via a femoral artery catheter, and a catheter for heparin injection and 14C-iodoantipyrine 4[N-methyl-14C] infusion was inserted into a femoral vein. After 30 minutes of equilibration, a bolus injection of 20 μCi 14C-iodoantipyrine 4[N-methyl-14C] (Perkin-Elmer, Boston, MA, USA) in saline was given (intravenously). At the start of the isotope injection and for the following 24 seconds, one drop of arterial blood was sampled every 2 seconds. At 24 seconds after isotope injection, rats were decapitated and the brains removed. Cerebellum and brain stem were removed and the cortex from both hemispheres was cleared of subcortical white matter and meninges with associated larger vessels. Within 1 minute after decapitation, the cortex tissue was cut into smaller pieces, transferred to scintillation vials, and weighed. Tissue samples weighed 100±12 mg. Samples were dissolved in 1 mL BTS-450 (Beckman Coulter, Fullerton, CA, USA) for every 100 mg tissue, and digested at 60 °C for 3 hours. Samples were then decolorized with 0.4 mL 30% H2O2 for 1 hour and chemiluminiscence was eliminated by the addition of 70 μL glacial acetic acid to each sample. After the addition of 10 mL Ready Organic scintillation liquid (Beckman Coulter), vials were counted in a Beckman Liquid Scintillation Counter (Beckman Coulter).
Arterial blood samples were transferred to scintillation vials containing 1 mL of a 1:1 mixture of Soluene-350 (Perkin-Elmer, Waltham, MA, USA) and isopropanol, and dissolved for 2 hours at 60 °C. Samples were decolorized with 0.2 mL 30% H2O2 for 30 minutes at room temperature and then heated to 60 °C for 30 minutes. Ten milliters of Ready Organic scintillation liquid was added and vials were counted as above. Cerebral blood flow was calculated by solving the equation. 18

for
Laser-Doppler Flowmetry for Measurement of Acute Cerebrovascular ET Receptor Antagonism by Clazosentan In Vivo
A catheter was inserted into the cisterna magna and a laser-Doppler blood flow meter probe was placed on the dura through a hole in the skull drilled 4 mm anterior from the bregma and 3 mm rightwards of the midline. 19 Clazosentan or vehicle was injected into the cisterna magna catheter followed after 1 hour by injection of two increasing doses of ET-1, also in the cisterna magna catheter. Cerebral blood flow was continuously monitored from 1 hour after injection of clazosentan until 30 minutes after the injection of ET-1.
Harvest of Cerebral Arteries
Rats were decapitated 2, 3, or 4 days after SAH or sham surgery (during CO2 sedation). Brains were removed and chilled in cold bicarbonate buffer solution before the isolation of middle cerebral arteries (MCAs).
In Vitro Pharmacology
A wire myograph (Danish Myograph Technology A/S, Aarhus, Denmark) was used to record isometric tension in segments of isolated cerebral arteries.
20
One millimeter long vessel segments were mounted in the myograph and immersed in a 37 °C running buffer solution of the following composition (mmol/L): NaCl 119, NaHCO3 15, KCl 4.6, MgCl2 1.2, NaH2PO4 1.2, CaCl2 1.5, and glucose 5.5. The buffer was continuously aerated with 5% CO2 maintaining a pH of 7.4. The vessel segments were stretched to pretension of 2 mN/mm and allowed to equilibrate. The vessels were then exposed to a solution of 63.5 mmol/L K+ obtained by the partial substitution of NaCl for KCl in the above described buffer. Basilar artery (BA) with K+-induced responses over 2 mN and MCA with K+-induced responses over 0.7 mN were used for experiments. Concentration-response curves were obtained by cumulative application of 5-CT (5-carboxamidotryptamine; Sigma, St Louis, MO, USA) in the concentration range 10−12 to 10−4 M and ET-1 (AnaSpec, San Jose, CA, USA) in the concentration range 10−14 to 10−7 M. The presence of functional endothelium in the vessel segments was assessed by means of precontraction with 5-HT (3 × 10−7 M) followed by relaxation with carbachol (10−5 M) as described in Larsen
Immunohistochemistry
Four millimeter long MCA segments were imbedded in Tissue-Tek (Gibco, Invitrogen A/S, Taastrup, Denmark) and frozen on dry ice. Ten micrometer thick sections were prepared in a cryostat (Leica Microsystems GmbH, Wetzlar, Germany). After fixation in Stephanini's fixative, the sections were pre-incubated with phosphate-buffered saline containing 5% donkey serum (Jackson ImmunoResearch Europe, West Grove, PA, USA) and 1% bovine serum albumin (BSA). The primary antibodies used were sheep anti-ETB (Alexis Biochemicals, Farmingdale, NY, USA) diluted 1:250, rabbit anti-5-HT1B (Abcam, Cambridge, UK) diluted 1:200 and mouse anti-β-actin (Abcam) diluted 1:500. Secondary antibodies used were DyLight 488-conjugated donkey anti-sheep antibody diluted 1:200, DyLight 488-conjugated donkey anti-rabbit antibody 1:200 and DyLight 549-conjugated donkey anti-mouse antibody 1:200 (all from Jackson ImmunoResearch Europe). All antibodies were diluted in phosphate-buffered saline containing 1% BSA, 0.25% Triton X-100 and in addition, primary antibody dilution buffer contained 2% donkey serum. On negative control slides, primary antibodies were omitted. Secondary antibodies were detected at appropriate laser wavelengths in a confocal microscope (Nikon D-eclipse C1, Nikon Instruments, Tokyo, Japan). Images were analyzed using the software EZ-C1 3.70 FreeViewer, measuring the staining intensity in the smooth muscle cell (β-actin positive) layer. The β-actin positive layer was marked manually, and the staining intensity was quantified in the entire β-actin positive area. All images were analyzed by personnel masked with regard to the experimental groups of the animals. 10 To minimize complications of the quantification because of differences in the extent of fixation, antibody penetration, etc., only sections showing strong beta-actin staining in the entire smooth muscle layer, as well as normal morphology of the tissue were used for quantification of receptor staining intensity. Moreover, to minimize the technical/methodological variation, intensities from three sections from each animal were averaged.
