
Abstract
Collateral circulation provides an alternative route for blood flow to reach ischemic tissue during a stroke. Blood flow through the cerebral collaterals is a critical predictor of clinical prognosis after stroke and response to recanalization, but data on collateral dynamics and collateral therapeutics are lacking. Here, we investigate the efficacy of a novel approach to collateral blood flow augmentation to increase collateral circulation by optically recording blood flow in leptomeningeal collaterals in a clinically relevant model of ischemic stroke. Using high-resolution laser speckle contrast imaging (LSCI) during thromboembolic middle cerebral artery occlusion (MCAo), we demonstrate that transiently diverting blood flow from peripheral circulation towards the brain via intra-aortic catheter and balloon induces persistent increases in blood flow through anastomoses between the anterior and middle cerebral arteries. Increased collateral flow restores blood flow in the distal middle cerebral artery segments to baseline levels during aortic occlusion and persists for over 1 hour after removal of the aortic balloon. Given the importance of collateral circulation in predicting stroke outcome and response to treatment, and the potential of collateral flow augmentation as an adjuvant or stand-alone therapy for acute ischemic stroke, this data provide support for further development and translation of collateral therapeutics including transient aortic occlusion.
Keywords
INTRODUCTION
Focal brain ischemia resulting from occlusion of a cerebral blood vessel induces cell death, whose rate and reversibility varies with the degree of preserved blood flow. While blood flow below 20% of baseline in the core of the stroke leads to rapid, irreversible cell death, ‘penumbral’ brain tissue surrounding the core exhibits partially maintained blood flow and delayed cell death. 1 Treatments that restore blood flow to the penumbral tissue can therefore reduce neuronal damage and improve outcome. For example, recanalization with intravenous recombinant tissue plasminogen activator (tPA) significantly reduces mortality and disability associated with ischemic stroke when administered within 4.5 hours of symptom onset.2, 3 Unfortunately, relatively few patients are treated with recombinant tissue plasminogen activator and it remains ineffective in the majority of patients treated within its therapeutic window. 4
Collateral Circulation and Collateral Therapeutics
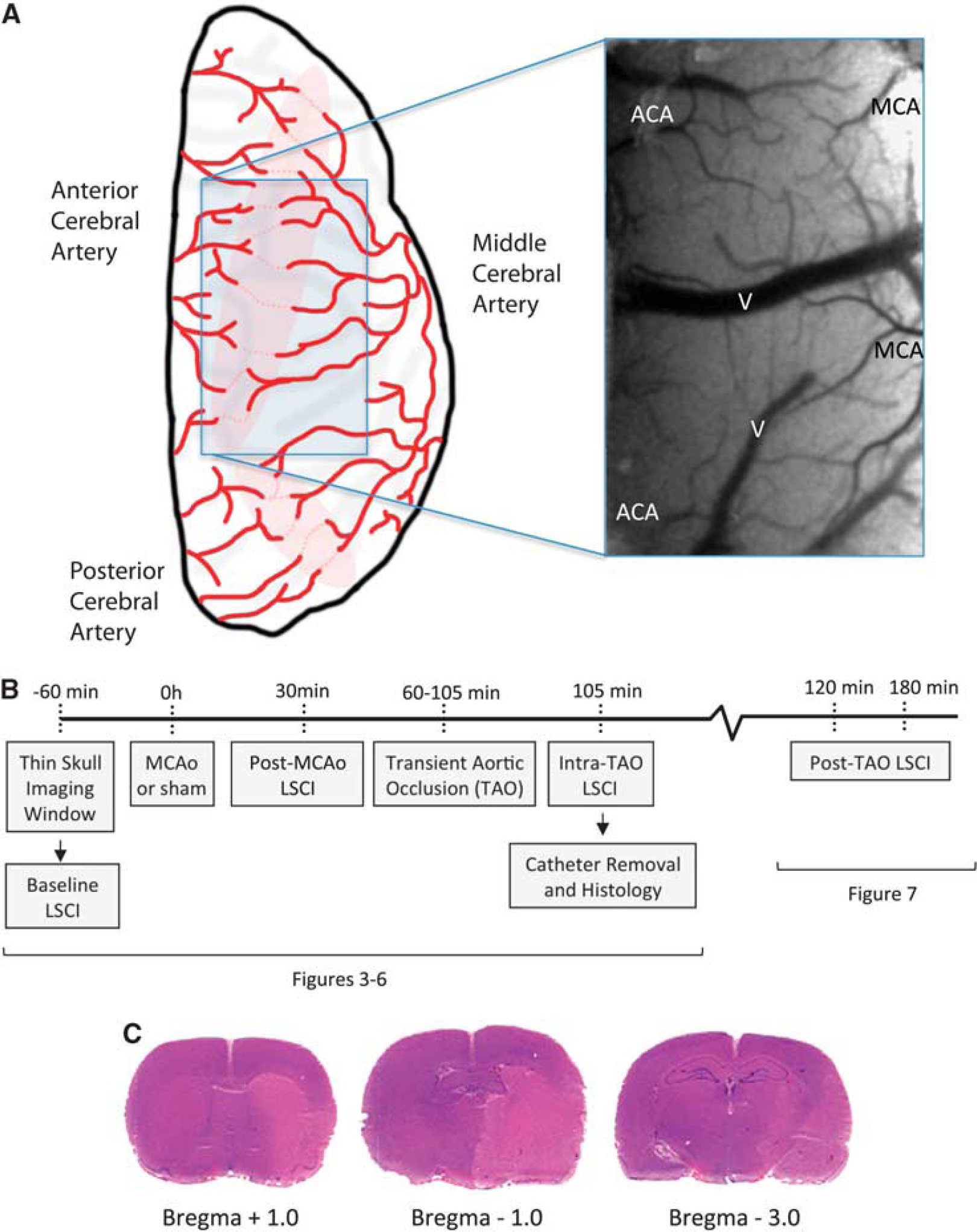
Partially maintained blood flow in the penumbral tissue during stroke is primarily due to the collateral circulatory pathways in the brain. Collateral circulation refers to auxiliary vascular pathways that allow for partial perfusion of ischemic tissue after primary vascular routes are blocked, such as during focal ischemic stroke.5, 6, 7 Leptomeningeal collaterals (or pial collaterals) form anastomotic connections between the distal branches of the cerebral surface arteries. These small arteriolar anastomoses (∼50 to 400 μm) facilitate blood flow from the territory of an unobstructed artery into the territory of an occluded artery.5, 6 In the case of occlusion of the middle cerebral artery (MCA), the most common cause of focal ischemic stroke, anastomotic connections between distal segments of the MCA, and the anterior and posterior cerebral arteries (ACA) can partially maintain perfusion in the ischemic MCA territory (Figure 1).5, 6, 8, 9 Although human stroke patients exhibit significant variability in the size, extent, and retrograde filling time of leptomeningeal collaterals, 9 it has been shown that ischemic patients with better angiographically assessed collateral scores have smaller infarction volumes and lower modified Rankin scale scores at discharge.10, 11 Moreover, patients with good collateral grades have reduced hemorrhagic transformation and better recanalization rates after endovascular recanalization therapy.12, 13
(
‘Collateral therapeutics' harness these endogenous vascular redundancies to improve perfusion of the penumbral tissue during acute ischemic stroke. By increasing perfusion of ischemic tissue, collateral flow augmentation may reduce cell death, increase delivery of thrombolytic agents to both sides of the clot, and potentiate the efficacy of other neuroprotective strategies by increasing drug delivery to ischemic tissues. However, although a number of collateral therapies have been suggested, they remain largely under developed and concrete demonstrations of enhanced collateral blood flow during stroke are rare. Recently, promising preclinical and clinical data support the use of transient aortic occlusion (TAO) to increase global cerebral perfusion and reduce damage due to stroke. Preclinical work in rats has demonstrated reduced infarct size in treated rats 24 hours after thromboembolic MCA occlusion (MCAo). 14 Clinically, data from the SENTIS trials suggest that TAO is safe and may improve stroke outcome in subsets of patients.6, 14, 15, 16, 17, 18 However, important mechanistic data demonstrating the efficacy with which TAO increases leptomeningeal collateral circulation is lacking. Here, we use high-resolution LSCI to conclusively demonstrate augmentation of collateral flow through ACA–MCA anastomoses during TAO in a clinically relevant rodent model of MCAo. Our data suggest TAO can restore blood flow in distal MCA branches to near baseline levels and that enhanced collateral flow persists after treatment cessation. This direct demonstration of enhanced leptomeningeal collateral flow provides support for the use of collateral therapeutics including TAO during acute ischemic stroke.
