
Abstract
In moyamoya disease (MMD), surgical revascularization may be complicated with postoperative hyperperfusion. We analyzed cerebral perfusion and metabolism using positron emission tomography (PET) or single-photon emission computed tomography (SPECT) before and after bypass surgery on 42 sides of 34 adult patients with MMD. In seven cases (16.7%) with symptomatic hyperperfusion, diagnosed by qualitative 123I-iodoamphetamine (IMP) SPECT, a subsequent PET study during postoperative subacute stages revealed significantly increased cerebral blood flow (CBF) from 34.1 ± 8.2 to 74.3 ± 12.8 mL/100 g per minute (
Introduction
The causes of moyamoya disease (MMD), characterized by progressive stenosis/occlusion of the terminal internal cerebral artery and its branches, are unclear; ischemic and hemorrhage injuries may be the causes of MMD (Suzuki and Takaku, 1969). Superficial temporal artery (STA)-middle cerebral artery (MCA) anastomosis or various kinds of indirect bypasses are recommended for symptomatic patients based on the degree of hemodynamic compromise (Kuroda and Houkin, 2008; Takahashi and Miyamoto, 2010). Despite favorable long-term outcomes after successful bypass surgery for MMD, increasing evidence suggests that this may be complicated with temporary neurologic deterioration during the postoperative acute stage owing to focal cerebral hyperperfusion around the site of the anastomosis (Fujimura et al, 2007, 2009, 2011; Furuya et al, 2004; Kim et al, 2008; Ogasawara et al, 2005). Postoperative cerebral hyperperfusion is defined as a major increase in ipsilateral cerebral blood flow (CBF) well above the metabolic demands of brain tissue (Piepgras et al, 1988; Sundt et al, 1981), and is well characterized in patients after carotid endarterectomy (CEA). Although a similar cerebral hyperperfusion phenomenon was reported in patients with MMD using single-photon emission computed tomography (SPECT) or xenon-enhanced computed tomography (Fujimura et al, 2007, 2009, 2011; Furuya et al, 2004; Kim et al, 2008; Ogasawara et al, 2005), no previous study has quantitatively analyzed CBF and metabolism of postoperative hyperperfusion in MMD. The purpose of this study was to analyze CBF and metabolism by positron emission tomography (PET) in cases of symptomatic cerebral hyperperfusion, screened by qualitative 123I-iodoamphetamine (123I-IMP) SPECT as previously reported, after STA-MCA anastomosis in patients with MMD. Relative increases and absolute values of CBF in PET during symptomatic hyperperfusion in MMD were compared with those of the traditional definition of post CEA hyperperfusion and the predefined CBF value as normal control + 2 standard deviations (s.d.).
Materials and methods
Patient Population
This study protocol was governed by the guidelines of national government based on the Helsinki Declaration revised in 1983, and it was approved by the Institutional Research and Ethics Committee of our hospital. All study participants provided informed consent in the study. Between April 2009 and June 2011, 34 patients (21 women) with MMD were treated at the Department of Neurosurgery, National Cerebral and Cardiovascular Center, Osaka, Japan; age (mean ± s.d.) was 39.3 ± 15.3 years (range, 15 to 70 years). Pediatric patients were excluded from the study. Diagnosis of MMD was based on cerebral angiography studies according to diagnostic criteria updated in 1997 (Fukui, 1997). Presenting symptoms were cerebral infarction (
Surgical Procedure
All patients were treated by the same surgeons (KI and NN). Under general anesthesia mainly using propofol, the parietal and/or frontal branches of the STA were dissected, and single and/or double anastomosis to supra- and/or infra-Sylvian MCA (M4) was performed in a side-to-end manner. The patency of the anastomoses was intraoperatively confirmed by Doppler ultrasonography and indocyanine green videoangiography.