Western Blotting
The BA and both MCAs were isolated from the brains of sham-operated, SAH-induced, SAH-induced treated with U0126, and SAH-induced treated with clazosentan rats at 3 days after SAH induction or sham operation and all the three arteries were pooled into one sample for each rat. The arteries were homogenized by sonication on ice for 2 minutes in a modified RIPA buffer (50 mmol/L Tris pH 7.5, 150 mmol/L NaCl, 1 mmol/L EDTA, 50 mmol/L beta-glycerolphosphate, 1% NP-40, 0.1% deoxycholate, 0.1% SDS, 0.5% Triton X-100) containing phosphatase (Merck, Darmstadt, Germany) and protease inhibitor (Sigma, St Louis, MI, USA) cocktails. Sonicated tissue lysates were centrifuged at 15.000 at 4 °C for 15 minutes, and the supernatants were collected as protein samples. Protein concentrations were determined using standard protein assay reagents (Bio-Rad, Hercules, CA, USA) and 15 to 20 μg total protein in each sample was added LDS sample buffer (Expedeon, Cambridgeshire, UK) and separated on a 4% to 12% RunBlue SDS Precast gel (Expedeon) at 180 V for 60 minutes and then transferred to a PVDF membrane at 150 V for 70 minutes. Membranes were blocked in blocking buffer (phosphate-buffered saline containing 0.1% Tween-20 and 2% ECL Advance blocking agent (GE Healthcare, Buckinghamshire, UK)) for 1 hour at room temperature and then incubated overnight rotating at 4 °C in blocking buffer with the primary antibody rabbit anti-ETB receptor (Alomone Labs, Jerusalem, Israel) followed by incubation with ECL horse-radish peroxidase-conjugated sheep anti-rabbit IgG antibody (GE Healthcare) for 1 hour at room temperature. 21 Labeled proteins were developed using Lumigen TMA-6 chemiluminiscence solutions (Pierce/Thermo Scientific, Rockford, IL, USA). Subsequently, membranes were extensively washed in phosphate-buffered saline plus 0.1% Tween-20 and then reprobed with the primary antibody goat anti-rat 5-HT1B receptor (Abcam) at 4 °C overnight in blocking buffer followed by incubation with horse-radish peroxidase-conjugated rabbit anti-goat IgG antibody (Pierce/Thermo Scientific) for 1 hour at room temperature and development of labeled proteins. Finally, blots were reprobed with mouse beta-actin antibody (Abcam) for loading control at +4 °C overnight in blocking buffer followed by incubation with horse-radish peroxidise-conjugated rabbit anti-mouse IgG antibody (Pierce/Thermo Scientific) for 1 hour at room temperature and development of labeled proteins. Labeling chemiluminiscence intensities were quantified using the software Image Gauge V4.0 (Fujifilm, Tokyo, Japan).
Statistical Methods
Concentration-contraction curves were compared by two-way analysis of variance. Immunohistochemistry and western blot data were analyzed with one-way analysis of variance followed by Bonferroni's
Results
The Subarachnoid Hemorrhage Method
In all rats, mean arterial blood pressure, PaO2, PaCO2, pH, and temperature were within acceptable physiologic limits during surgery, and there were no differences in physiologic parameters between the groups (Supplementary Table 1).12, 21 Injection of blood prechiasmatically increased ICP from 8 to 168 mm Hg and cortical CBF dropped to 13% of resting flow (group average of all SAH animals). There was no difference between the three treatment groups.
The acute mortality rate during the first 24 hours after surgery was 9% for all SAH animals and 3% for all sham-operated animals. There was no difference in mortality between the three groups (vehicle, U0126, and clazosentan treatment groups) during the first 24 hours.
