
Abstract
[ 18 F]fallyprlde is a high-affinity dopamine D2/3 receptor tracer with the ability to reliably quantify D2/3 receptor sites in both striatal and corticolimbic regions. The translational potential of [ 18 F]fallypride imaging is, however, limited by the lengthy scanning sessions (60–80 minutes duration over a total of 3–4 hours) required by current protocols. The aims of our study were to adapt [ 18 F]fallypride imaging for use in clinical populations with neurological and neuropsychiatric disorders, by reducing the duration of individual scanning sessions;and to establish the reproducibility and reliability of our adapted protocol in healthy older people. Eight participants (five male and three female;mean age = 75.87 ± 4.39 years) were scanned twice, 4–6 weeks apart. [ 18 F]fallypride binding potential was determined from image data collected during three sampling times: 0-30;60-90;and 210–240 minutes post injection. High reproducibility and reliability (test-retest variability <8%;intraclass correlation coefficient >0.8) were observed in all but the prefrontal regions, and remained so when sampling times were reduced to 20 minutes (0-20;70-90;220-240 minutes). The adapted protocol is feasible for use across neuropsychiatric disorders in which dopamine has been implicated and is sufficiently sensitive to detect within-subject changes between 2.7% and 5.5% in striatal and limbic regions.
INTRODUCTION
Since dopamine D2/3 receptors were first visualized
Another major development in imaging technology has been the use D2/3 PET tracers to image endogenous neurotransmitter release. The observation that D2/3 tracers compete with endogenous dopamine for receptor sites has been used in imaging paradigms to investigate the sensitivity of the dynamic system after pharmacological or behavioral challenge. 11 High-affinity D2/3 receptor tracers are increasingly used in this respect as they offer the opportunity to explore the role of corticolimbic dopamine release in human behavior12,13 and in a range of neurological and psychiatric illnesses including schizophrenia-spectrum disorders 14 and Parkinson's Disease. 15
[ 18 F]fallypride is unique among D2/3 receptor tracers, as it can provide stable estimates of both striatal and extrastriatal receptor availability within the same scanning session. 6 However, techniques currently used to quantify [ 18 F]fallypride binding involve multiple sampling periods (each lasting 60-80 minutes) over a total scan duration of 3-4 hours, to allow tracer uptake to achieve a plateau within the striatum where receptor sites are more densely concentrated.6,16 These imaging protocols are not feasible for use in many clinical populations, particularly older, cognitively impaired individuals or those with movement disorders. Adapting [ 18 F]fallypride imaging for use in clinical populations who are unable to tolerate lengthy scanning sessions would widen its potential for use in understanding disease mechanisms, drug occupancy, and dopamine release in response to pharmacological and behavioral challenge.
The aims of the study were as follows:
To adapt [ 18 F]fallypride imaging by reducing the length of individual scanning sessions to 30 minutes.
To establish the test-retest reliability of the adapted protocol in healthy older people.
To investigate whether sampling times could be further reduced to 20-minute sessions without reducing reliability.
MATERIALS AND METHODS
Sample
Eight healthy older adults (five male and three female; mean age = 75.87 ± 4.39 years) were recruited to the study. Participants were ‘healthy controls’ identified from the Dementia Case Register database within the South London and Maudsley (SLaM) NHS Trust, funded by the National Institute of Health Research (NIHR Biomedical Research Centre). All participants gave written informed consent. The study was approved by the Joint South London and Maudsley and the Institute of Psychiatry NHS Research Ethics Committee. Permission to administer [ 18 F]fallypride was given by the Administration of Radioactive Substances Advisory Committee. Before their involvement, a full medical and psychiatric history was taken from participants, including dementia screening using the Mini-Mental State Examination. 17 Exclusion criteria included (i) current or past neurological or psychiatric illness, including drug and substance abuse; (ii) Mini-Mental State Examination score <26; (iii) history of any cerebrovascular event; (iv) use of estrogen replacement therapy or other medications, which may have affected brain dopamine activity; (v) needle phobia; and (vi) other medical conditions that might affect the ability to tolerate a brain scan, such as significant cardiorespiratory disease or severe kyphosis. Structural imaging (T1-weighted magnetic resonance imaging (MRI)) was carried out at the Centre for Neuroimaging Sciences to exclude intracranial abnormalities.
