
Abstract
We present a new method for inducing a circumscribed subcortical capsular infarct (SCI), which imposes a persistent motor impairment in rats. Photothrombotic destruction of the internal capsule (IC) was conducted in Sprague Dawley rats (male;
INTRODUCTION
Although the annual death rate due to stroke has decreased recently, there has been a growing prevalence of strokes affecting subcortical white matter in elderly people.1, 2, 3 A recent meta-analysis revealed that strokes are highly associated with white-matter lesions, leading to poor clinical and functional outcomes. 2 Among white-matter lesions, infarction of the internal capsule (IC) is known to have a negative clinical prognosis because the posterior limb of the IC (PLIC) constitutes the core of the subcortical motor pathway and contains the major corticofugal tract that is directly related to motor function.4, 5 Consequently, damage to the PLIC from a stroke will likely lead to a persistent motor disability and a deterioration of the ability to accomplish daily life activities.
Animal models have been used to understand the pathophysiology of stroke and to guide the development of more effective therapeutic or rehabilitative interventions. Although many studies of therapeutic strategies have been performed using cortical infarct models, only a few studies have investigated subcortical capsular infarcts (SCIs), owing to a lack of pertinent rodent models for capsular infarct.6, 7, 8 Specifically, to investigate motor deficits and their recovery after a stroke, a portion of the motor pathway from the motor cortex to the medullary pyramid should be selectively destroyed or modified to create animal models that have motor impairment. However, most of these models involve damage within the gray matter of the cortex, and only a few studies have attempted to damage the white matter to develop a stroke model. There are several possible reasons for the lack of rat models of white-matter stroke. For example, rats have substantially less white matter than nonhuman primates or humans. 7 The IC in a rat has an irregular, elongated structure, making it difficult to access it stereotactically from the surface of the brain and to control the infarct location accurately. Additionally, no efficient tools have yet been developed to selectively destroy the planned extent of the target structures.6, 7
Only a few models have been successful in manifesting a persistent and marked sensorimotor deficit after SCI.6, 7, 8 During the last decade, it has been a challenge to create a persistent SCI model. Several methods have been developed and tested, including occlusion of the middle cerebral artery, occlusion of the anterior choroidal artery, and injection of the vasoconstrictive peptide endothelin-1 into the PLIC.8, 9, 10, 11 Occlusion of the proximal middle cerebral artery, a widely accepted stroke model, may induce infarction in the IC by interrupting the blood supply from lenticulostriate arteries; however, the extent of infarction often affects neighboring structures, such as the basal ganglia, and motor impairment is not consistent because the infarcts vary in size.12, 13 Occlusion of the anterior choroidal artery in a miniature pig successfully generates a lacunar infarction, mostly in the IC; however, motor impairment returned to normal by day 10 after a stroke in this model. 9 Recently, injection of endothelin-1 has been considered as the most reliable way to simulate a capsular infarct while preserving the cortical motor cortex.6, 7, 8 However, the destruction of IC fibers in this model was incomplete, leading to a lack of marked deficits in various tests of unskilled sensorimotor behavior. Establishing an animal model that is associated with persistent behavioral deficits is important for validating the model and for monitoring recovery (e.g., improvement of motor function or increased plasticity) when therapeutic or rehabilitative interventions are introduced.14, 15 Also, visualization of neural activity after the infarct may be important for further research on functional recovery. 16
The aim of this study was to use the photothrombotic technique to establish a SCI model that manifests a motor impairment and that can potentially be used to evaluate motor recovery using novel therapeutic or rehabilitative interventions. MicroPET (positron emission tomography) with 2-deoxy-2-[18F]-fluoro-D-glucose ([18F]-FDG) and a behavioral test were used to characterize functional changes related to SCI. This model will be useful for future studies of the mechanism of motor recovery and the progress of brain plasticity during rehabilitative treatment.