Diagnosis of Symptomatic and Asymptomatic Hyperperfusion Based on Perioperative Positron Emission Tomography and Single-Photon Emission Computed Tomography Studies
The protocol of the perioperative measurement of CBF with/without metabolism was shown in Figure 1. The PET or
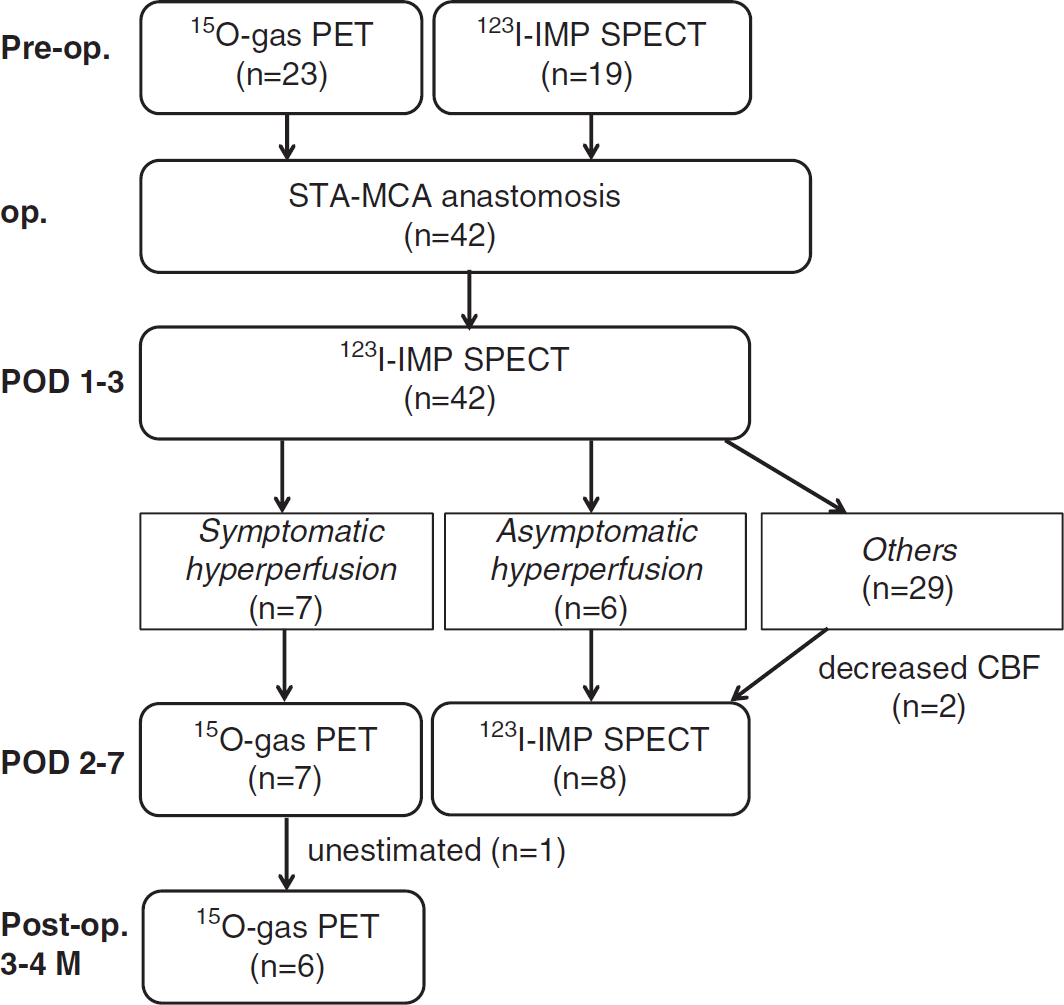
The protocol of the examination. As for screening, 123I-IMP SPECT was conducted first during postoperative day (POD) 1 to 3 for all patients to determine qualitatively the presence of a significant focal increase in cerebral blood flow (CBF) at the site of anastomosis. Then, if patients with hyperperfusion on postoperative 123I-IMP SPECT developed focal neurologic deficits, they underwent the PET study on POD 2 to 7. If patients did not develop new apparent neurologic symptoms despite hyperperfusion on 123I-IMP SPECT, then they were classified as asymptomatic hyperperfusion and repeated the 123I-IMP SPECT study during the subacute stages. Patients with symptomatic hyperperfusion repeated the PET study during the chronic phase 3 to 4 months after surgery. 123I-IMP, 123I-iodoamphetamine; SPECT, single-photon emission computed tomography; PET, positron emission tomography; STA-MCA, superficial temporal artery-middle cerebral artery.
Positron Emission Tomography Measurement
A series of PET scans were performed to quantitatively assess CBF and cerebral metabolic rate of oxygen (CMRO2) at each stage, according to the dual-tracer autoradiographic protocol developed by Kudomi et al (2005) with a minor modification of replacing intravenous administration of 15O-water by 15O-carbondioxide inhalation (Nezu et al, 2012). The PET scanner used was ECAT ACCEL from Siemens-CTI (Knoxville, TN, USA), and data were acquired in the 2D mode. The scan can provide an intrinsic spatial resolution of 4.5 mm full-width at half-maximum at the center of the field-of-view. A catheter was placed in the brachial artery for measurement of arterial input function. After a 10-minute transmission scan using a rotating external 68Ge-68Ga rod source, a PET scan was obtained 3 minutes after inhalation of 15O-labeled carbon monoxide gas (C15O) of 2,500 MBq for 30 seconds. After the 10 minutes allotted for radioactivity decay, an additional dynamic scan was performed for 8 minutes, while 4,000 MBq of oxygen (15O2) and 5,000 MBq of 15O-labeled carbon dioxide (C15O2) were inhaled through a facemask sequentially at 5-minute intervals. The inhalation period was 1 minute for each gas. Arterial blood was continuously withdrawn during this dynamic scan, and the radioactivity concentration of the blood in the catheter tube was monitored using a scintillator block detector system (BeCON; Molecular Imaging Lab Inc., Suita City, Japan) (Kudomi et al, 2003). Arterial blood samples were also taken before and after the dynamic scan, and arterial oxygen content (PO2) and arterial PCO2 were measured.