PET Imaging Procedure
Participants were scanned twice at rest, 4–6 weeks apart, on a GE (GE Healthcare, Hatfield, UK) VCT Discovery PET-CT camera (FWHM 5 mm), at St Thomas’ PET Centre. A molded head rest and straps were used to minimize head movement and an external webcam was used to detect significant head movements that could degrade the quality of image data. [ 18 F]fallypride was administered via a single bolus intravenous injection of 250 MBq. Each scanning session consisted of three dynamic scans in three-dimensional (3D) mode, each lasting 30 minutes, and preceded by a low-dose computed tomography scan for attenuation correction. Image data were collected during three scanning sessions, determined from previous [ 18 F]fallypride studies in young adults;16,18,19 0–30 minutes to provide an input function to model a reference region approach; 60-90 minutes to capture peak tracer binding within extrastriatal regions; and 210–240 minutes to ensure that tracer binding had achieved a plateau in the striatum of all participants (in a small proportion of people, the tracer may take up to 210 minutes to achieve equilibrium) 20 and to achieve a good model fit. The initial 3 minutes of the first scanning session acquired frames with short duration (1 × 10 seconds, 10 × 5 seconds, 6 ×10 seconds, 1 × 20 seconds). The remaining 87 minutes of scanning were acquired using frame lengths of 1 minute.
Image Analysis
Data were analyzed using a simplified reference tissue model 21 and the cerebellum as a reference region. This approach has been previously validated for the quantification of [ 18 F]fallypride BPND 22 and found to have good reproducibility and reliability. 23 Preprocessing was performed using SPM8 (www.fil.ion.ucl.ac.uk/spm/software/spm8/) and all other analyses using Matlab (www.mathworks.com). [ 18 F]fallypride images were processed using SPM8 in Matlab. Non-attenuation corrected, fully 3D iteratively reconstructed PET scans (GE ‘VuePoint’ reconstruction algorithm, 2 ierations, 28 subsets, 4.8 mm Hanning 3D-filter) were used for frame-by-frame realignment. These transformations were then applied to attenuation-corrected (AC) filtered back projected (Fourier-rebinned 2D reconstruction, with geometric, deadtime, scatter, and random correction, 2.8 Hanning Transaxial filter, GE Scanner) PET images, which were used for quantification, and AC-VuePoint PET images (4 iterations, 28 subsets, 4.8 mm Hanning 3D-filter) used for warping atlases. All images were reconstructed to 128 × 128 × 47 voxels with dimensions 2 × 2 × 3.27 mm 3 .
Method 1
Image data collected over the three sampling times (0-30; 60-90; and 210-240 minutes) were used to quantify binding of [ 18 F]fallypride to dopamine D2/3 receptors, expressed as BPND. 24 The cerebellar reference region was defined using the Automated Anatomical Labeling atlas 25 and included all cerebellar regions apart from the vermis. Regions of interest (ROI) in areas with specific binding were defined using the Tzioritzi atlas 26 and included the caudate, putamen, medial and inferior temporal gyri, thalamus, amygdala, hippocampus, orbitofrontal cortex, and anterior cingulate gyrus.
In addition to the Tzioritzi atlas, we used a pre-existing template that defines the striatum in terms of its functional connections, and which has been previously used to quantify [
11
C] Raclopride BPND in people with Alzheimer's disease.
27
The striatal subdivisions were defined in standard space (Montreal Neurological Institute, MNI), using the parameters described by Martinez
We chose not to coregister MRI with PET data, as our specific aim was to establish the most widely applicable analysis method that would be suitable for use in older, cognitively impaired individuals, in whom MRI may be contraindicated or difficult to tolerate. As an alternative, atlases (and the striatal functional subdivisions template) were warped to subject space via a PET [ 18 F]fallypride template in standard (MNI) space. The [ 18 F]fallypride template was created from six healthy young subjects, 29 using the following method:
Structural (MRI) data were spatially normalized to MNI space using the unified segmentation algorithm in SPM.
These transforms were applied to each of the coregistered summed (3–30 min) AC-VuePoint PET images.
A mean [ 18 F]fallypride template was calculated by scaling each transformed PET image by the subject global mean, and then taking the mean of the six PET images.
Method 2
Sampling times were reduced from 30 to 20-minute blocks (0–20; 70–90; and 220–240 minutes). All other aspects of the image analysis were identical to Method 1.
Statistical Analysis
All statistical analysis was carried out using SPSS 19 (www.spss.com). A paired
RESULTS
Administered dose of [
18
F]fallypride was 244.1 ± 7.3 MBq. There were no significant differences in administered dose between scan 1 and scan 2 (mean difference = 0.5 ± 10.8 MBq,
Reliability Analysis
Method 1
Time–activity curves for Method 1 (30-minute sampling times) are shown in Figure 1 (all ROI defined using the Tziorotzi atlas), Figure 2 (extrastriatal ROI, defined using the Tzioritzi atlas), and Figure 3 (striatal functional subdivisions), and represent the AC filtered back projected data on which the kinetic analysis was carried out. Mean percentage test–retest differences (% variability) and reliability (ICC) of regional [ 18 F]fallypride binding for Method 1 are presented in Table 1. Reproducibility was excellent within the caudate, putamen, amygdala, and inferior temporal gyrus, where <5% variability was observed.