Time Course of Upregulation of Contractile ETB and 5-HT1B Receptors in Cerebral Arteries after Subarachnoid Hemorrhage
Figure 1 shows that the 5-CT-induced concentration-response curve was shifted to the left in SAH at 2 and 3 days post SAH but not at day 4 post SAH. The responses in the basilar and MCAs from sham-operated rats did not differ from fresh (from unoperated rats) vessels (data not shown). The ET-1 responses increased significantly in maximum contraction at day 2 and 3 post SAH. As demonstrated in an earlier study, the apparent normalization of the contractile responses at day 4 post SAH may be the large mortality after day 3, after which only less affected animals survive. 12
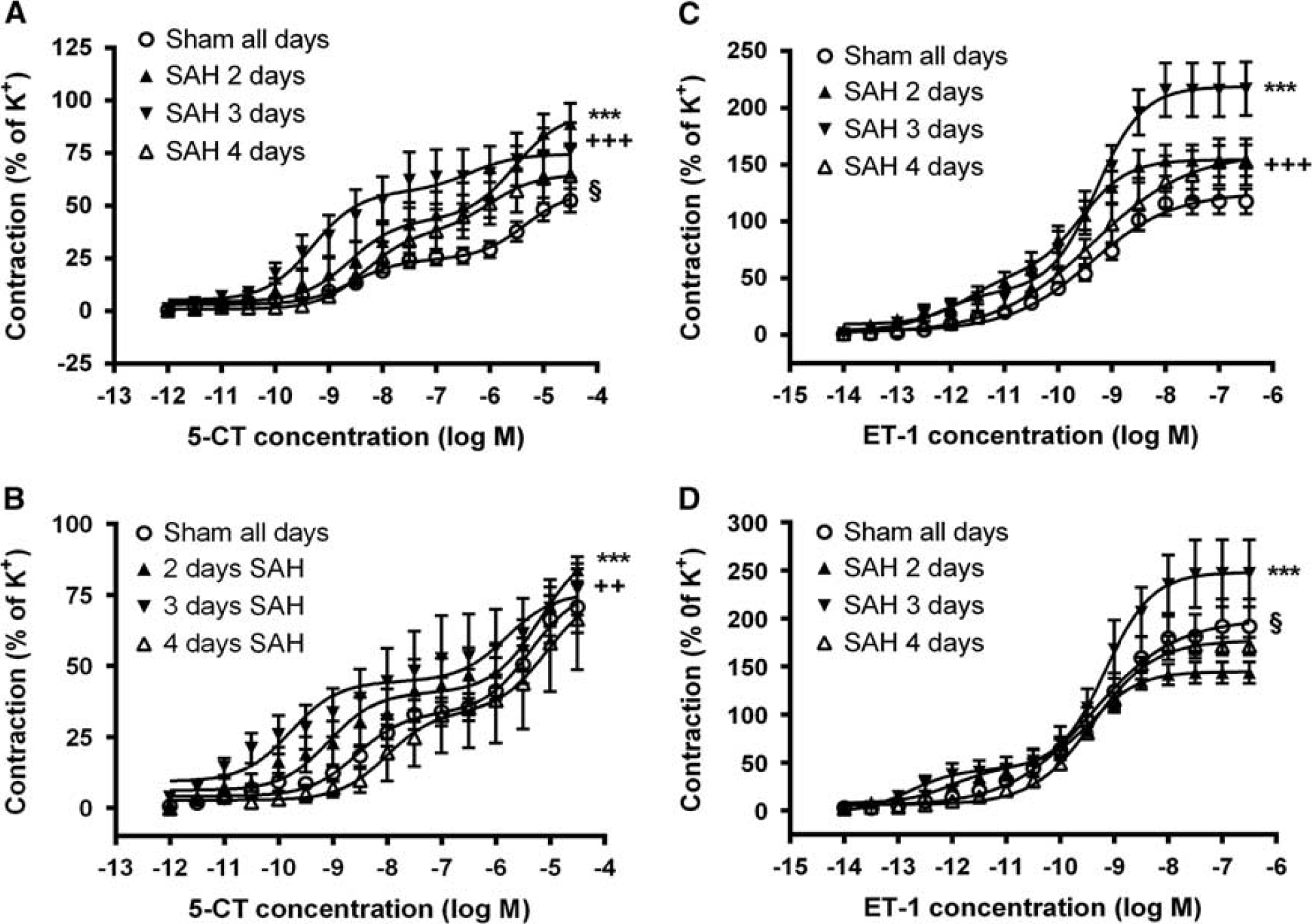
Concentration-response curves elicited by 5-CT and ET-1 in cerebral arteries in various time points after SAH. Shown are the data for BA and MCA from sham-operated rats terminated at either 2, 3, or 4 days after sham operation (Sham all days) and rats with induced experimental SAH terminated at 2, 3, or 4 days after the SAH (SAH 2 days, SAH 3 days, SAH 4 days). (
These enhanced contractile responses were in agreement with protein analysis demonstrating that the immunoreactivity of 5-HT1B and ETB receptors showed enhanced expression in the vascular smooth muscle cells at day 2 and 3 after the SAH (Figures 2 and 3). The upregulation of these receptors was also verified by western blotting at day 3 post SAH (Figure 6).