MATERIALS AND METHODS
Experimental protocols conform to the guidelines established by the Canadian Council on Animal Care and were approved by the Health Sciences Animal Care and Use Committee at University of Alberta. Briefly, male Sprague–Dawley rats (400 to 550 g, n=38) were divided into four treatment groups (MCAo+TAO, n=10; MCAo+sham TAO, n=5; sham MCAo+sham TAO, n=5; sham MCAo+TAO, n=5) before laser speckle contrast imaging (LSCI) through a thinned-skull imaging window (Figures 1A and B). Repeated LSCI was performed such that maps of blood flow were acquired at baseline, postMCAo (or sham), and during or after 45 minutes of TAO (or sham). Throughout surgery and imaging, rats were anesthetized with 1.5% to 2.0% isoflurane (30:70, O2:N20). Temperature was maintained at 37oC, and heart rate, oxygen saturation, and breath rate were monitored at the forepaw contralateral to the ischemic hemisphere using a MouseOx pulse oximeter (STARR, Oakmont, PA, USA; Life Sciences). In addition to LSCI experiments, separate cohorts of rats were used to validate diameter measurements (n=5) or to measure blood pressure changes above and below aortic occlusion (n=8).
Thin-Skull Imaging Window
Before imaging, an ∼5 × 5-mm section of the skull over the distal regions of the right MCA territory corresponding the right sensorimotor cortex (spanning 1 to 5 mm lateral to midline and centered at bregma, see Figure 1A) was thinned until translucent using a dental drill. HEPES-buffered artificial cerebrospinal fluid was frequently flushed over the skull while thinning it to dissipate any excess heat generation. The thinned skull was smoothed with a rounded scalpel (Surgistar, Knoxville, TN, USA; #6400), covered with a thin layer of 1.3% low-melt agarose (in HEPES-buffered artificial cerebrospinal fluid), and sealed with a coverslip. 8
Laser Speckle Contrast Imaging and Analysis
Rats were placed in a custom stereotaxic plate under a Dalsa 1M60 Pantera camera mounted on a video macroscope with a tandem lens configuration (× 1.7 magnification). A total of 300 to 500 images of back-scattered laser light were collected at 20 Hz (15-illisecond exposure time) during illumination of the imaging window with a 784 nm (32 mW) laser (StockerYale, Salem, NH, USA). Analysis of laser speckle images was performed using ImageJ software (NIH, Bethesda, MD, USA). The speckle contrast factor K is defined as the ratio of the standard deviation to the mean intensity (K=σs/I) in a small (5 × 5 pixels) region of the speckle image. K has a minimal value of 0 when the scattering particles are moving quickly, a maximal value of 1 with no movement, and is inversely related to blood flow velocity.8, 19, 20 Maps of the speckle contrast value at each pixel of the image show the pattern of blood flow on the cortical surface during imaging, with darker vessels demonstrating relatively faster blood flow than lighter vessels. The mean speckle contrast values in large diameter surface veins and branches of the MCA were calculated by measuring the average speckle contrast in 2 to 8 equidistant regions of interest within the vessel borders. 8 The mean areas of regions of interest in MCA segments and surface veins were 132.2±12.8 and 538.0±40.9 pixels, 2 respectively. To provide a better estimate of relative changes in blood flow velocity, speckle contrast values were converted to correlation times (τc) that are, in theory, inversely and linearly proportional to blood flow velocity (i.e. 1/τc is proportional to the velocity of the blood flow at the ROI where speckle contrast was measured). 21 However, the assertion that correlation times are inversely proportional to blood flow is based on simplifying assumptions derived from literature using other imaging modalities and may not hold under all imaging and blood flow conditions. 20 We have therefore focused on within animal comparisons of changes in blood flow (as indicated by correlation times) as opposed to quantitative determinations of blood flow velocity.
The relationship between speckle contrast, K, and τc is given by

where T is the exposure time of the camera. Relative changes in blood flow are illustrated by calculating the ratio of baseline (preMCAo) τc to the τc of a particular imaging session (τBaseline /τc). τ Baseline /τ c values are equivalent to 1/τc normalized to baseline, with a value of 1 for baseline measures, and values at later imaging sessions demonstrating change from baseline (e.g. a vessel that had a 20% increase in blood flow velocity after MCAo that persisted at 45 minutes would have τ Baseline /τ c values of 1, 1.2, and 1.2 for the pre-stroke, poststroke, and 45-minute time points).
Changes in vessel diameter for cortical surface veins and branches of the MCA downstream of anastomoses were determined using an ImageJ plug-in that uses a full-width at half-maximum algorithm to estimate the inner vessel diameter. 22 Here, diameters were measured from vessels defined by LSCI maps of blood flow at anatomically distinct regions of the vessels that could be clearly identified across imaging sessions. Only vessels that were apparent in all imaging sessions were measured (i.e. vessels that were not carrying blood poststroke but reperfused during treatment were excluded because reliable estimates of postMCAo diameter could not be attained). In two animals (from the MCAo+TAO group), venous flow in poststroke imaging was too low to reliably determine vessel diameter from LSCI maps, and these animals were therefore excluded from venous diameter change analyses.
To better estimate the change in blood flow through MCA segments, incorporating both changes in blood flow velocity and blood vessel diameter, measures of relative blood flow (relQ) were calculated. An estimate of flow rate (Q) in a circular vessel can be estimated using the formula

where r is the mean radius of the vessel and v is the velocity of blood flow. Here, we approximated the relative blood flow in MCA segments downstream of anastomoses using the formula

where r n is the mean radius of the MCA segments in a given animal normalized to the baseline radius for that animal (i.e. baseline r n =1 and τ Baseline / τ c =1, such that for all animals, baseline relQ=π). relQ values were normalized to baseline within animals and averaged to give an index of blood flow relative to baseline.
Permanent Middle Cerebral Artery Occlusion
Thromboembolic MCAo was induced as previously described.8, 14 In brief, a 1.5-cm longitudinal incision was made along the midline of the ventral cervical skin. The distal portion of the ECA was ligated and cut. A modified PE-10 catheter filled with bovine thrombin was inserted into the right ECA and blood was withdrawn and allowed to clot for 15 minutes. Once the clot formed, the catheter was advanced 17 mm in the ICA until it reached the origin of the MCA. The clot was injected into the MCA, the catheter removed, and the wound closed.