Test–retest reproducibility of regional [ 18 F]fallypride binding using method 1 (3 × 30 minutes)
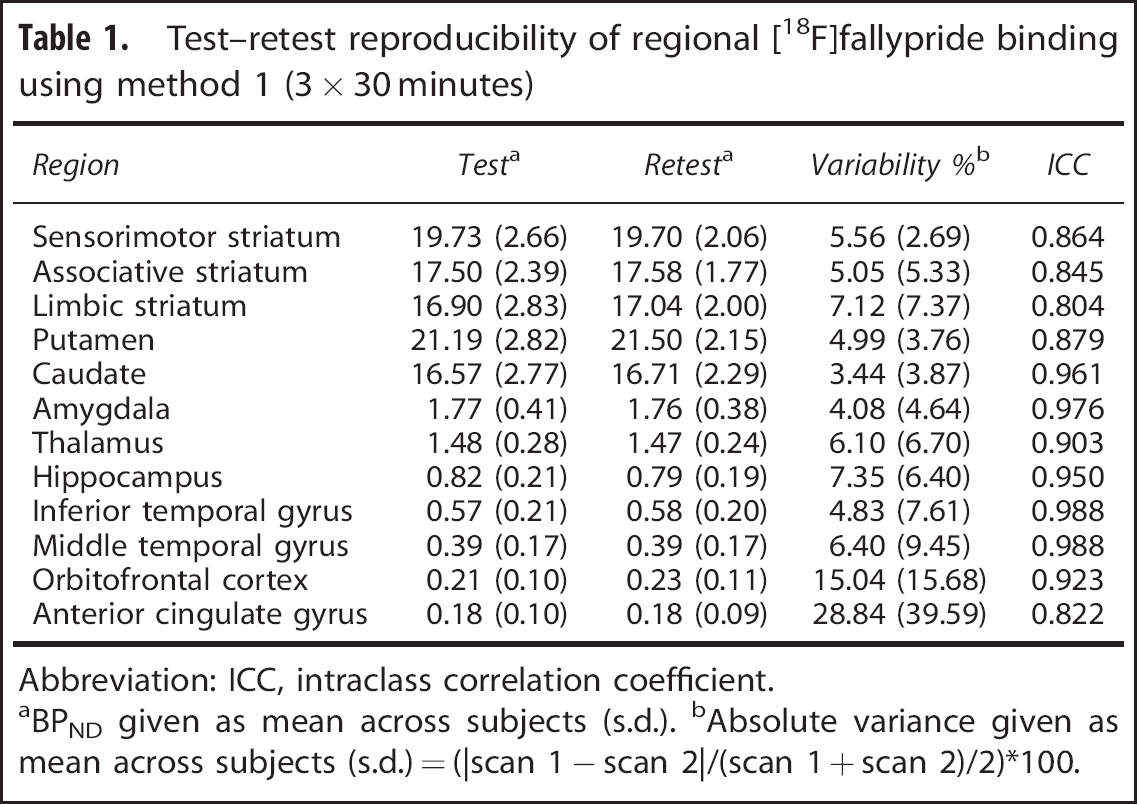
Abbreviation: ICC, intraclass correlation coefficient.
aBPND given as mean across subjects (s.d.).
bAbsolute variance given as mean across subjects (s.d.) = (|scan 1 – scan 2|/(scan 1 + scan 2)/2)*100.