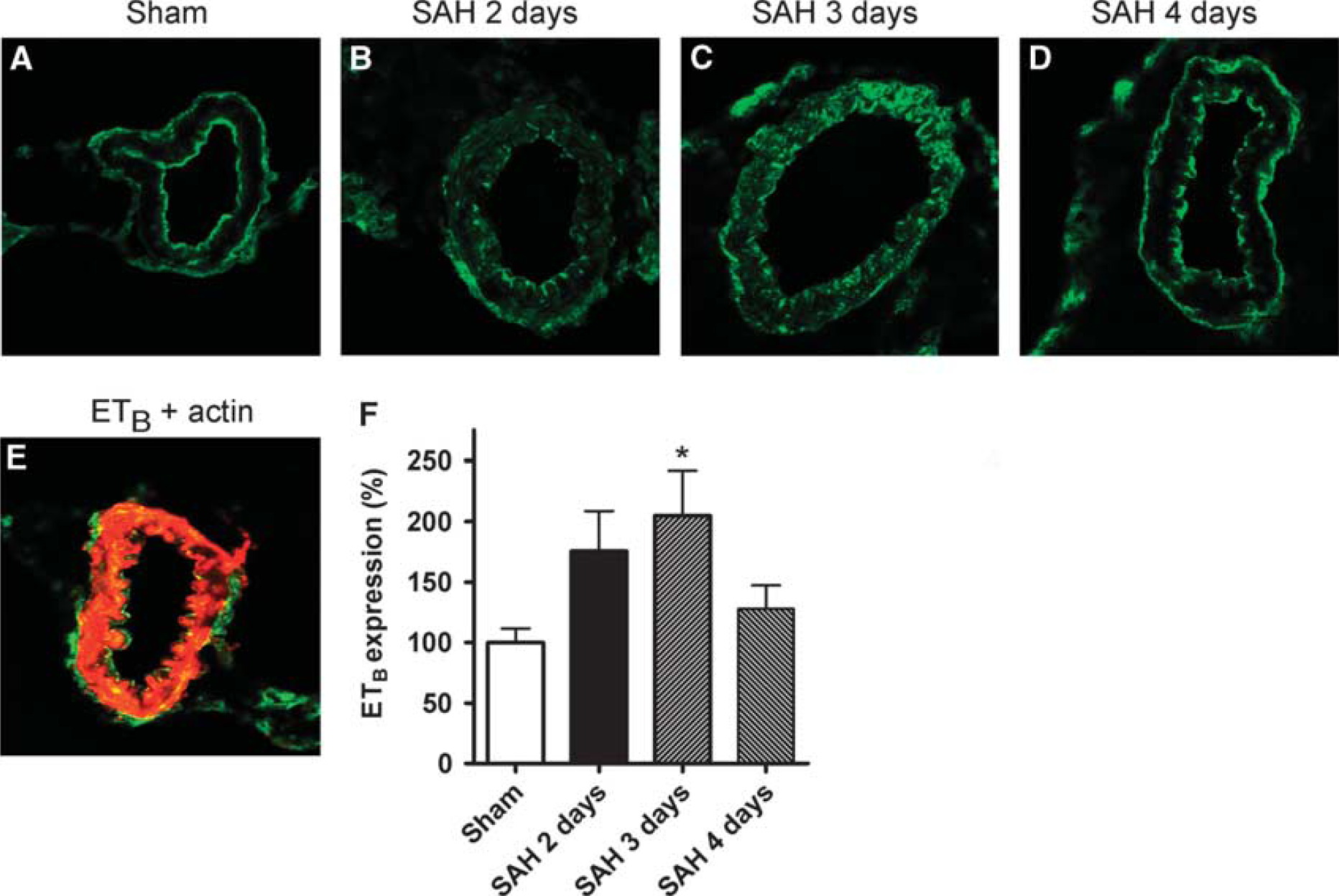
Time-course of ETB receptor expression in cerebral arteries. ETB receptor expression and localization was determined in MCA sections by means of immunohistochemical stainings and confocal microscopy. Shown are data for sham-operated rats (sham) and rats with induced experimental SAH terminated at 2, 3, or 4 days after the SAH (SAH 2 days, SAH 3 days, SAH 4 days). (
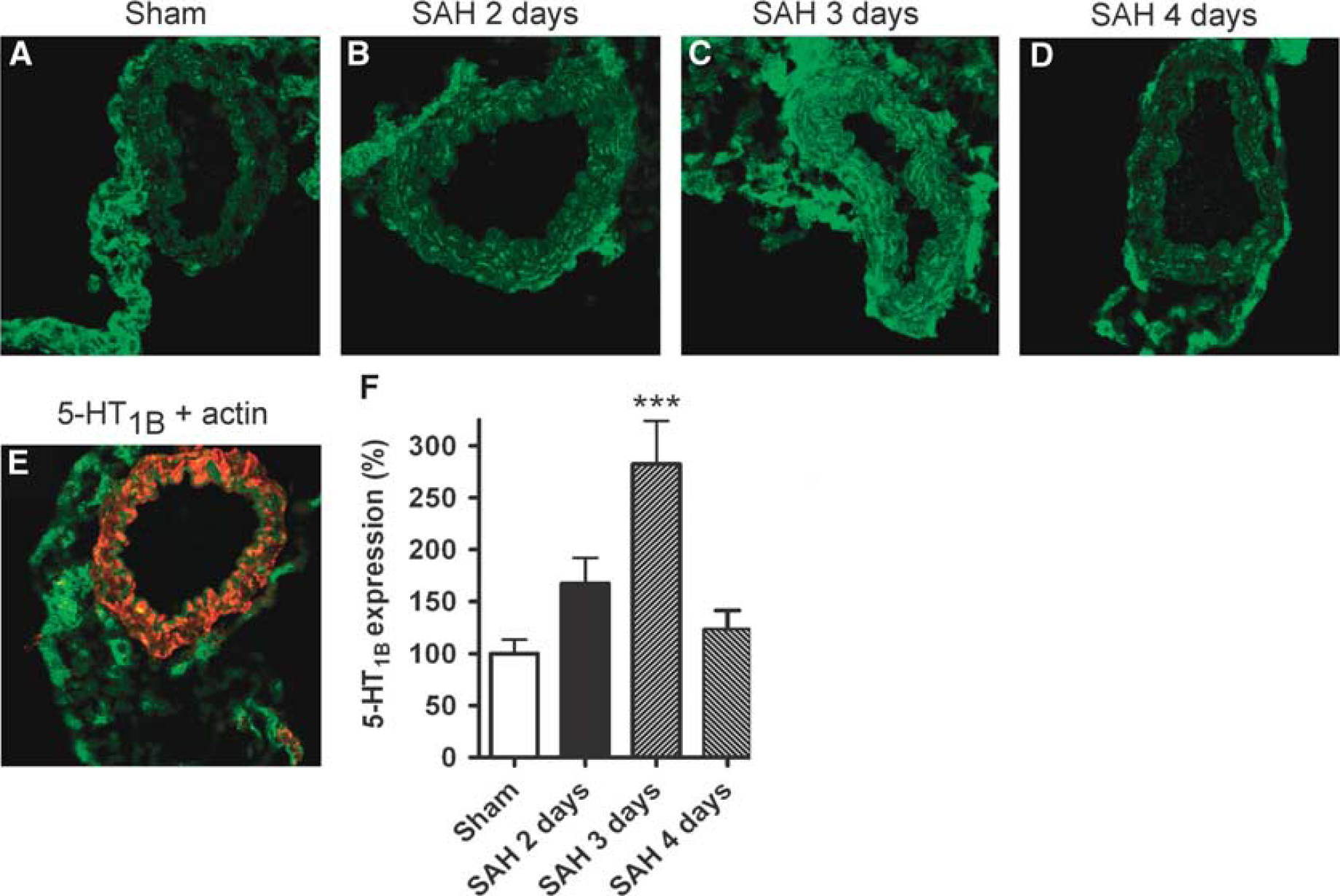
Time-course of 5-HT1B receptor expression in cerebral arteries. 5-HT1B receptor expression and localization was determined in MCA sections by means of immunohistochemical stainings and confocal microscopy. Shown are data for sham-operated rats (Sham) and rats with induced experimental SAH terminated at 2, 3, or 4 days after the SAH (SAH 2 days, SAH 3 days, SAH 4 days) (
Quantitative measurements of CBF with an injection of [14C] iodoantipyrine showed marked reductions at day 2 and 3 but not significant at day 4 (Figure 4), thus correlating with the time course of contractile receptor upregulation. Moreover, neurology scores after SAH was analyzed using spontaneous activity analysis (locomotion, rearing, and time with no movement) and the rotating pole test. 8 As can be seen in Figure 4, the SAH resulted in significantly reduced neurologic function with a time course correlating with receptor upregulation and CBF reduction.