Transient Aortic Occlusion
To transiently occlude the descending aorta, 14 a dilation catheter (2.0mm diameter, Cordis, Bridgewater, NJ, USA; Fire Star RXPTCA) was advanced past the origin of the renal artery from either the exposed iliac (intra-occlusion imaging, Figures 3 and 4) or femoral (postocclusion imaging, Figure 7) arteries. Aortic flow diversion was initiated 30 to 60 minutes after onset of the thromboembolic MCAo and maintained for 45 minutes. Proper placement of the catheter was verified postmortem in intra-occlusion imaging groups. The final images were acquired during either the 45th minute of aortic occlusion or after removal of the dilation catheter.
Blood Pressure Measurement During Transient Aortic Occlusion
To monitor arterial blood pressure above and below the aortic occlusion, blood pressure was measured in the carotid and ventral tail arteries in non-ischemic rats (n=8). Arteries were isolated under isoflurane anesthesia and cannulated with a silicone catheter containing 500 IU/ml heparinized saline. Access to the carotid was achieved through the ECA as described above, with the catheter advanced out of the ECA into the common carotid towards the heart. Blood pressure was measured before TAO, during 45 minutes of TAO, and immediately after TAO using a PressureMAT monitor (PendoTECH, Princeton, NJ, USA).
Two-Photon Blood Flow Imaging
To validate surface vessel diameter values derived from LSCI data, these values were compared against diameter measurements from the same vessels imaged during in vivo two-photon microscopy through a cranial window preparation (performed as described in detail elsewhere).23, 24 Briefly, a section of the skull over the right MCA territory was thinned until translucent using a dental drill then gently removed. The cranial window was covered with a thin layer of 1.3% low-melt agarose (in brain buffer), and sealed with a coverslip. 8 Fluorescein isothiocyanate–dextran (70,000 MW, Sigma-Aldrich, Edmonton, Alberta, Canada) was injected via the lateral tail vein (0.3 Ml, 5% (w/v) in saline). In vivo microscopy was performed using a Leica SP5 MP two-photon laser scanning microscope and Coherent Chameleon Vision II pulse laser tuned to 800 nm. Z-stacks through the first 200 μm of cortical tissue were acquired through the cranial window using a 1.0 N.A. × 20 water dipping objective (Leica HCX APO), and vessel diameter measurements were made from maximum intensity projections of these stacks.
Statistical Analysis
Data are displayed as mean±s.e.m. Repeated measures analysis of variance were used to determine main effects of treatment on LSCI-derived measures of blood flow and vessel diameter for all groups. Means at each time point were compared with means from all other time points within each treatment group using Tukey's honestly significant difference (where three time points were compared, Figures 2C–G and Figures 6F, G, and I) and Sidak multiple comparison tests (where two time points were compared, Figures 5B, and 5C and Figure 6H). Statistical significance was defined as P<0.05.
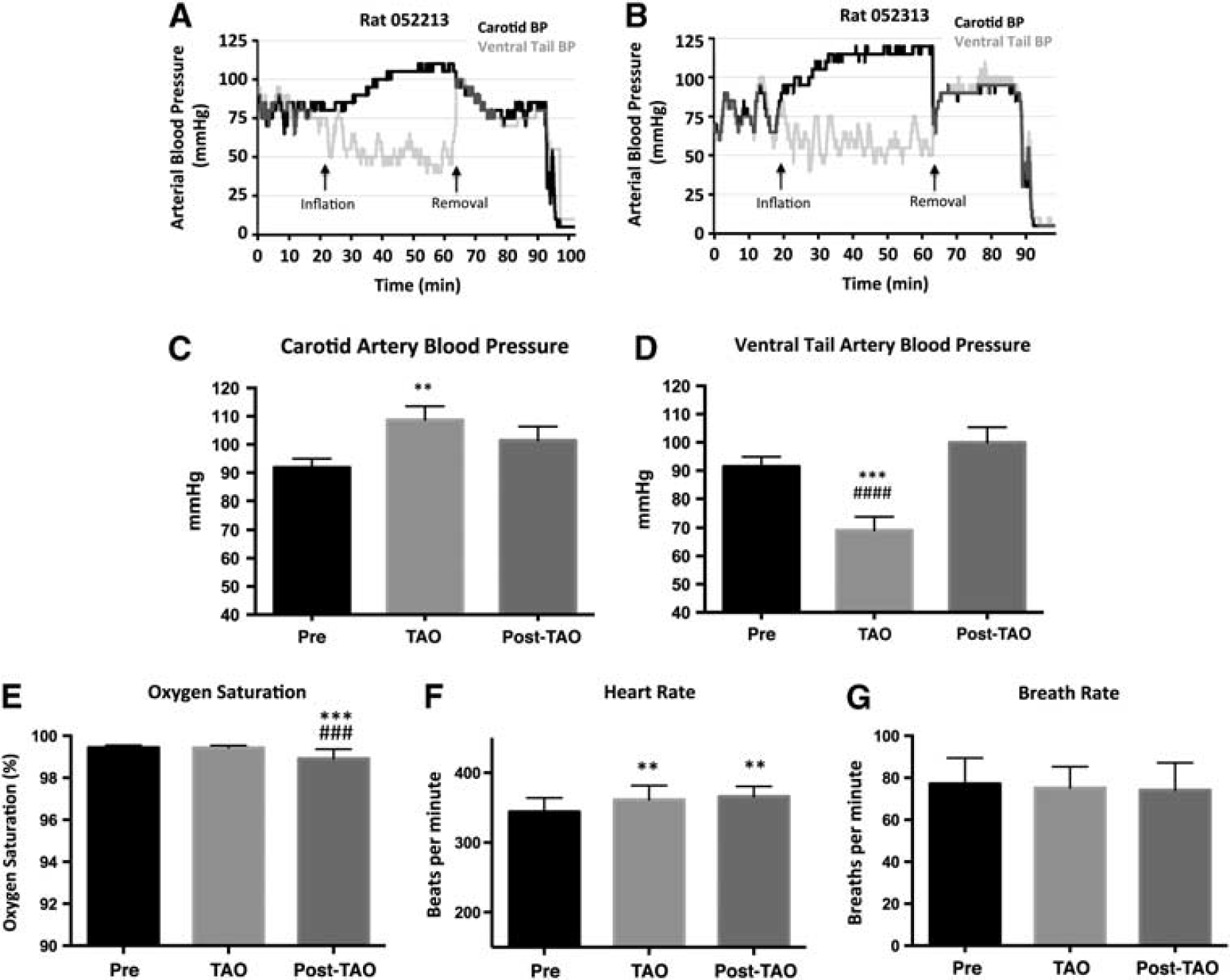
Systemic effects of transient aortic occlusion (TAO). (
Histology
Immediately after the final imaging session, anesthetized animals were killed and their brains removed. To confirm early infarcts were consistent with previous studies, early indices of infarct size and location were assessed in a subset of rats (n=6, 3 each from treated and untreated MCAo groups) on cryostat sectioned 20 μm coronal brain sections stained with hematoxylin and eosin (Figure 1C).