MATERIALS AND METHODS
Experimental Animals
Animal experiments were performed according to the institutional guidelines of the Gwangju Institute of Science and Technology, which are compliant with McGill University guidelines for experimental research. ARRIVE guidelines were followed in the preparation of the manuscript. Rats were housed two per cage in a controlled animal husbandry unit at 21±1°C with water
Induction of Photothrombotic Capsular Infarction
Male Sprague Dawley rats (
Behavioral Evaluation
Three types of behavioral tests were performed; two of the three tests were unskilled-behavior tests that consisted of forelimb placing and forelimb use asymmetry tests, and the last test was a skilled-behavior test that included single pellet reaching tasks (SPRTs). In the forelimb placing test, rats were held with forelimbs moving freely and moved to lightly touch the tabletop with each side of their vibrissa or the ulnar side of their forelimb. Ten trials were conducted for each forelimb, and the percentage of the trials in which the rats placed the preferred forelimb on the edge of the table in response to the stimulation was recorded. 17 In the forelimb use asymmetry test, rats were placed in a cylinder for 2 minutes to check the frequency of the use of ipsilateral or contralateral forelimbs to support an upright body posture. The test score was calculated as a percentage of forelimb usage contralateral to infarct in each session. 17 For SPRT, the experimental apparatus was made of clear Plexiglas (40 cm × 45 cm × 13.1 cm wide) with a 1-cm wide slit in the middle of the front wall. The food shelf was attached in front of the midline slot. 18 Once rat's reach began to show a forelimb preference to take a sucrose pellet (Bio-Serve, Frenchtown, NJ, USA) through the slit, a pellet was obliquely placed contralateral to the preferred paw to prevent the use of the nonpreferred paw. Subsequently, the animals were administered 20 pellets per session for 3 weeks. Successful reach was defined as a reach in which an animal grasped a food pellet, brought it into the cage, and consumed it without dropping the pellet. Reaching performance was scored as the percentage of successful reaches as defined by the following formula:

Performance scores from three sessions before the operation were averaged and used to represent preoperative reaching performance.
Skilled reaching performance is the primary outcome measure in stroke models, and a motor recovery level is a typical inclusion criterion in stroke patients. We measured the reaching success rate for the lesioned group, and the rats were subdivided into immediate (IRG), moderate (MRG), and poor recovery groups (PRG) on the basis of their performance during the 2 weeks after capsular infarct. If the reaching performance recovered >50% in 1 week, then the rats were classified into the
Micro-Positron Emission Tomography/Computed Tomography Scanning and Image Analysis
At postlesion day 4 (PL4), when a mature infarct lesion and an overt functional disconnection were assumed, changes in regional glucose metabolism related to capsular infarct were evaluated using an [18F]-FDG microPET/CT scanner (Inveon; Siemens Medical Solution, Knoxville, TN, USA), which has a transaxial resolution of 1.4 mm full width at half maximum and a field of view of 12.7 cm. Each rat was scanned twice: the first scan before lesioning (baseline), and the second scan at PL4. The rats were deprived of food for 12 hours before scanning and were injected with [18F]-FDG (0.1 mCi/100 g) through the tail vein under brief anesthesia with isoflurane. After an uptake period of 30 minutes, the animals were anesthetized by inhalation of isoflurane (2% in 100% oxygen) and placed prone on the scanning bed with their head immobilized using a custom-made head holder (Hyosung Inc., Gwangju, Korea). The body temperature was maintained at 36.5±2°C, and vital signs, including respiration, heart rate, and body temperature, were monitored during standard scanning procedures (BioVet; m2m Imaging Corp, Newark, NJ, USA). A 25-minute static acquisition with 5 minutes of attenuation correction computed tomography scan was performed. After scanning, the images were corrected for attenuation, and all of the images were reconstructed using the iterative OSEM3D/MAP algorithm. Imaging analysis was performed using a MINC tool kit (McConnell Brain Imaging Centre, Montreal Neurological Institute, Montreal) and VINCI (http://www.nf.mpg.de/vinci3). All images were manually coregistered to a standard histologic template and Schweinhardt atlas in Paxinos coordinates.19, 20 Intensity normalization was conducted using the proportional method. To assess the initial infarct-induced regional glucose metabolic changes, we performed a voxelwise analysis between the baseline and the PL4 images for each group (PRG or MRG) using a paired
Neurohistologic Examination
After 3 weeks of behavioral evaluation, the rats were killed, and transthoracic cardiac perfusion was performed using a 4% paraformaldehyde solution. The brains were then removed and coronally cut into sections with a thickness of 4
Statistical Analysis
Data were analyzed using the SPSS, V10.0 statistical analysis software (SPSS Inc., Chicago, IL, USA). Forelimb placing, forelimb use asymmetry, and skilled reaching performances were analyzed using repeated measure analysis of variances for the effect of groups and times.