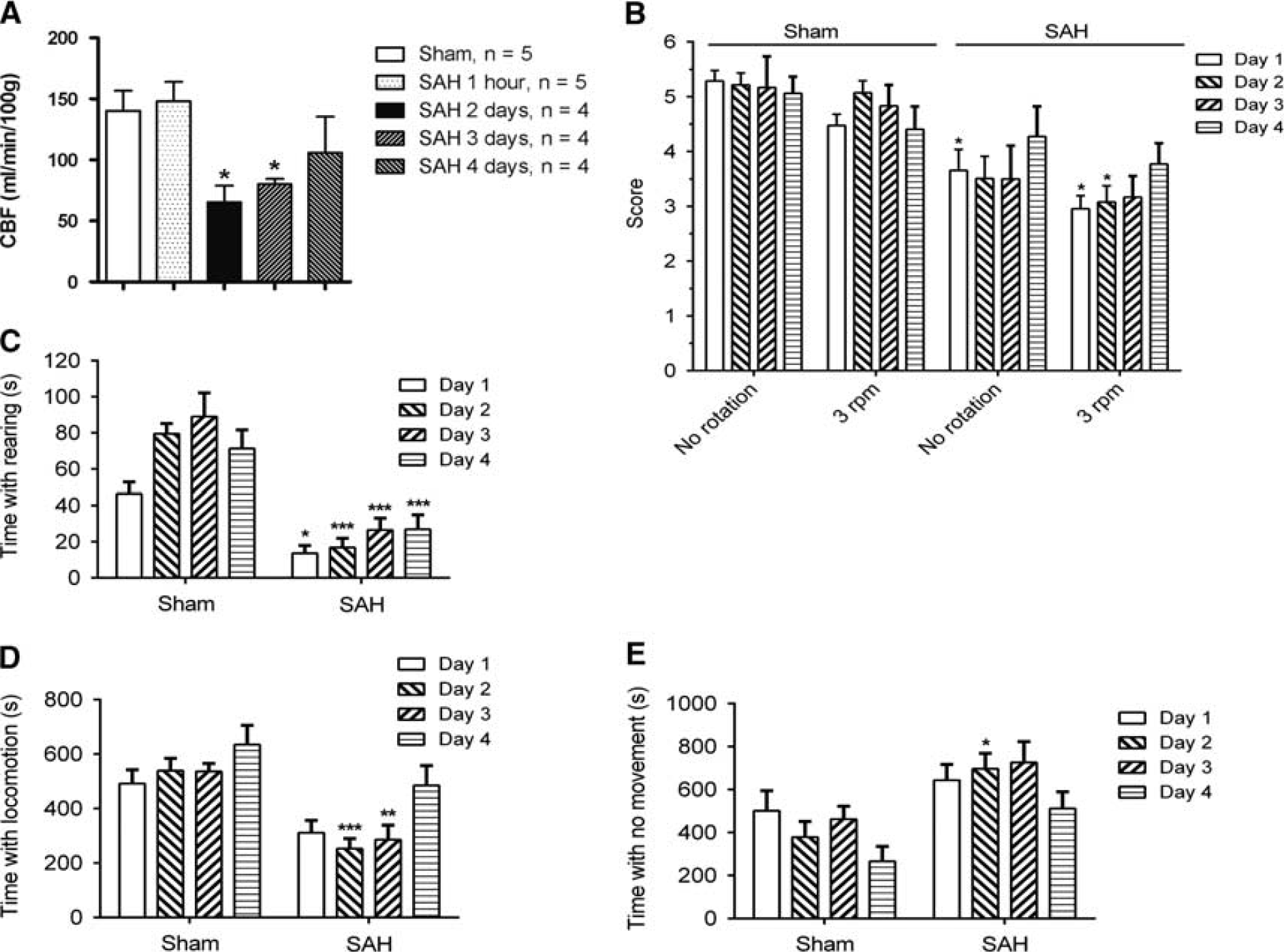
Cerebral blood flow (CBF) and neurologic deficits at various time points after SAH. (
Effect of U0126 and Clazosentan on ETB and 5-HT1B Receptor Contractile Function after Subarachnoid Hemorrhage
At first, we verified that the chosen dose of clazosentan was active in cerebral arteries when given intracisternally. CBF was measured by laser-Doppler flowmetry via a closed cranial window. Animals were treated with clazosentan or vehicle injected into cisterna magna via a catheter 1 hour before start of the CBF measurement. ET-1 (50 μL of a 10−7 M or a 10−6 M solution as indicated in Figure 5) was likewise injected into the cisterna magna catheter. Clazosentan blocked the acute effect of ET-1. Previously, we have demonstrated that U0126 MEK1/2 inhibition 8 or Raf inhibition 22 has no effect on CBF in itself. In this study, we confirmed that U0126 did not block the acute contractile response to ET-1 on cerebral vessels (data not shown).