RESULTS
Systemic Effects of Transient Aortic Occlusion
Transient aortic occlusion increases blood volume above the occlusion and is thought to increase cerebral blood flow. To monitor arterial blood pressure above and below the aortic occlusion, blood pressure was measured in the carotid artery and ventral tail artery in non-ischemic rats (n=8). As illustrated in representative animals in Figures 2A and B, TAO induced a gradual increase in arterial pressure above the occlusion, with a corresponding decrease in blood pressure below the occlusion. Mean blood pressure before, during, and after TAO are illustrated in Figures 2C and D. Transient aortic occlusion significantly altered blood pressure in the carotid and ventral tail arteries (repeated measures analysis of variance, F(2.000, 14.00)=8.054, P=0.0047 and F(2.000, 14.00)=28.21, P<0.0001, respectively). Specifically, blood pressure in the internal carotid artery was significantly greater during TAO than during baseline, whereas ventral tail artery pressure was significantly reduced during TAO relative to baseline and postocclusion values (Figures 2C and D). A trend for increased blood pressure in the carotid artery after TAO was observed but did not reach significance. Physiologic parameters remained largely stable during TAO, with a small but significant decrease in oxygen saturation after TAO and a small increase in heart rate during and after TAO (Figures 2E–G).
Laser Speckle Contrast Imaging of Collateral Blood Flow
Based on the blurring of laser speckle patterns by the motion of blood cells, LSCI can be used to produce high-spatiotemporal resolution images of blood flow in vasculature on the cortical surface. Here, by positioning a thin-skull imaging window over the distal segments of the ACA and MCA (Figure 1A), LSCI was used to monitor the blood flow in individual surface vessels downstream of a MCAo and thereby assess changes in leptomeningeal collateral flow due to MCAo treatment with TAO. Laser speckle contrast imaging maps of blood flow were acquired immediately before and after MCAo (or sham surgery), then again during the 45th minute of TAO or after removal of the intra-aortic catheter (or sham