RESULTS
Behavioral Tests
All of the experimental animals were impaired when tested throughout a series of three behavioral tests. A total of 8 animals displayed a level of recovery that led them to be categorized in the MRG, 9 rats in the PRG, 7 rats in the SOG, and 14 rats in the IMG. Therefore, our SCI model produced a persistent motor impairment in 63% of animals. Both the PRG and the MRG showed a significant decrease in forelimb placing in response to forelimb stimulation compared with the SOG during the 3 weeks after induction of SCI (
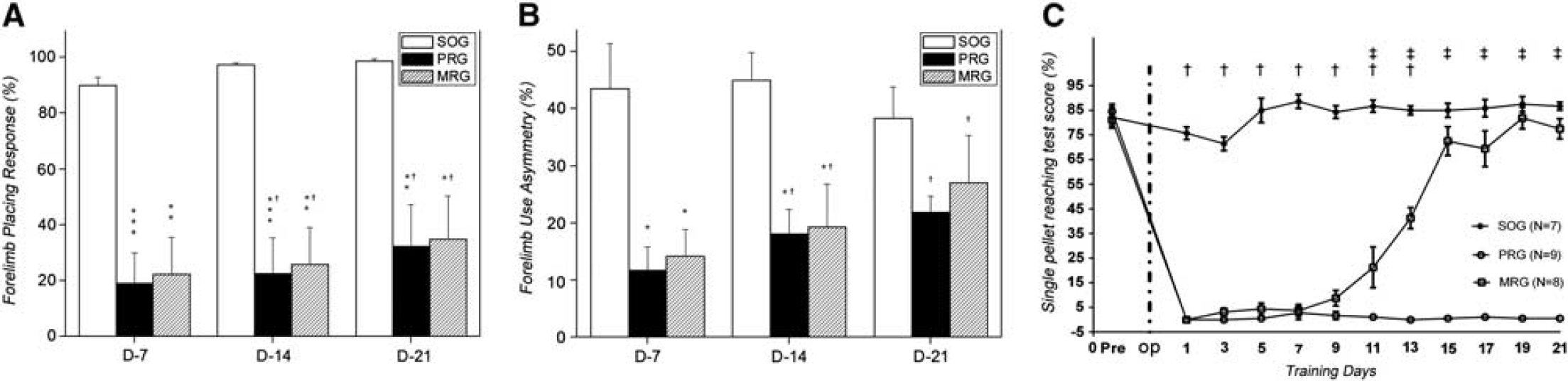
Behavioral tests in the photothrombotic capsular infarct models and SOG. (
Neurohistologic Findings
Histologic examination of specimens 3 weeks after SCI showed circumscribed infarct lesions in the PLIC. At low power magnification (× 15), a round-to-ovoid cystic cavity surrounded by reactive fibrillary astrocytes and a few macrophages was observed in hematoxylin and eosin-stained sections (Figure 2A). The presence of reactive astrocytes delineating the cystic cavity was clearly identified on the sections that were stained for glial fibrillary acidic protein immunohistochemistry (Figure 2B). The subcortical white matter and destruction of capsular fibers were well defined by neurofilament protein-M/H immunohistochemistry (Figure 2C). The Luxol fast blue-PAS stain, which highlights the myelin sheath of axon bundles, showed a clear loss of myelin sheaths and a few macrophages containing PAS-positive myelin debris (Figure 2D). At a higher magnification (× 40), it could be seen that lesioning with low energy produced an elongated and circumscribed destruction of the capsular fiber that was confined to the IC and did not encroach on the neighboring striatum and optical tract (Figures 3A and 3B). In addition, there was mild compression of the molecular layer of the cortex. There were minor histopathologic changes along the optical fiber tracts, including cortical gray matter, fimbria of hippocampus and striatum, in both sham and experimental groups; however, the sham group did not show damage within the underlying IC.