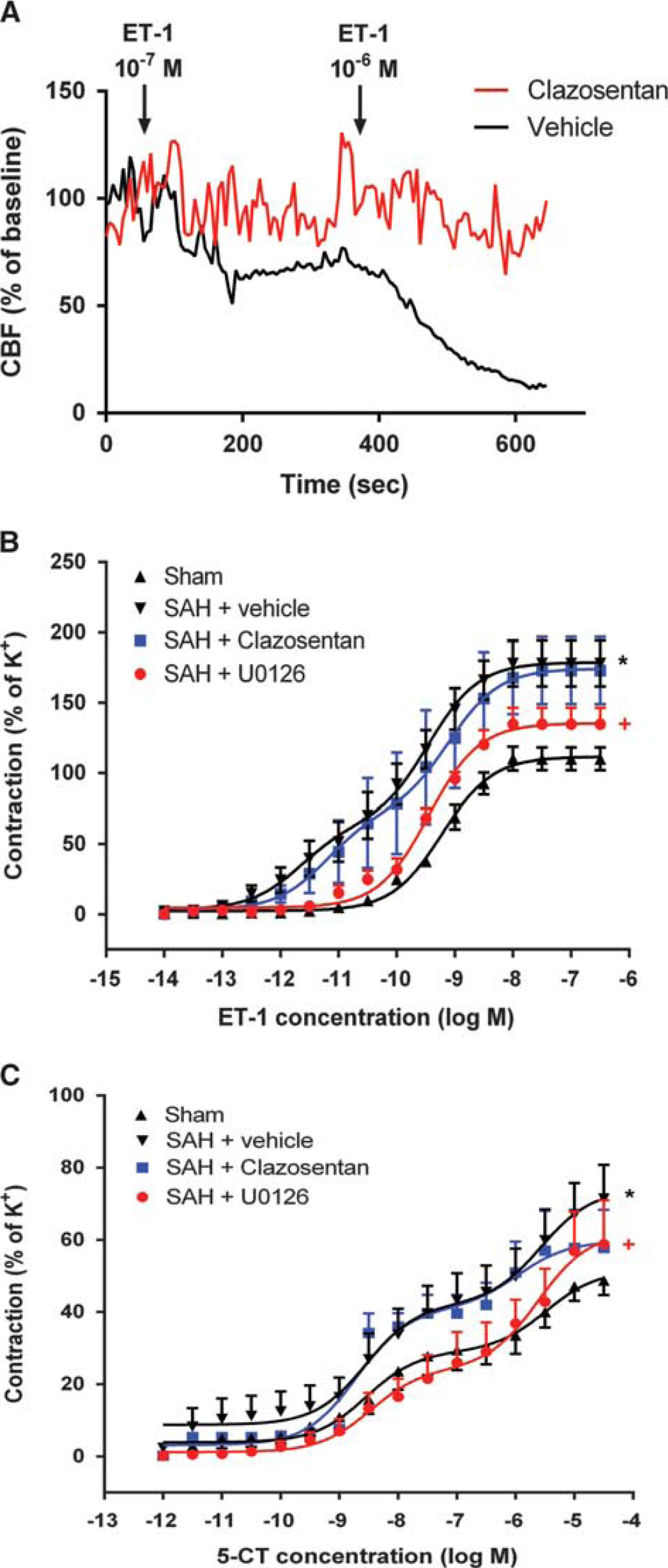
Effect of clazosentan and U0126 on SAH-induced enhancement of contractile responses to ET-1 and 5-CT. (
We subsequently tested the effect of treatment with either U0126 or clazosentan started 6 hours after the SAH on the subacute enhancement of contractile responses to ET-1 and 5-CT at day 3 post SAH. Although the U0126 treatment completely prevented receptor upregulation, treatment with clazosentan had no effect on the enhanced contractility (Figure 5).
Effect of U0126 and Clazosentan on ETB and 5-HT1B Receptor Protein Expression after Subarachnoid Hemorrhage
To confirm the effect of the two different treatment approaches on post-SAH upregulation of contractile receptors, we assessed the expression levels of ETB and 5-HT1B receptors at 3 days post SAH in the treatment groups. SAH-induced enhanced protein levels for these two receptors and this response was significantly blunted by U0126 but not by clazosentan treatment (Figure 6).