treatment). As shown in Figure 3, the maps of blood flow attained via LSCI in sham-MCAo animals were highly consistent over imaging sessions, irrespective of TAO or sham treatment. Importantly, these animals did not exhibit anastomotic connections between the distal segments of the ACA and MCA. Conversely, MCAo induced clear changes in blood flow downstream of the occlusion (Figure 4). Immediately after MCAo, robust anastomotic connections between distal segments of the ACA and MCA (Figure 4, arrows in middle panels) were observed in all animals. These leptomeningeal anastomoses remained stable during postMCAo imaging sessions in sham- and TAO-treated animals, as all ACA–MCA anastomoses identified immediately postMCAo persisted until the final imaging session 45 minutes after sham treatment.
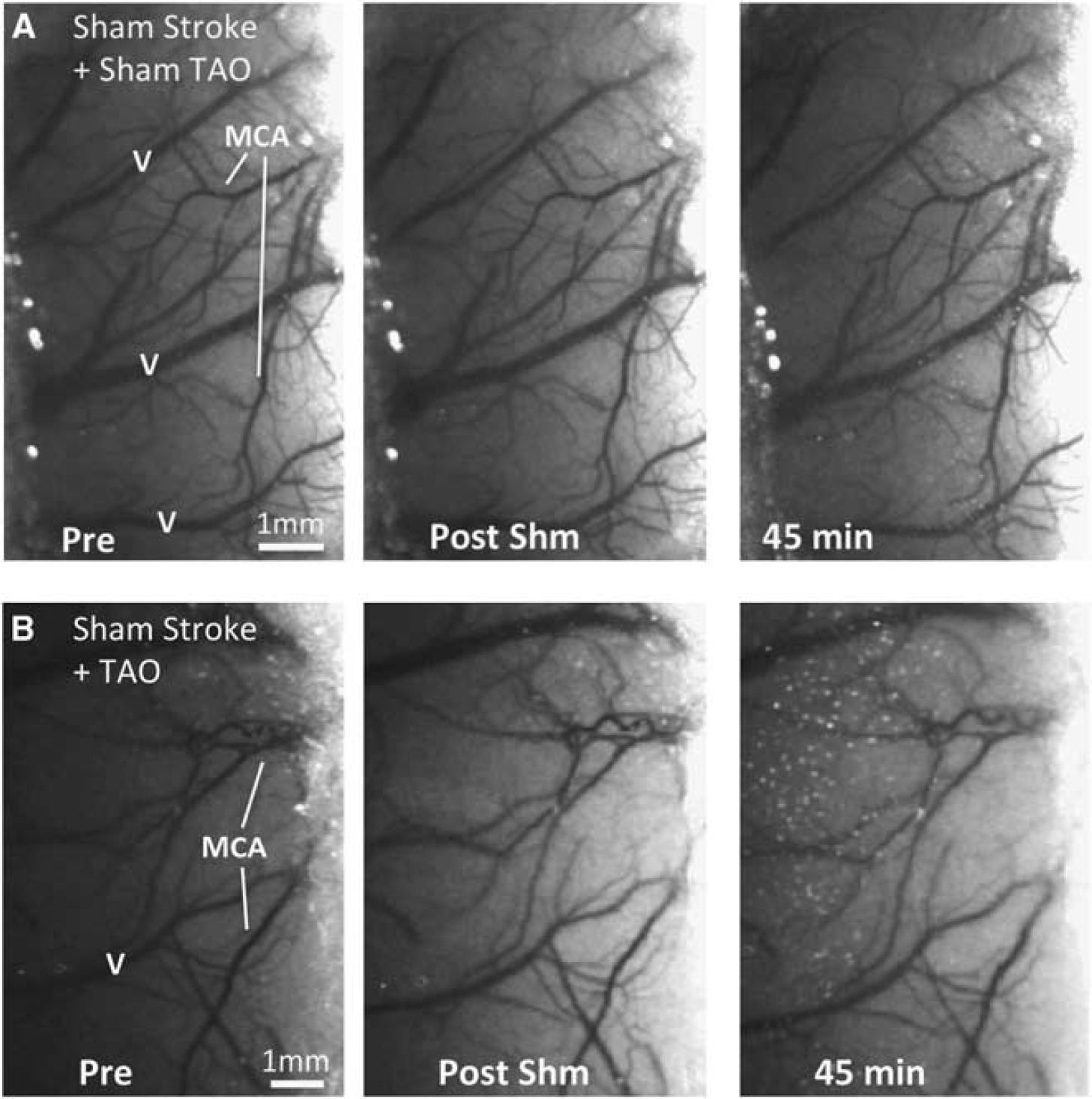
Laser speckle contrast imaging (LSCI) maps of blood flow in animals with sham middle cerebral artery occlusion (sham-MCAo). Laser speckle contrast imaging-derived maps of blood flow were stable throughout all imaging sessions in sham-MCAo animals in both sham-treated rats (
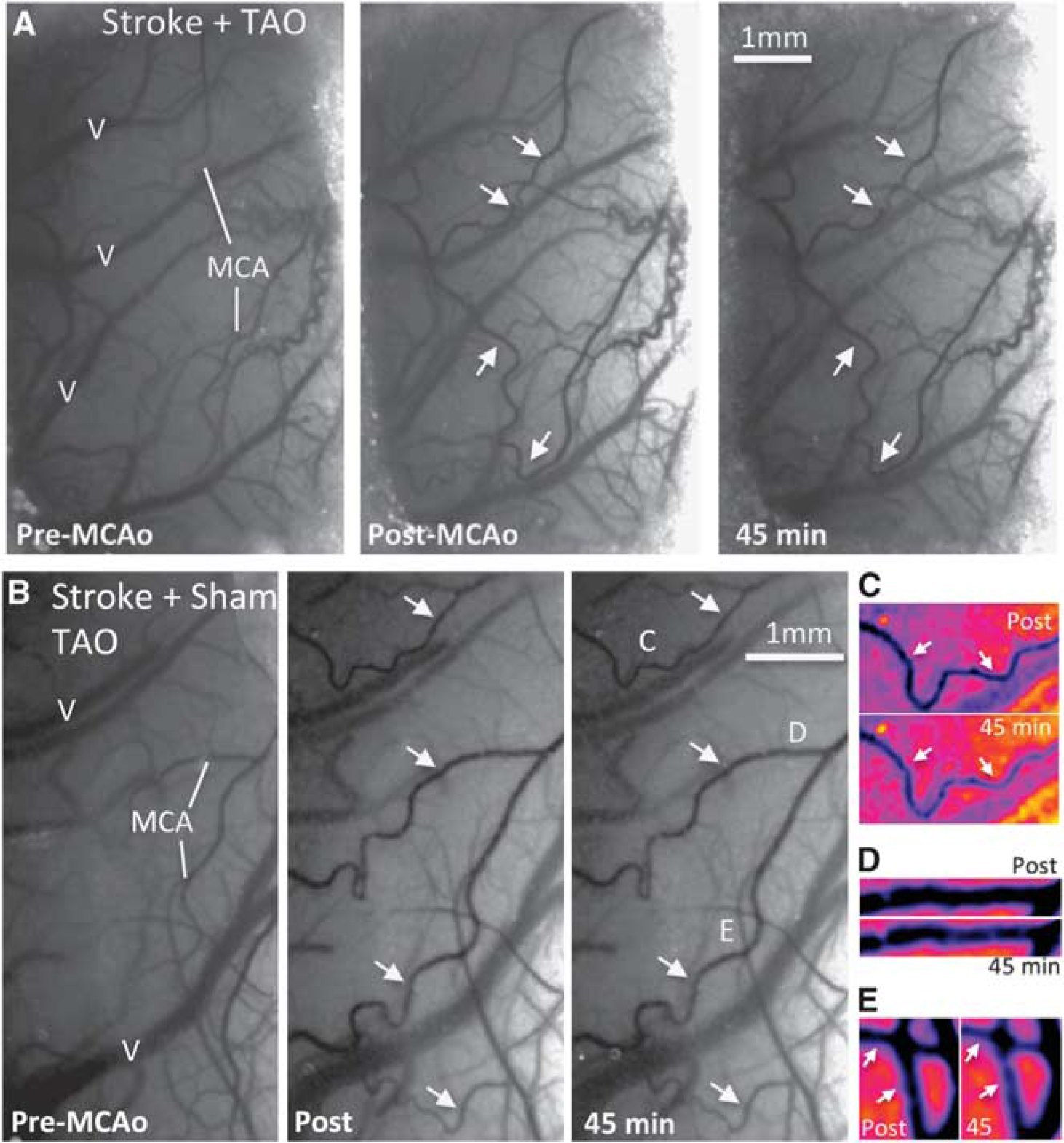
Laser speckle contrast imaging (LSCI) maps of blood flow in rats after middle cerebral artery occlusion (MCAo) and transient aortic occlusion (TAO). (
Characterization of Blood Flow Changes and Vessel Diameter After Middle Cerebral Artery Occlusion and Transient Aortic Occlusion
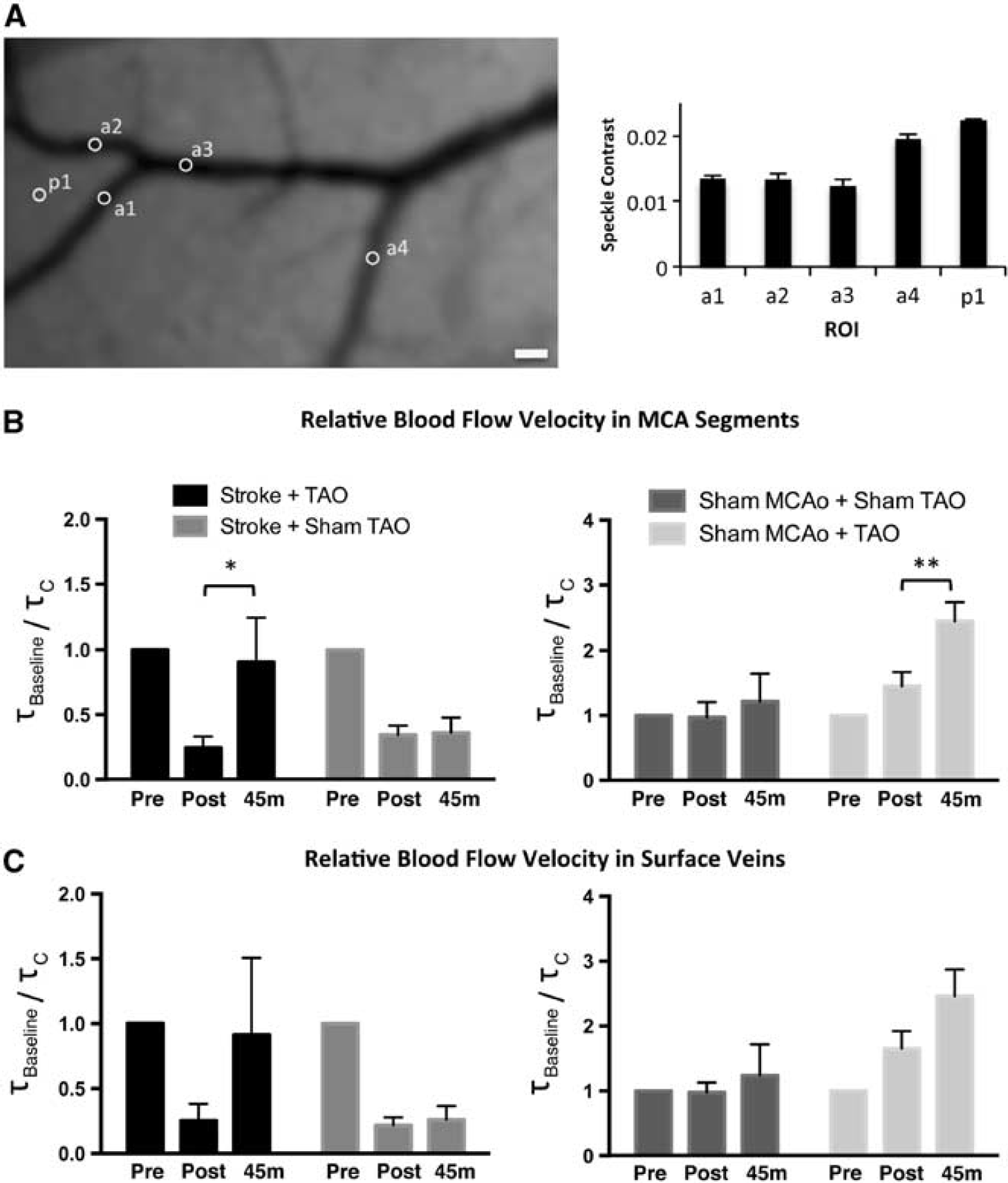
Repeated measure analysis of the correlation times (τc) derived from speckle contrast measurements in MCA segments (e.g. Figure 5A) identified a significant main effect of treatment group on τc in both TAO-treated and sham-TAO rats after MCAo (MCAo+TAO, F(2, 10)=5.891, P=0.0204; MCAo+Sham-TAO, F(2, 8)=7.525, P=0.0145) but not sham-MCAo. Notably, post hoc comparisons demonstrated that τc remain significantly greater than baseline (reflecting decreased blood flow velocity) in these MCA segments at all time points after stroke in sham-TAO rats (all P <0.05), where as TAO returned τc to baseline levels (Baseline versus postMCAo, P <0.05; baseline versus 4 minutes, P>0.05; postMCAo versus 45 minutes, P<0.05).