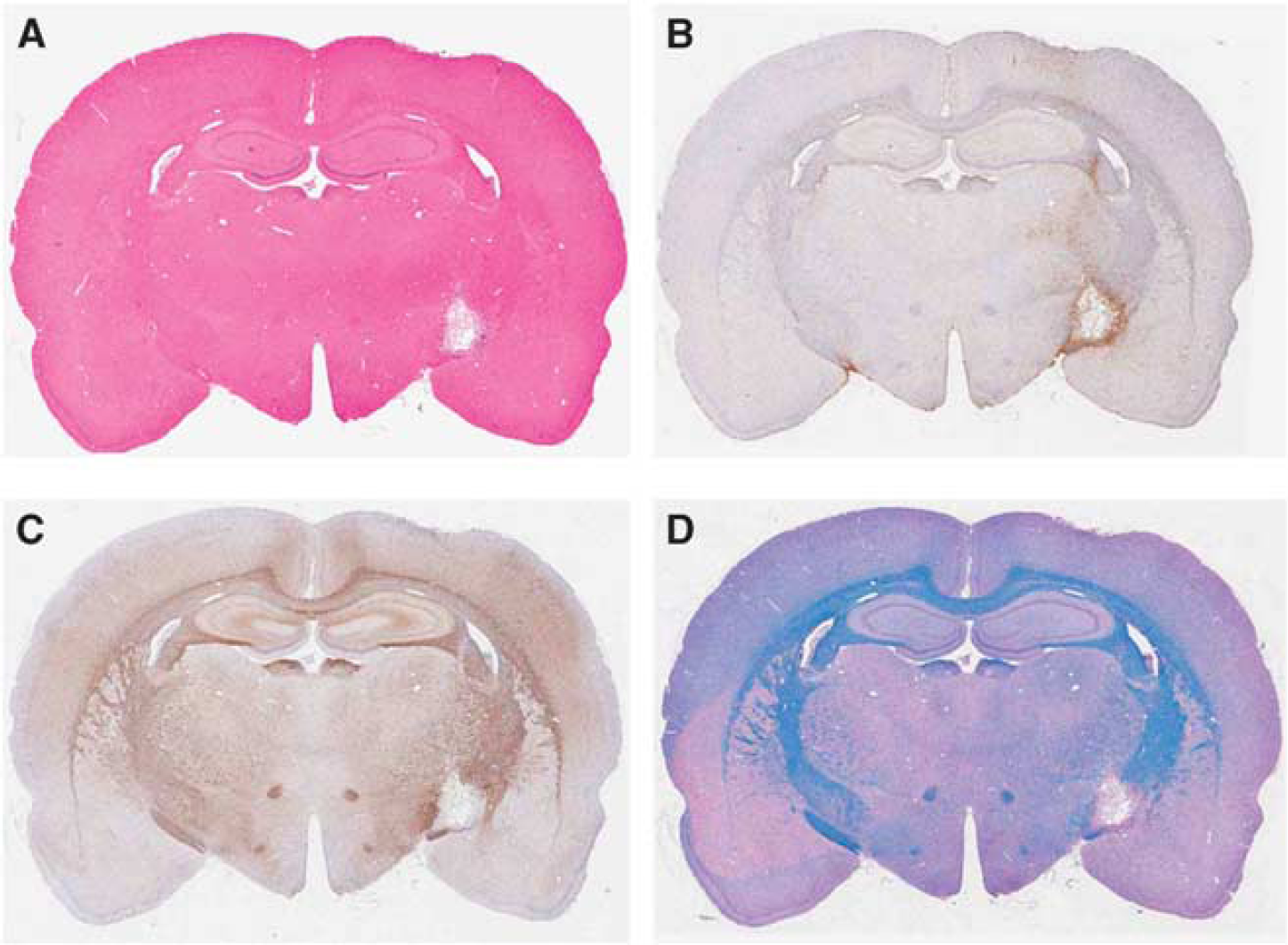
Histopathologic features showing the destruction of internal capsule (IC) in a subcortical capsular infarct (SCI) model by hematoxylin and eosin (H&E) staining (
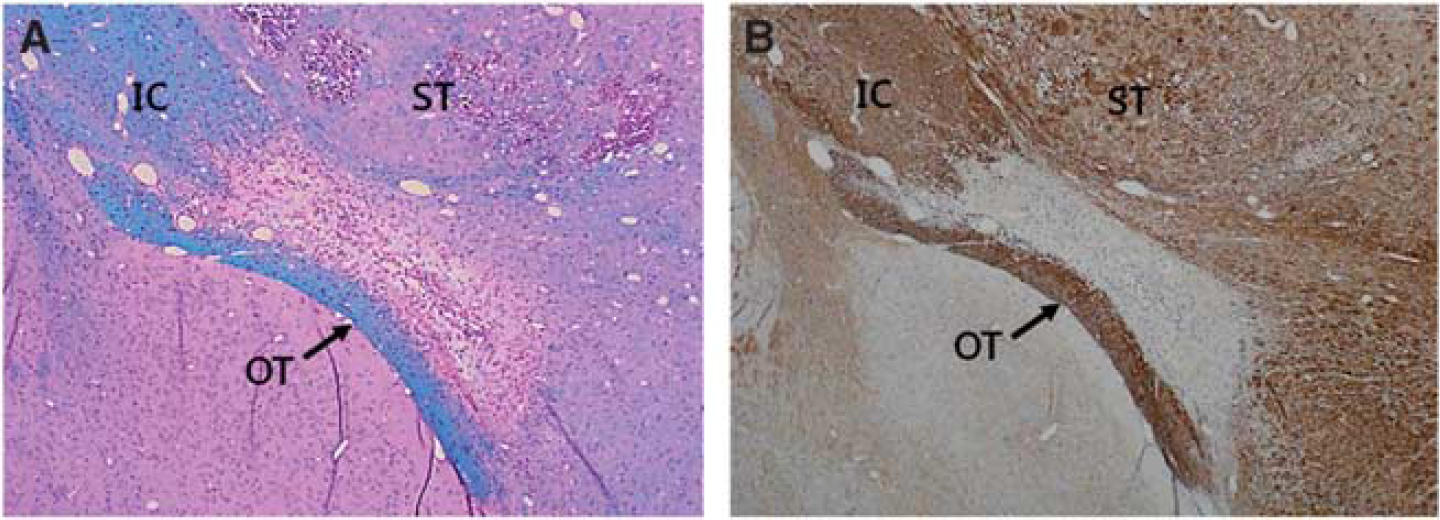
Histologic staining of brain sections showing the selective destruction of the white-matter tract in the subcortical capsular infarct (SCI) model using neurofilament protein-L (× 40) (
The mean infarct volume, which includes the area of necrosis and surrounding demyelination, was 0.6±0.2 mm3 in the PRG and 0.5±0.2 mm3 in the MRG, measured in serial sections. The infarct volume was not related to the degree of motor recovery (see Supplementary Information Figure 2). However, the PRG showed more complete, full thickness destruction of the fiber tract at the anterior part of the PLIC, whereas the MRG showed partial destruction of the IC on serial sections of the brain (see Supplementary Information Figure 3). Incidentally, the optic tract laid adjacent to the IC was partially injured.