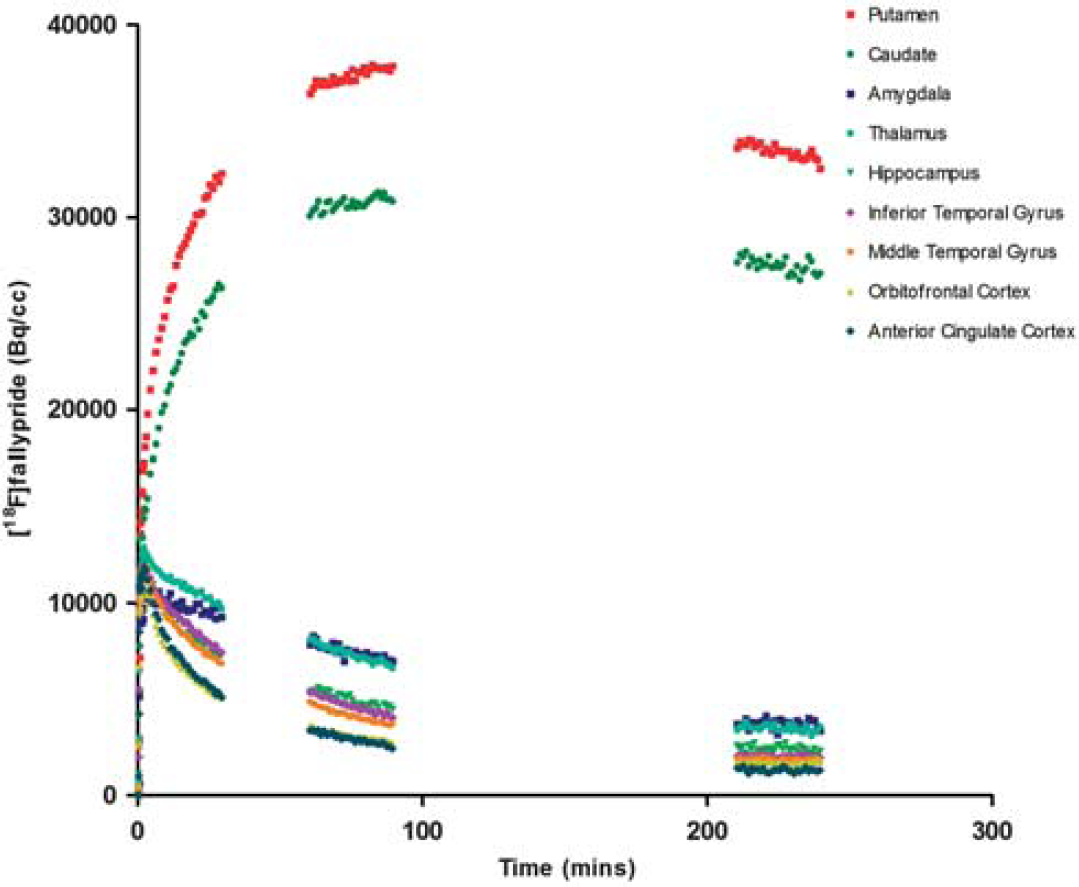
Time–activity curves (Method 1) are shown for regions of interest defined using the Tziortzi atlas and represent [ 18 F]fallypride uptake in a single participant.
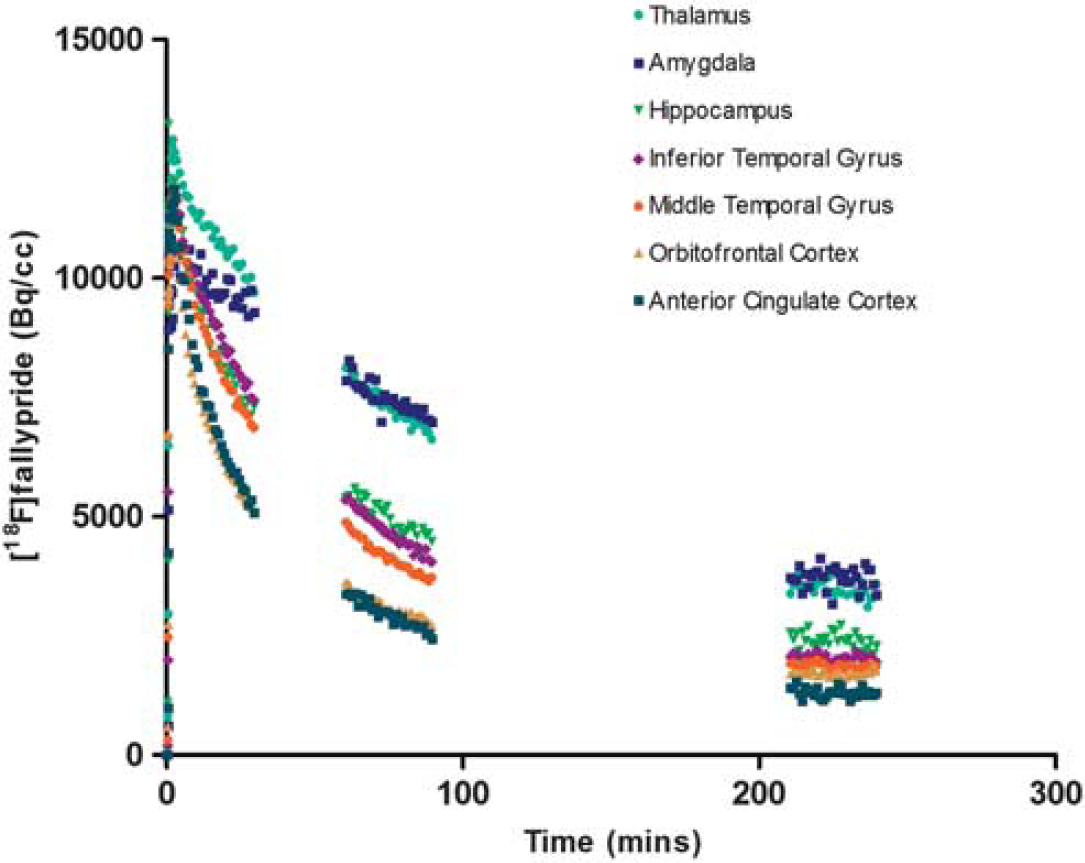
Time–activity curves (Method 1) are shown for extrastriatal regions of interest and represent [ 18 F]fallypride uptake in a single participant.