Elevated blood flow velocity during transient aortic occlusion (TAO) treatment of middle cerebral artery occlusion (MCAo). (
To more directly illustrate blood flow velocity changes due to TAO, τbaseline/τc ratios (Figures 5B and C) were calculated within animals. Because τc are inversely proportional to blood flow velocity, these ratios illustrate blood flow velocity relative to baseline in postMCAo (or sham-MCAo) and postTAO (or sham-TAO) imaging sessions. Two-way repeated measures analysis of variance confirmed a significant main effect of both treatment group (F(3–17)=9.708, P=0.0006) and time (F(1,17)=17.32, P=0.0007) on τbaseline/τc ratios calculated postMCAo (or sham) and postTAO (or sham) in MCA segments, and a significant interaction between treatment group and time (F(3,17)=3.484, P=0.0389). Sidak's multiple comparisons revealed significant increases in blood flow during the 45th minute of TAO in these MCA branches in both MCAo and sham-MCAo groups (Figure 5B). Significant main effects of treatment group and time were also observed for surface veins (Figure 5C, treatment group, F(3,17)=7.280, P=0.0024; time, F(1,17)=5.543, P=0.0308), although Sidak's post hoc comparisons within groups did not reach significance.
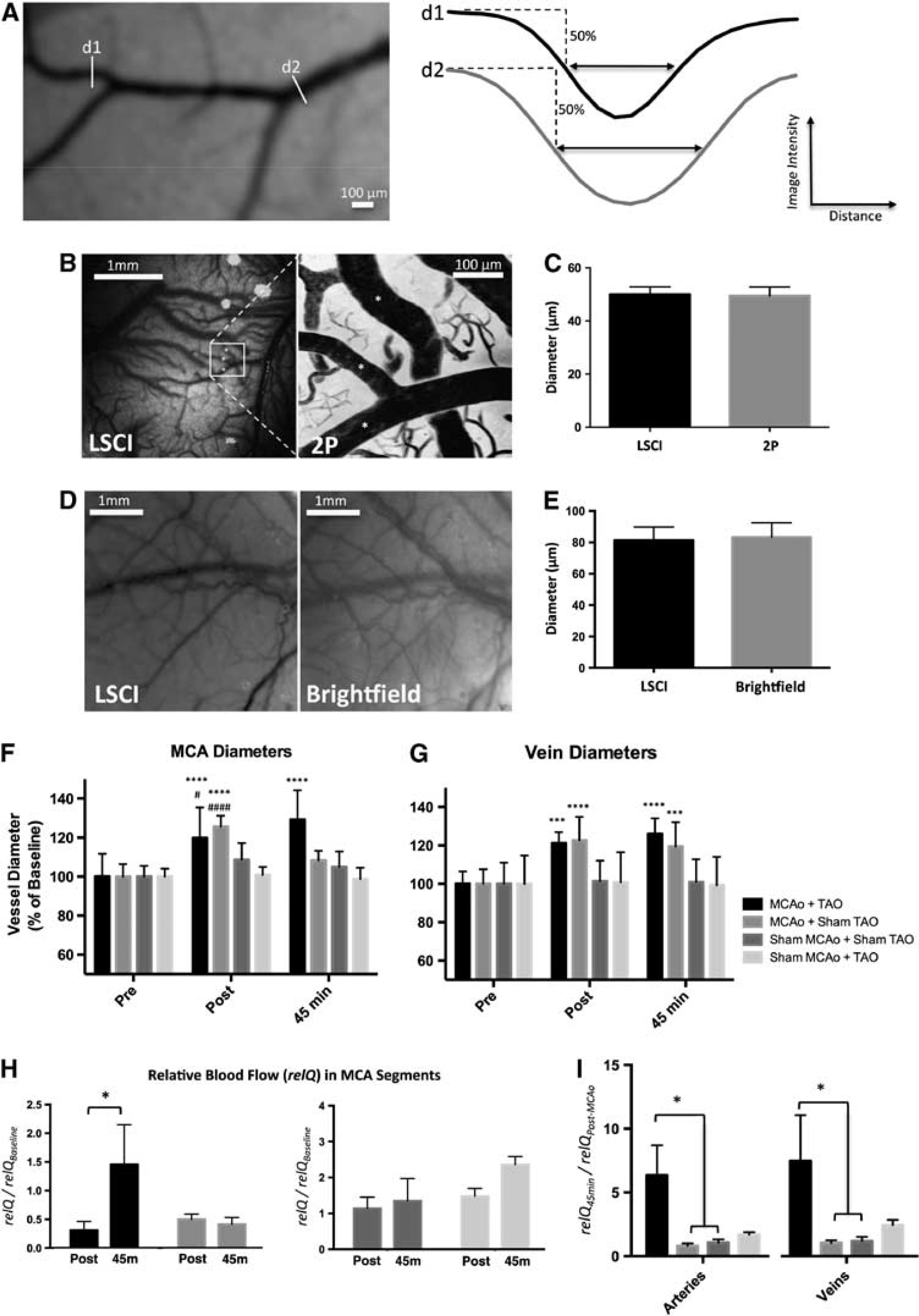
Measurements of the diameter of the surface vessels were made using an ImageJ (NIH) plug-in that uses a width at half-maximum algorithm to determine vessel diameter. 22 Diameter measurements were made orthogonal to the direction of flow in MCA segments and surface veins in anatomically distinct regions that could be unambiguously identified between imaging sessions (Figure 6A). Laser speckle contrast imaging diameter measurements were validated (using the same ImageJ plug-in) against vessel diameter measurements from surface veins and arteries identified in images acquired during two-photon blood flow imaging (Figures 6B and C, see Materials and Methods) and measurements of large surface vessels visible through the thinned skull under brightfield illumination (Figures 6D and E). Diameter measurements from LSCI were highly consistent with measures from two-photon (Figure 6C, t-test, P=0.667) or brightfield (Figure 6E, P=0.619) images. Two-way repeated measures analysis of variances of vessel diameter in surface vasculature revealed significant main effect of time in MCAo segments (F(2,32)=31.91, P<0.0001) and surface veins (F(2,30)=15.53, P<0.0001), and a significant interaction between treatment group and time (MCA segments, F(6,32)=10.91, P<0.0001; surface veins, F(6,30)=4.952, P=0.0013). Tukey's honestly significant difference post hoc comparisons demonstrated that vessel diameters significantly increased in MCA segments downstream of ACA–MCA anastomoses after MCAo but not sham-MCAo (Figure 6F). Mean MCA segment diameter remained significantly greater than baseline and postMCAo values during the 45th minute of TAO (Figure 6F). Conversely, MCA diameters during the 45th minute of sham-TAO with MCAo were significantly smaller than postMCAo values and not significantly different from baseline (Figure 6F, see also Figures 4C–E). In surface veins (Figure 6G), vessel diameters were significantly greater than baseline in both treated and untreated rats immediately after MCAo and during the 45th minutes of TAO or sham-TAO. Sham-MCAo rats did not show any significant changes in vessel diameter in either the TAO or sham-TAO groups.