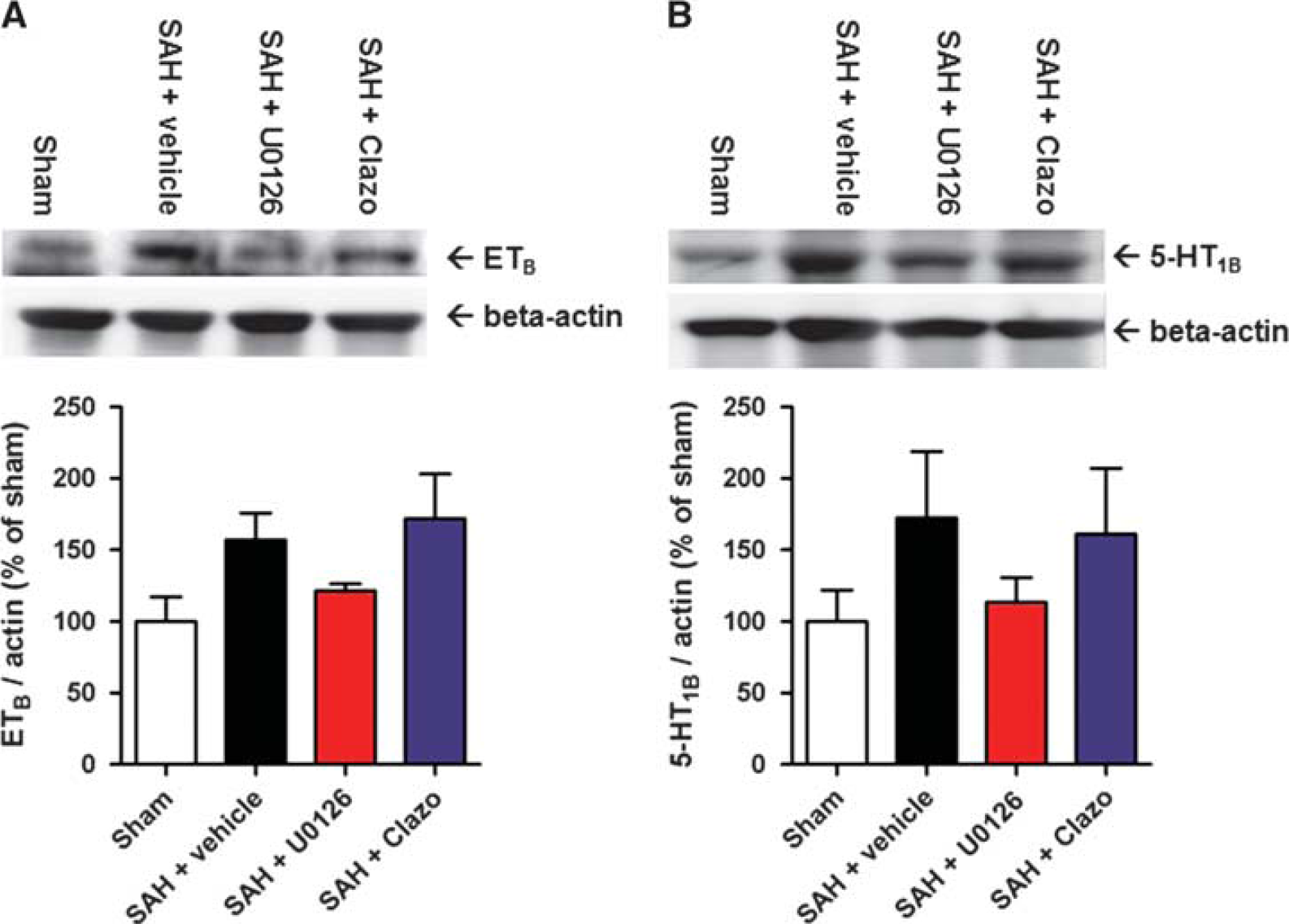
Effect of clazosentan and U0126 on SAH-induced upregulation of ETB and 5-HT1B receptor protein levels. Immunoblots of ETB (
Effect of U0126 and Clazosentan on Neurologic Function after Subarachnoid Hemorrhage
Neurologic outcome was evaluated using the rotating pole method (Figure 7). In sham animals, the behavior score was above and around 5, which is normal. At day 1, it was depressed in all three SAH groups; but at day 2 and 3, the U0126-treated animal score did not differ from sham (around score 5), whereas the clazosentan and vehicle groups were still significantly impaired (scores ∼3 to 5).