All of the other regions examined showed high reproducibility (<8% variability), with the exception of the orbitofrontal cortex (15.04% variability) and anterior cingulate gyrus (28.84% variability). Reliability (ICC) ranged from 0.804 (limbic striatum) to 0.988 (inferior and middle temporal gyri).
Method 2
Mean percentage test-retest differences (% variability) and reliability (ICC) of regional [ 18 F]fallypride binding for Method 2 (20-minute sampling times) are presented in Table 2. Reproducibility remained excellent (< 5% variability) in the caudate and amygdala, and high (< 8% variability) in all but the limbic striatum (8.25% variability) and prefrontal regions (orbitofrontal cortex = 17.45%;anterior cingulate gyrus = 37.35%). Intraclass correlation coefficient values ranged from 0.794 (anterior cingulate gyrus) to 0.986 (inferior and middle temporal gyri). When regional ‘test’ BPND values were compared across the two methods (shown in Table 2) mean variability was 3.19% or less in all regions sampled apart from the anterior cingulate gyrus (14.47%) (shown in Table 2).
Test–retest reproducibility of regional [ 18 F]fallypride binding using Method 2 (3 × 20 minutes)
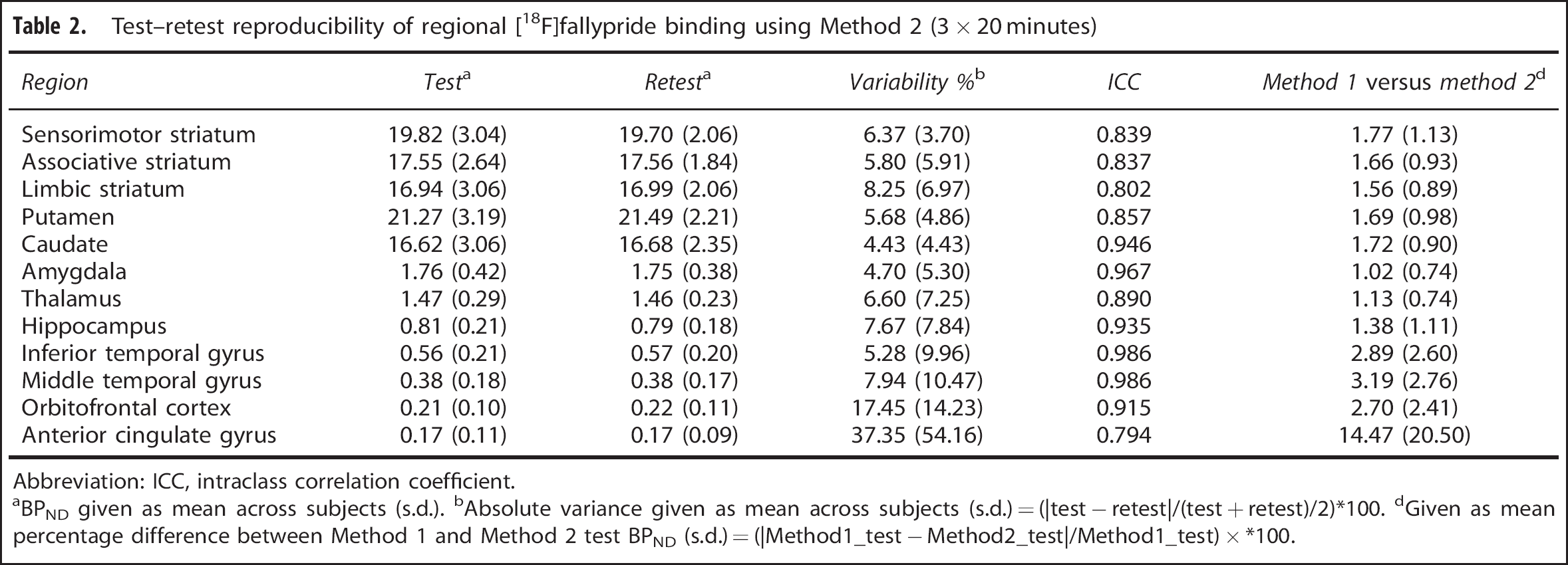
Abbreviation: ICC, intraclass correlation coefficient.