Effect of transient aortic occlusion (TAO) on vessel diameter and blood flow during middle cerebral artery occlusion (MCAo). (
A comparison of MCAo rats treated with TAO versus sham-TAO suggests that TAO increases blood flow velocity and blood vessel diameter in MCA segments. To better estimate the change in blood flow through MCA segments due to TAO, incorporating both blood flow velocity and diameter changes, we calculated the relative blood flow (relQ, see Materials and Methods) during TAO (or sham) relative to postMCAo (or sham). Analysis of relQ across treatment groups (Figure 6H) revealed a significant main effect of treatment group (F(3, 16)=3.506, P=0.0399) and time (F(1, 16)=9.926, P=0.0062), and Sidak's post hoc comparisons confirmed a significant increase in blood flow (relQ) during TAO in the MCAo+TAO group. Notably, in the MCAo+TAO group, blood flow (relQ) during TAO was 6.34±2.37 fold greater than postMCAo blood flow (Figure 6I), whereas blood flow (relQ) in the MCAo+Sham-TAO was reduced at 45 minutes relative to postMCAo values (0.81±0.21-fold change). A similar effect was observed in venous relQ (Figure 6I), where relQ values during TAO were 8.89±4.25-fold greater than postMCAo relQ.
Persistent Changes in Collateral Blood Flow after Transient Aortic Occlusion
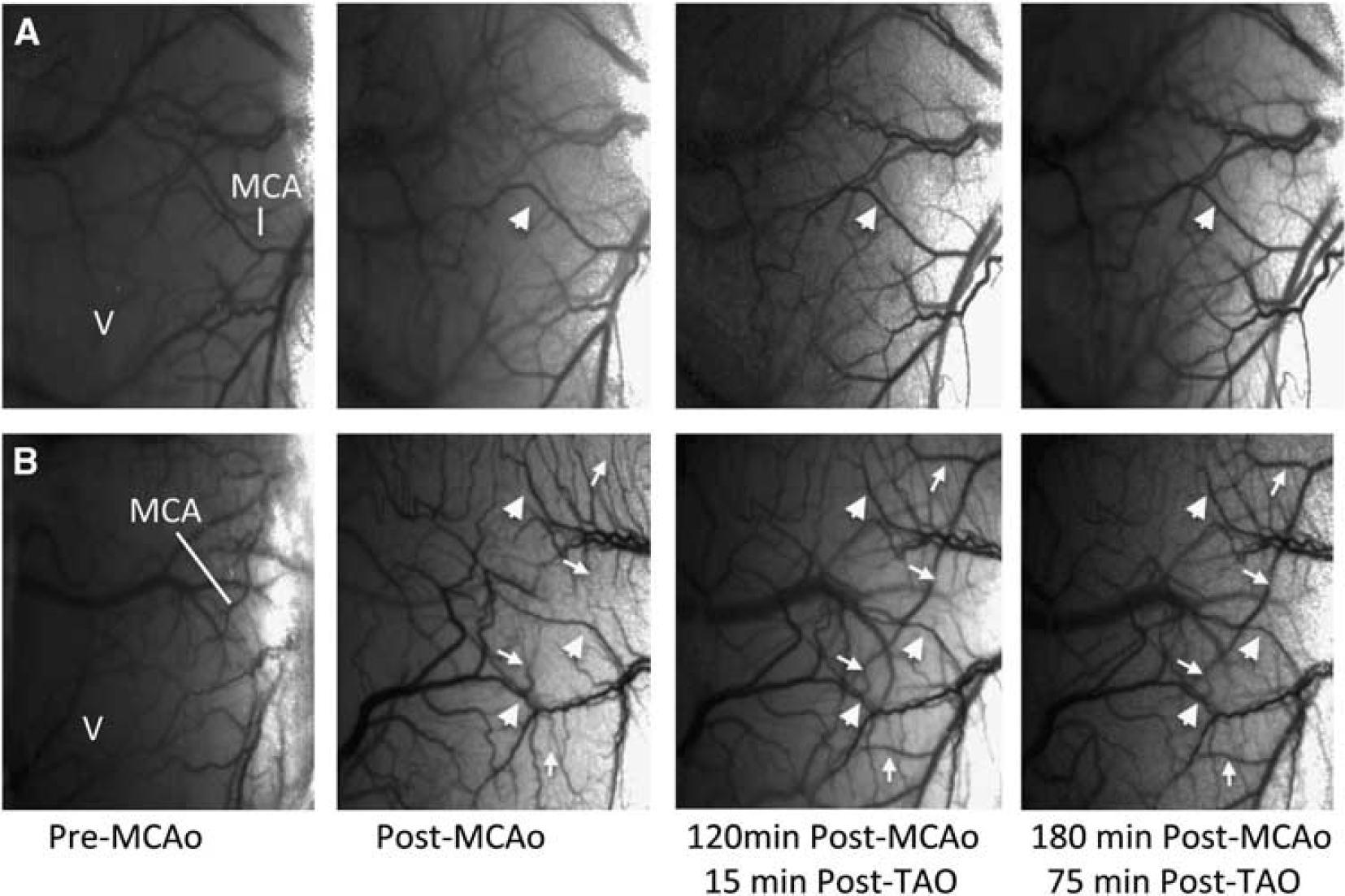
Laser speckle contrast imaging data described above demonstrate a significant increase in blood flow and vessel diameter in MCA segments downstream to ACA–MCA anastomoses during TAO. In five animals, TAO-induced changes were imaged 75 minutes after removal of the aortic catheter and balloon. Laser speckle contrast imaging maps demonstrated that enhanced collateral blood flow persisted through all imaging sessions in four of five rats (Figure 7A, large arrow), with two rats exhibiting a restoration of blood flow in MCA segments that were not carrying blood after MCAo that persisted after catheter removal (e.g. Figure 7B, small arrows). Middle cerebral artery occlusion+TAO induced persistent increases in blood flow, as relQ values calculated from MCA segments identified in images acquired 75 minutes after catheter and balloon removal were 3.30±1.33-fold greater than postMCAo values. Notably, this likely underestimates persistent TAO-induced changes in flow, as vessels that reperfused only after treatment were not included in these calculations because reliable measures of vessel diameter were not possible before reperfusion.
Persistent changes in blood flow after transient aortic occlusion (TAO). (
Histology
Laser speckle contrast imaging maps of collateral blood flow provided conclusive evidence of MCAo. Nonetheless, to confirm ischemic damage due to thromboembolic MCAo consistent with our previous studies 8 , histologic assessment of early infarct was performed on a subset of rats from imaging experiments (n=6). Hematoxylin and eosin staining (Figure 1C) demonstrated early indications of infarct in both TAO-treated and untreated MCAo rats (n=3 from each TAO and sham treatment groups). Infarcts included regions of the striatum and/or overlying sensorimotor cortex ipsilateral to the occlusion, with a mean volume of 81.3±17.0 mm3. While neuroprotective efficacy was not a focus of this study, a trend towards smaller early infarct in rats treated with TAO versus sham (61.6±27.0 mm3 versus 100.9±18.1 mm3, respectively) was observed in this small subset of animals.