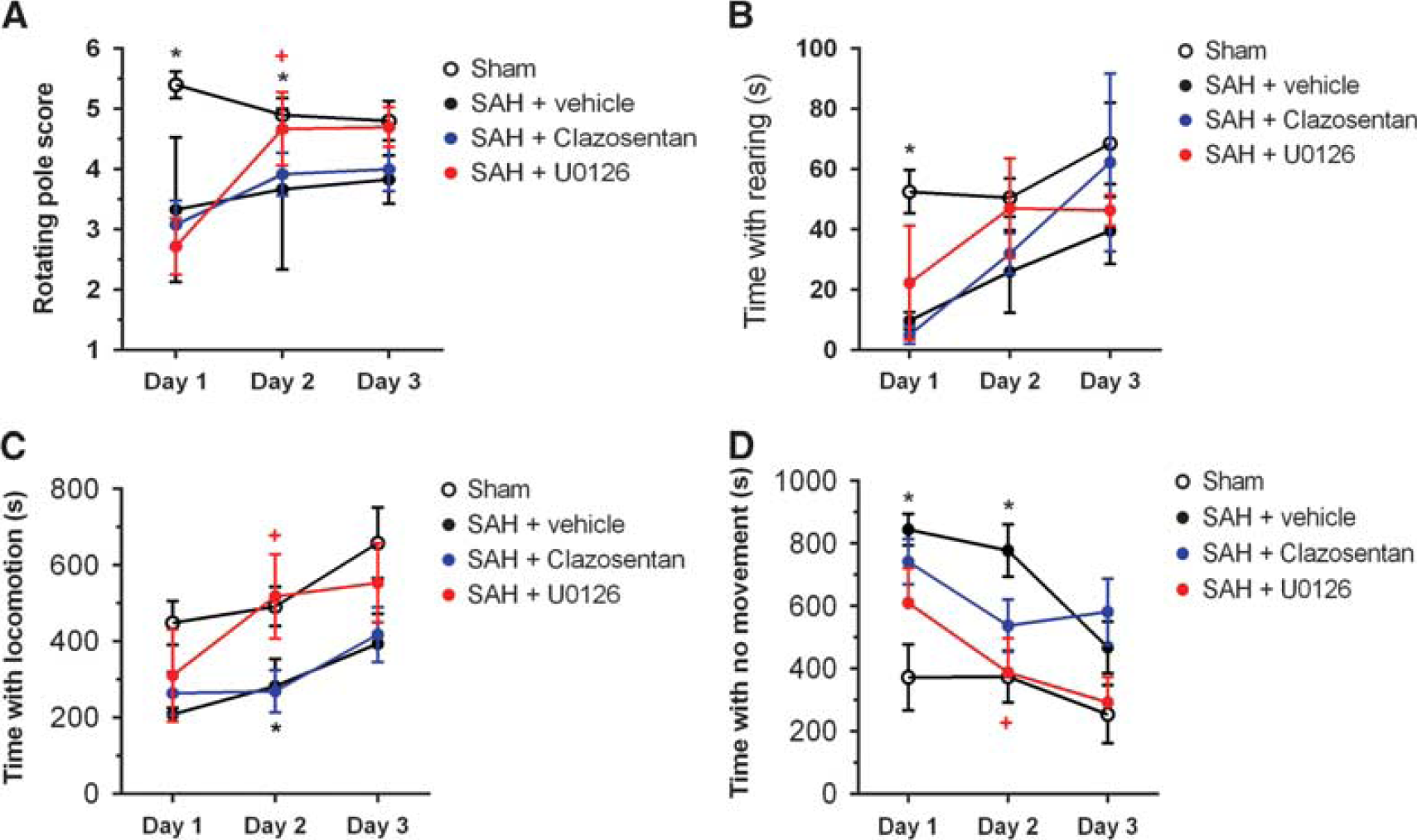
Effect of clazosentan and U0126 on neurologic function and spontaneous behavior after SAH. (
As a supplement to the rotating pole test, we assessed outcome in the animals by quantifying time spent by locomotion, no movement, and rearing (Figure 7). These parameters showed stable levels in the sham-operated animals post surgery, whereas the SAH animals revealed the impairment on behavioral patterns. The spontaneous behavior of U0126-treated animals was significantly improved, whereas this was not the case for clazosentan-treated animals.
Discussion
This study is the first to directly compare the effects of the endothelin receptor antagonist clazosentan and an inhibitor of MEK1/2, U0126, on mechanisms putatively involved in the development of late cerebral ischemia after SAH. Ample evidences exist that clazosentan blocks the contractile responses to ET-1
The first aim of this study was to examine the time course of receptor alterations in cerebral vascular smooth muscle for 4 days after SAH. There was a successive increase in contractile responses to ET-1 and 5-CT as evidenced in basilar and MCAs. Between day 3 and 4, there was considerable mortality of the animals as seen in this study (30%); those rats that appear most affected by the SAH die or have to be euthanized because of serious illness (according to Animal Ethics regulations). Thus, surviving animals have less upregulated responses and are less severely ill. This conclusion was supported by detailed analysis of receptor expression levels, quantitative measurements of CBF, and neurologic behavior scoring in an earlier study. 12 Therefore, the direct comparison of the effects of clazosentan and U0126 treatment were performed during a period of up to day 3 after SAH.
The second aim of the study was to investigate whether clazosentan had any effect on the delayed cerebrovascular upregulation of contractile receptors that we have demonstrated after SAH in earlier studies.22, 24 For comparison, we used the MEK1/2 inhibitor U0126 that has earlier been reported to prevent the SAH-induced vasoconstrictor receptor upregulation. 8 The administration of U0126 commencing 6 hours after the onset of SAH abolished the upregulation of endothelin and 5-HT receptors in accordance with previous studies.8, 21 In contrast, in animals treated with clazosentan after a similar administration regimen as for U0126, SAH-induced endothelin receptor upregulation was not significantly alleviated compared with vehicle-treated animals. The finding was confirmed both at the functional level in contractility experiments and by protein analysis with western blotting. Furthermore, neurology scoring after SAH was not different between clazosentan and vehicle-treated animals. However, in U0126-treated animals, the neurology score was significantly improved.
The present study offers support for the clazosentan trial data, which revealed an effect on vasoconstriction of cerebral vessels after SAH but no significant effect on the clinical outcome.5, 6 Meta-analysis of five randomized trials, four with clazosentan and one with TAK-044, reported an effect on angiographic vasospasm, less on LCI and nonexistent effect on overall clinical outcome.
5
This has been explained by the reduced availability of clazosentan to the abluminal side of the blood—brain barrier, which would limit the possibility to block endothelin-induced responses or because of side effects, such as hypotension or pulmonary complications. We have proposed that late cerebral ischemia is because of the upregulation of several G-protein-coupled receptors in cerebral arteries and, thus, it is necessary to prevent the upregulation of all of these contractile receptors to significantly modify the outcome after SAH.
10
The present study has made a direct comparison of clazosentan and the MEK1/2 inhibitor U0126, and included both vehicle group and sham-operated animals, and the results do induce support of this hypothesis.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.