BPND given as mean across subjects (s.d.).
Absolute variance given as mean across subjects (s.d.) = (|test - retest|/(test + retest)/2)*100.
Given as mean percentage difference between Method 1 and Method 2 test BPND (s.d.) = (|Method1_test - Method2_test|/Method1_test) x *100.
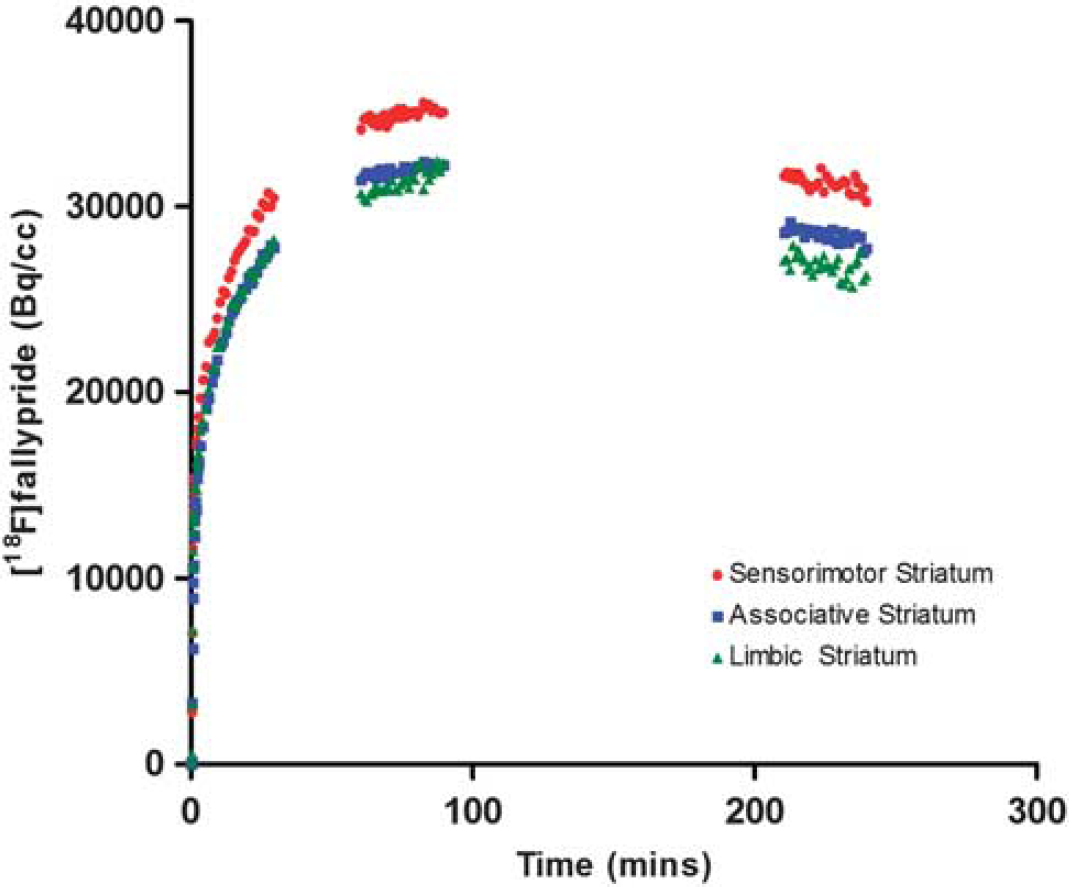
Time-activity curves (Method 1) are shown for the striatal functional subdivisions and represent [ 18 F]fallypride uptake in a single participant.