DISCUSSION
Despite the promise of collateral therapeutics, concrete demonstrations of enhanced blood flow in leptomeningeal collaterals remain rare. Our data show that TAO induced a significant increase in blood pressure in the carotid artery. This increased cerebral perfusion pressure would be predicted to enhance leptomeningeal collateral blood flow during MCAo, an effect that was confirmed using high-resolution LSCI that demonstrated persistent increases in blood flow downstream of ACA–MCA anastomoses after MCAo treated with TAO. Our data show that TAO restored blood flow in MCA segments downstream of leptomeningeal anastomoses to baseline levels and maintained stroke-induced vasodilation in these MCA segments (whereas vessel diameters in sham-treated rats returned to baseline within 45 minutes). Moreover, we show that enhanced collateral blood flow persisted for at least 75 minutes after removal of the aortic catheter and balloon. These persistent increases in cerebral blood flow agree with previous studies in a non-ischemic porcine model. 25 Persistence of enhanced cerebral flow may result from a trend towards elevated systemic blood pressure after TAO (as observed in some rats, Figure 2B and C). Alternatively, TAO may trigger transient vasodilation via circulating vasoactive factors initiated by peripheral ischemia, as has been observed after remote ischemic conditioning in patients with subarachnoid hemorrhage. 26 Combined, our data demonstrate the potency with which TAO can augment collateral flow to ischemic tissue and support further preclinical and clinical investigation.
Although LSCI permits sensitive mapping of blood flow in surface vessels and measurement of relative changes in blood flow over time, it should be noted that the precise quantification of blood flow velocity is difficult because the exact relationship between speckle contrast and blood flow velocity remains undefined. 27 The demonstration that correlation times are inversely proportional to blood flow is rooted in a number of simplifying assumptions based on literature from other imaging modalities and may not hold under all imaging and blood flow conditions. 20 Recent developments in LSCI image acquisition and analysis can improve quantitative accuracy,20, 28, 29, 30, 31 though at this point, LSCI remains a powerful but only semi-quantitative modality best restricted to describing relative changes in blood flow within animals rather than a quantitative measure of blood flow velocity. As such, our analyses focused on within animal effects of MCAo and TAO on collateral blood flow. We demonstrate that in rats receiving a thromboembolic MCAo, TAO restored blood flow to near baseline levels in MCA segments downstream of leptomeningeal collaterals. Our measures of vessel diameter derived from LSCI data highlight a novel mechanism for improved flow during TAO (prevention of collateral collapse during ischemia) in addition to enhanced global cerebral perfusion. Our determination of vessel diameter from LSCI maps is novel and was validated by comparison against images acquired during brightfield illumination and two-photon microscopy. Although our validation experiments were performed in non-ischemic animals, measurements were made from a variety of vessel diameters and types, including large surface veins and arteries as well as small surface arterioles and venules. Blood flow velocity will vary from <1 mm/s in smaller vessels to >10 mm/second in larger vessels in rats. As such, the accuracy of LSCI diameters across different vessel types and sizes would suggest that they are reliable across a broad range of physiologic velocities. Moreover, robust vasodilation of surface arterioles has been reported previously after MCAo,32, 33 and our LSCI measures agree well with these previous studies. Our approximations of relative blood flow (relQ) incorporating TAO induced changes in blood flow velocity and vessel diameter highlight the efficacy with which TAO enhances blood flow through leptomeningeal anastomoses during MCAo. Future studies using techniques permitting resolution below the cortical surface, such as two-photon microscopy, 34 will be important to extend these findings and determine the degree of enhanced perfusion in penetrating arterioles and at the neurovascular interface below the cortical surface.
Comparison with Previous Studies of Collateral Therapeutics
Although several avenues for collateral blood flow augmentation have been suggested, including volume expansion, mild induced hypertension, administration of vasodilators, and stimulation of the sphenopalatine ganglion, preclinical and clinical data in support of these methods are variable.6, 7 Collateral augmentation with volume expansion has been evaluated in acute stroke with variable results in clinical trials. 5 Mild induced hypertension has proven effective in preclinical trials, as increased collateral blood flow and neuroprotection has been observed after induced hypertension in rodent models of ischemia. 35 Preliminary clinical data have suggested a benefit for induced hypertension, with reports identifying improvements in perfusion pressure, NIHSS scores and volume of hypoperfused tissue with only a small increase in intracranial pressure, that may be particularly useful for patients ineligible for thrombolysis.36, 37, 38, 39 However, clinical trials have not demonstrated unequivocal beneficial results in neurologic outcome after stroke. 6 Moreover, the risks of induced hypertension in stroke populations remain undefined, and systemic hypertensive treatments may increase the risk of intracerebral hemorrhage, reflex bradycardia, and ischemic bowel disease. 40 Vasodilation using inhaled nitric oxide has recently shown promise in reducing brain damage in traumatic brain injury and ischemic stroke in preclinical studies.41, 42 Notably, studies in animal models suggested that inhaled nitric oxide selectively dilated arterioles in the ischemic penumbra during MCAo, thereby increasing collateral blood flow and significantly reducing ischemic brain damage. 42 Similarly, promising preclinical studies of electrical stimulation of the sphenopalatine ganglion, the source of parasympathetic innervation of the anterior cerebral circulation, suggest increased ipsilateral blood flow and reduced damage in stroke models, results that have prompted preliminary clinical studies of this approach.43, 44, 45
Recent preclinical and clinical evidence supports the use of TAO to direct blood flow to the brain during ischemic stroke and thereby reduce brain damage. Studies in a non-stroke porcine model suggest that TAO can increase cerebral blood flow by over 30%. 25 Neuroprotective efficacy was demonstrated in a recent study in rats that found that TAO for 1 hour resulted in reductions in infarct volume comparable with tPA without increasing hemorrhagic transformation or damaging the blood–brain barrier. 14 Notably, the combination of flow augmentation with tPA had an additive neuroprotective effect. 14 Clinically, TAO has been proven safe alone and after tPA administration.4, 16, 18 In the SENTIS trial, 515 patients with cortical ischemic stroke received 45 minutes of aortic occlusion or standard stroke treatment. Transient aortic occlusion met primary safety endpoints but failed to reach the primary efficacy endpoint. 16 No difference in serious adverse events was found between TAO-treated stroke patients and controls: TAO did not increase the risk of intracerebral hemorrhage and no significant differences in renal, cardiovascular, pulmonary, gastrointestinal, or vascular events were observed. These data suggest that TAO (associated with hypertension only above the aortic occlusion) may have an improved safety profile relative to induced (systemic) hypertension. Moreover, the utility of induced hypertension in normotensive patients is unclear, and it has been suggested that the benefits of TAO are not simply because of increased blood volume or hypertension above the occlusion. Partial aortic occlusion redistributes blood volume into the upper body, which manifests as an increase in central venous pressure. 46 Pranevicius et al. 46 suggest that this increase in venous pressure recruits the collapsed vascular network and eliminates cerebral venous steal, thereby improving perfusion of ischemic tissue. Notably, data from the SENTIS trial demonstrates that TAO significantly improved outcomes in patients that received early treatment (<5 hours from onset), patients with moderately severe stroke (NIHSS 7 to 15) and patients over the age of 70 years.15, 16, 17 Interestingly, older treated patients were two times more likely than controls to benefit from treatment.15, 16, 17 Our data extend this existing preclinical and clinical data and conclusively demonstrate that TAO is a potent approach for enhancing collateral flow (via leptomeningeal anastomoses) to ischemic tissue after MCAo. Transient aortic occlusion therefore offers exciting potential as both a stand-alone neuroprotective strategy and an adjunct therapy to improve efficacy of other treatments during acute ischemic stroke. In particular, combining TAO with tPA (to enhance thrombolysis) or with vasodilators such as inhaled nitric oxide (to increase flow through dilated vasculature) offer exciting potential as combination therapies.
Footnotes
Ashfaq Shuaib is a member of an advisory committee to CoAxia Inc. The remaining authors declare no conflict of interest.