Change in Regional Glucose Metabolism
(see Supplementary Information Figure 1 & Supplementary Movie 1). Figure 4 and Table 1 summarize the PET [18F]-FDG changes in regional glucose metabolism at PL4 compared with prelesion (baseline) scans, based on the significance threshold (local maxima,
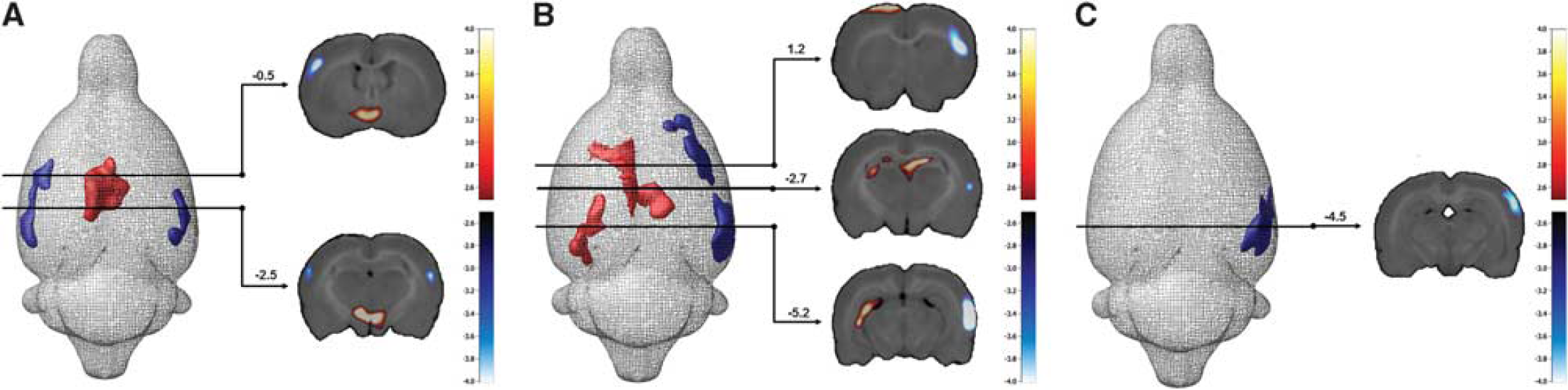
MicroPET imaging showing a significant glucose metabolic difference between baseline and postlesion 4 day in the moderate recovery (
Brain areas of significant difference of regional glucose metabolism between baseline and postlesion 4 day scan (
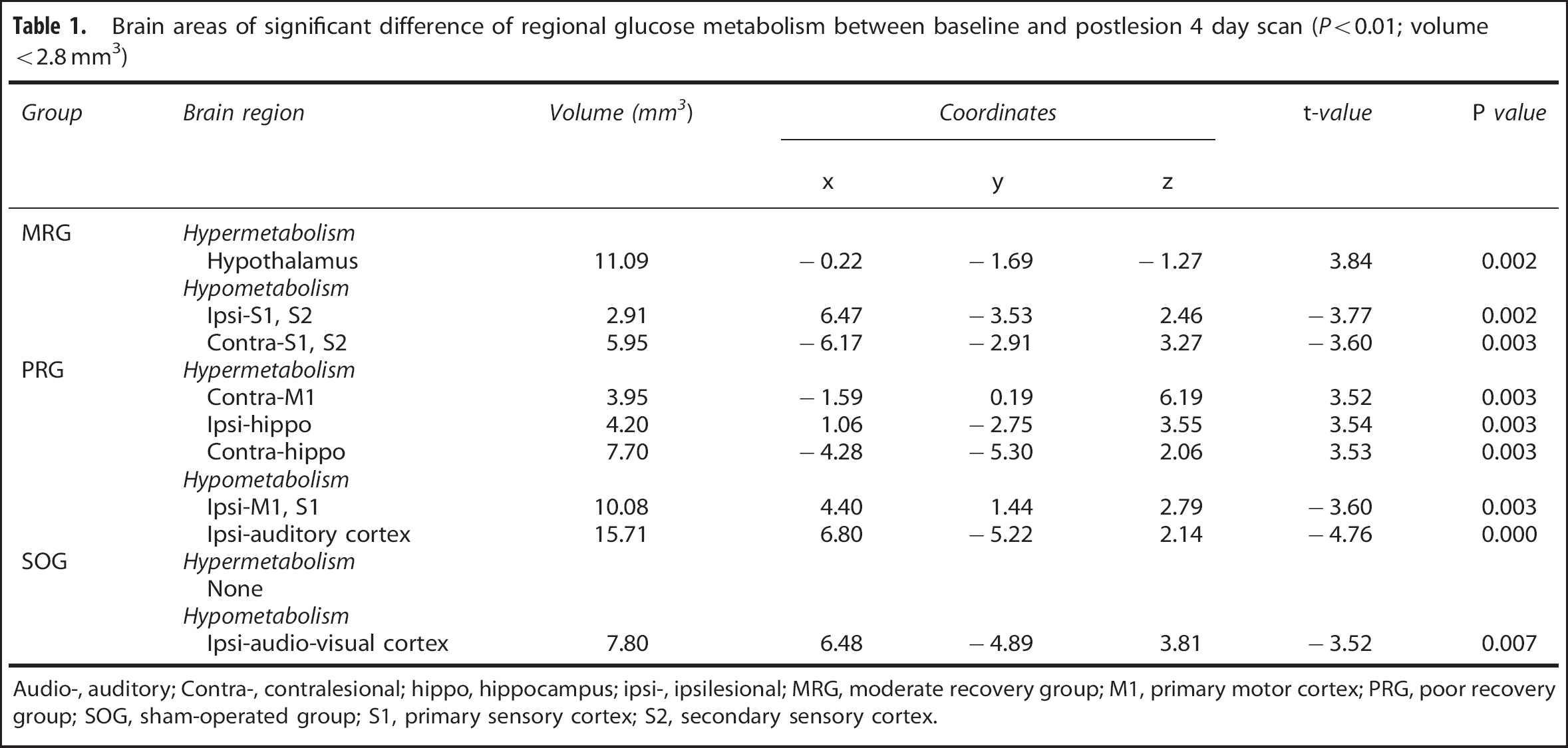
Audio-, auditory; Contra-, contralesional; hippo, hippocampus; ipsi-, ipsilesional; MRG, moderate recovery group; M1, primary motor cortex; PRG, poor recovery group; SOG, sham-operated group; S1, primary sensory cortex; S2, secondary sensory cortex.
DISCUSSION
The present study has shown the feasibility of generating an SCI model by photochemically inducing an infarction in the IC. Photothrombotic infarction modeling was advantageous in selectively producing an infarct in white matter due to its optic properties. We also showed that this model is associated with a marked and persistent motor impairment and a decrease in metabolic activity, predominantly in the ipsilesional motor and sensory cortex. Complete destruction of the IC is more likely than incomplete destruction of the IC to lead to a persistent motor impairment; incomplete IC destruction produced rather than gradual recovery of motor function. The use of a more ventral target at the anterior part of the PLIC compared with previous reports is likely to generate severe motor impairment.6, 8
Assessing the progress of motor recovery is an essential measure for rehabilitative intervention in SCI. Earlier studies on stroke have suggested other rodent models to be unrealistically favorable because the animals used in those studies were mostly young and healthy rats with brains that had a relatively high capacity to compensate for functional loss. 16 Furthermore, the degree of motor impairment was not sufficient to allow precise comparative evaluation of the efficacy of therapeutic or rehabilitative intervention. Specifically, a capsular infarct is known to have a bad prognosis in a clinical setting. During the first year after a stroke, for example, lesions of the IC were associated with a significantly lower probability of isolated hand motor function returning than lesions of cortex, subcortex, or corona radiata. 