Power Analysis
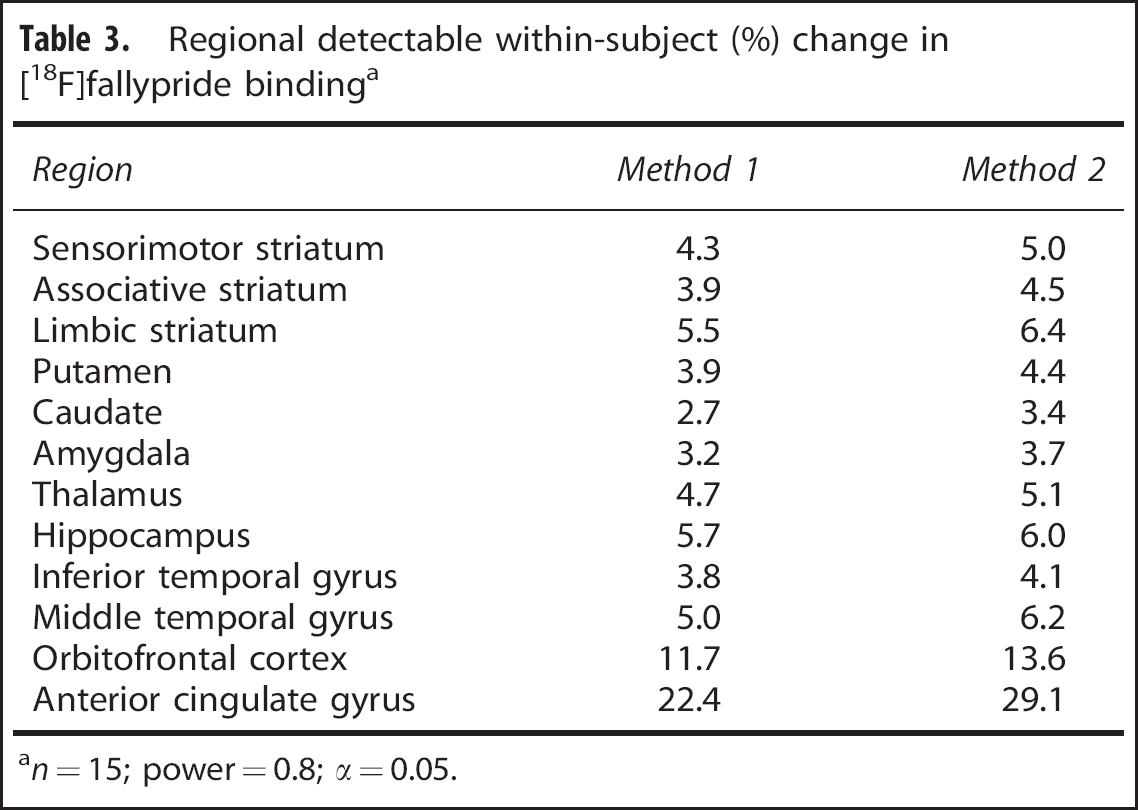
The results of a power analysis for a within-subject study design and a sample size of 15 (paired t-test; α0.05, power = 0.8) are shown in Table 3. This indicates that method 1 would be sufficiently sensitive to detect changes of 5% or less in all regions apart from the limbic striatum (5.5%), hippocampus (5.7%), orbitofrontal cortex (11.7%), and anterior cingulate gyrus (22.4%). Method 2 could detect changes of 5% or less across the caudate, putamen, dorsal striatal subdivisions, inferior temporal gyrus, and amygdala; and larger changes in the other regions.
DISCUSSION
This study has shown high reproducibility and reliability of an adapted [
18
F]fallypride protocol across the striatum, consistent with previous test-retest studies on [
18
F]fallypride in young adults, which have used full modeling with arterial sampling
6
or a simplified reference tissue approach
23
to image analysis. [
18
F]fallypride BPND was also highly reproducible in the amygdala, temporal cortex, thalamus, and hippocampus, comparable with previous data on [
18
F]fallypride.6,23 In contrast, reproducibility in prefrontal regions was poor, particularly in the anterior cingulate cortex, where a higher mean and wider range of variability was observed compared with the other regions sampled. These findings are consistent but more marked than those of Cropley
A [ 18 F]fallypride imaging technique that requires only brief periods in the scanner could significantly enhance the translational potential of [ 18 F]fallypride imaging across a range of neuropsychiatric disorders in which dopamine has been implicated, including patients with dementia, Parkinson's disease, movement disorders, and disorders of impulsivity. Our primary interest in adapting [ 18 F]fallypride imaging was to develop a technique suitable for use in D2/3 receptor occupancy studies in older and/or cognitively impaired patients. Older people are extremely susceptible to antipsychotic side effects, including extrapyramidal symptoms, falls, sedation, and increased cerebrovascular mortality.33,34 The potential mechanisms underpinning this heightened sensitivity are poorly understood, although several theories have been proposed, including alterations in central pharmacokinetics and reduced D2/3 receptor reserve in the ageing brain. 35 It has been suggested that the ‘therapeutic window’ of striatal D2/3 receptor occupancy may be lower in older people, 36 but this has not been tested robustly using a within-subject approach, nor has it been extended to extrastriatal regions, such as the temporal cortex, that have been implicated in treatment response in young psychotic adults. 9
Our adapted protocol is sufficiently sensitive to detect small percentage changes in all but the prefrontal regions, and is therefore a suitable approach to establish the relative contribution of limbic versus striatal occupancy in elderly patients during antipsychotic treatment. This includes patients with schizophrenia-like illness, who are prescribed very low doses (1/10th of the dose used in young adults) of antipsychotic medication 33 and in whom a relatively low regional receptor D2/3 receptor occupancy might be anticipated. The fact that the length of individual scanning times can be reduced to 20 minutes without significantly compromising reliability increases its feasibility for use in patients with dementia. It could be argued that patients with cognitive or neurological impairment are likely to have more variable data than healthy older participants and that longer scanning sessions may be necessary to obtain data of sufficient quality. However, we anticipate that shorter sessions will maximize patient cooperation and reduce head movement confounds. The next stage of our research will be to pilot the protocol as a pretreatment (baseline) protocol in people with dementia who are about to begin antipsychotic medication, both to assess tolerability and the quality of the data collected over 30-versus 20-minute sampling times. We also aim to adapt and optimize an interrupted scanning protocol, which will be suitable for use post antipsychotic treatment, as occupancy by antipsychotic medication will reduce the number of available D2/3 receptor sites and shorten the time taken to achieve equilibrium, particularly within striatal regions.16,18 Similar considerations will need to be taken into account when adapting the protocol for other types of pharmacological interventions, which may alter tracer kinetics and affect times of peak uptake and washout.