21 In this sense, our model showed a marked and persistent motor impairment similar to chronic neurologic deficit, which properly models the long-term functional (motor) deficits of chronic stroke patients.
We created a model using photothrombosis. Photothrombosis is well established as being useful for creating infarction lesions in the cortex. It has been reported that the size of a photothrombotic infarct may be altered with high reproducibility by adjusting the intensity of light output and the size of the irradiated area in the cortex.22, 23 Similarly, we were able to selectively destroy the IC with minimal damage to the neighboring striatum by making a straight optical fiber to reach the target region accurately. The selectivity of lesioning was based on two optical properties of the laser light. First, the scattering of light was >4 times higher in white matter than in gray matter. 24 Accordingly, if the intensity of light has a low enough irradiance (<814 mW/mm2), then one can limit the extent to which photothrombosis lesions affect the target area (i.e., IC). Considering that the striatum is the most vulnerable region in the brain, 25 the use of the difference in optical properties between gray and white matter may be helpful to achieve a localization of infarct lesions in the white matter with only a minimal encroachment on the striatum. Second, the penetration of light energy was very limited. Approximately 99% of light energy was lost beyond 1 mm from the source of light. 26 It has been postulated that light of higher energy can induce infarcts in both gray and white matter, whereas lower energy light could induce photothrombosis only in white matter. We suggest that this technique may be useful for generating an infarct in any restricted location in white matter, and result in functional loss related to the anatomic structure of the lesion.
In our study, a small lesion in the PLIC resulted in a marked impairment of unskilled and skilled behaviors. This was compatible with anatomic evidence showing the condensation (overlapping) of corticospinal tract fibers at the IC. Similarly, a complete lesion in the pyramid, where corticospinal fibers are also condensed, has reportedly produced severe, long-lasting motor impairment in contralateral forelimb movement.27, 28 Nonetheless, partial lesions of the PLIC resulted in a substantial sparing of movement or less severe impairment of the contralateral limb. 28 It is noteworthy that previous models, generated by the injection of endothelin-1, showed selective destruction of the IC with a measurable motor deficit, but the degree of the motor deficit was not as severe as those resulting from sensorimotor cortex lesions.6, 8 In our study, the experimental animals that had incomplete destruction of the IC, as shown in the MRG, were likely to show gradual recovery after 1 week following lesioning, whereas those that had complete destruction of the IC showed a severe degree of motor deficit similar to complete lesioning in the pyramid. Previous observations indicated that the extent of the lesions is related to the severity of motor deficit.29, 30 Therefore, it is plausible to reason that previous models spared the critical portion of the IC. In this study, we attempted to compromise the genu portion and PLIC by lowering the target regions compared with previous models. In addition to the anatomic parameters of the lesion, motor recovery is influenced by various factors. To accurately predict the motor outcome, we suggest that 2 weeks of observation is mandatory for the selection of an appropriate model that requires a consistent motor deficit.
Together with local brain changes, stroke produces neurologic, structural, metabolic, and electrophysiologic effects in remote ipsilateral or contralateral brain areas.31, 32, 33 The present PET [18F]-FDG findings at PL4 might reflect an earlier regional metabolic adaptation imposed by SCI, rather than a permanent change in the brain network.34, 35, 36 Further imaging studies should be conducted to better define metabolic adaptations and to indicate their predictive power regarding individual functional recovery. In our study, we observed that the SCI resulted in hypometabolism in the ipsilesional motor and bilateral sensory cortex, whereas hypermetabolism was observed in the contralesional motor cortex. This result is in line with previous fMRI studies conducted in the early stages of a unilateral stroke that showed that ipsilesional functional impairment is associated with contralesional activation.37, 38 Interestingly, the bilateral hippocampal hypermetabolism observed in the PRG might reflect neural adaptation associated with implicit learning of SPRT in this experiment. 39 This finding may support the role of the hippocampus in motor recovery from a stroke. 40 In contrast, the hypometabolism in the auditory and visual cortex and hypothalamus suggests that metabolic changes occurring during recovery from the IC lesion lead to functional brain adaptations throughout a wide area. However, further studies are necessary to clarify the temporal evolution of these adaptations.
Despite its usefulness, our model may have limitations. First, despite the selectivity of the lesioning technique, the optic tract adjacent to the IC was often observed to be partially damaged. We assume that this is because the optic tract, a type of white matter, has a higher scattering rate than the IC. Second, although we conducted a functional imaging study at PL4, it may not be sufficient to identify the dynamic pattern of functional reorganization. Longitudinal studies using the SCI model will be necessary to assess this issue. Nonetheless, the findings from functional imaging may provide significant information to determine the influence of SCI during the early stages of a stroke.
CONCLUSION
The present study showed an unprecedented PLIC lesion that is able to impose a marked and prolonged motor impairment. Behavioral, histologic, and functional imaging findings support the usefulness of this novel SCI rat model for investigating motor recovery and the mechanisms underlying SCI. This model may allow the use of longitudinal PET imaging to quantify the molecular mechanisms that underlie recovery from SCI.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.