The decision not to use MRI data for coregistration with PET images was based on our previous experience of imaging older participants, particularly those with cognitive impairment, 37 in whom a multiple scan approach is more challenging and tolerance for confined spaces is generally poor. As an alternative, regions that were predefined on an atlas were warped to participants’ PET images using a [ 18 F]fallypride template and an automated procedure. This method is similar to the approach previously used to quantify [ 11 C] Raclopride BPND in people with Alzheimer's disease 27 and has the advantage of removing any subjectivity in the placing of ROIs. However, the fact that the templates originated from structural and functional imaging data on healthy young adults could have impacted upon the warping process. Although high tracer signal forms the key component of the process, the accuracy of warping, particularly in smaller, noisier regions, may have been reduced. Partial volume effects, particularly relevant in an older sample, 38 are also likely to have affected the accuracy of tracer quantification. These factors are likely to have contributed to the high test-retest variability in the anterior cingulate gyrus. However, the method of image analysis does not appear to have affected the pattern of reproducibility across other brain regions, as our findings are consistent with previously conducted test–retest studies that used the participant's MRI 23 or PET-MR coregistered images 6 to define ROI. A further consideration is the fact that the sampling times used to quantify cortical and striatal BPND were based upon [ 18 F]fallypride studies carried out in young adults. Given that time to achieve peak tracer binding is dependent upon receptor density, and may be affected by age-related factors including peripheral clearance, regional cerebral blood flow, and blood brain barrier transport, it remains possible that the adapted protocol did not optimally capture the peak in all participants. These methodological limitations are less important for within-subject study designs, but will need to be addressed to maximize the potential of the protocol for use in between-subject comparisons, or to correlate regional BPND with behavioral measures.
In addition to receptor occupancy, we wanted to establish the sensitivity of our protocol to detect changes in endogenous dopamine after pharmacological or behavioral intervention. Amphetamine displacement studies carried out in young adults have found that [ 18 F]fallypride is less sensitive to changes in cortical dopamine levels than other high-affinity tracers such as [ 11 C]FLB457, because of its relatively low signal to noise ratio in these regions. 39 A sufficiently robust effect has, however, been demonstrated across striatal and limbic (hippocampal and amygdala) regions.12,19,23 A power calculation, using a standard sample size of 15 (previous studies have included 10-25 subjects),12,13,15,19,39 indicates that our adapted protocol will be sufficiently sensitive to detect within-subject changes between 2.7% and 5.5% within striatal and limbic regions using method 1, and between 3.4% and 6.4% using method 2. As discussed earlier, we have not yet established whether these findings will generalize to cognitively or neurologically impaired populations, and this issue is particularly relevant for studies that aim to quantify endogenous dopamine release, where small changes in BPND are anticipated. Given the fact that sensitivity to detect within-subject change is crucial for studies of this type, it may be advisable to collect data over the longer (30 minute) sampling times used in method 1 to image endogenous neurotransmission.
We have successfully adapted [ 18 F]fallypride imaging, using an interrupted scanning protocol that considerably shortens scanning times. The high reproducibility and reliability of this protocol means that it could be applied not only to D2/3 receptor occupancy studies but also to image endogenous neurotransmission in striatal and limbic regions. Future work will aim to pilot the protocol in clinically relevant populations and to refine the image analysis method to maximize its potential for use in between-subject study designs.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.