Control values of PET parameters were obtained from eight patients (six male and two female; mean age ± s.d. = 66.1 ± 9.4 years) who had unilateral stenosis of the internal carotid artery or the trunk of MCA with minimal or no infarction on magnetic resonance imaging. Values of PET parameters obtained from the contralateral MCA region were as follows: CBF, 46.6 ± 5.6 mL/100 g per minute; cerebral blood volume (CBV), 2.90 ± 0.61 mL/100 g; CMRO2, 3.56 ± 0.62 mL/100 g per minute; oxygen extraction fraction (OEF), 0.43 ± 0.05; and CBF/CBV, 18.8 ± 6.8/min. There were no significant changes in these values with advancing age.
Single-Photon Emission Computed Tomography Measurement
Preoperative clinical SPECT studies followed the DTARG protocol, with dual administration of iodoamphetamine (Kim et al, 2006). Briefly, two dynamic scans were acquired in quick succession, with a 2-minute interval between scans. The first scan covered the initial 0- to 28-minute period and the second was acquired from 30 to 58 minutes. At 4 minutes per frame, seven frames covered each of the two dynamic scan periods. 123I-Iodoamphetamine was infused twice over 1 minute into the antecubital vein at 0 and 30 minutes. Acetazolamide (17 mg/kg, 1,000 mg maximum) was administered intravenously 20 minutes after the first iodoamphetamine injection, corresponding to 10 minutes before the second iodoamphetamine injection. Projection data were summed for the acquisition duration of the first and second scans and reconstructed. The SPECT data provide quantitative information on CBF at rest and after an acetazolamide challenge; it provides information about vascular reserve and the severity of hemodynamic brain ischemia. Regional vascular reserve was defined as the ratio of the difference between acetazolamide-activated regional CBF (rCBF) and resting rCBF to resting rCBF: Regional vascular reserve = ((acetazolamide-activated rCBF/resting rCBF–1) × 100(%)). The severity of hemodynamic brain ischemia was classified into three stages as follows: stage 0 (vascular reserve >30%), stage I (30% ≤ vascular reserve ≤ 10% or 80% of normal CBF ≤ resting CBF), and stage II (10% > vascular reserve > −30% and 80% of normal CBF > resting CBF) (JET study Group, 2002). This classification was based on hemodynamic status, determined from PET findings (Powers, 1991). The 123I-IMP autoradiographic method (Iida et al, 1994) was performed postoperatively for all patients. The 123I-IMP autoradiographic method uses a single iodoamphetamine administration to assess CBF at rest. The same image reconstruction process as for the DTARG protocol was used.
Magnetic Resonance Imaging Protocol
The MR imaging was performed using a 1.5-T MR scanner (Symphony, Siemens, Erlangen, Germany) fitted with a circularly polarized head coil. Fast fluid-attenuated inversion recovery MR images were acquired before STA-MCA anastomosis (7 ± 5 days before or after the first PET). Sequence parameters were as follows: repetition time/echo time/number of excitations, 9,000 ms/120 ms/l; inversion time, 2,500 ms; turbo factor, 15; and matrix, 352 × 352. Additional MR scans were also performed on each patient during the hyperperfusion phase (1 ± 2 days before or after the second PET) and the chronic phase (7 ± 5 days before or after the third PET).
Data Analysis
The PET images were reconstructed using a standard filtered-back projection technique on the PET scanner console, which included corrections for a scatter and attenuation. A postreconstruction Gaussian filter of 8 mm full-width at half-maximum was also applied. All PET and MR images were then transferred to an independent PC workstation for further analyses. Functional images for CBF, CMRO2, OEF, and CBV were obtained using an in-house program published previously (Kudomi et al, 2005), with a minor modification in the process of compensating for the recirculation water in the arterial blood (Iida et al, 1993) with automatic separation of two input functions (Kudomi et al, 2009). All PET images were registered to the CBF image taken at the preoperative study using Multimodality Image Registration Software (Dr View, AJS Inc., Tokyo, Japan), which fits six rigid body parameters using a mutual information matching technique. The MR images taken at three different time points were also registered to the CBF image so that all PET and MR images were aligned at the same coordinates. Agreement of the registered images was visually confirmed to match the brain contours between PET and MR images, including the cerebellum, sylvian fissure, and ventricular regions.
Regions-of-interest were carefully selected using QView software from the QSPECT project at National Cerebral and Cardiovascular Center Research Institute (Osaka, Japan) (Iida et al, 2010). For quantitative assessment of CBF, CMRO2, OEF, and CBV using PET in patients with symptomatic hyperperfusion, regions-of-interest were constructed to delineate areas of increased CBF around the site of anastomosis on the postoperative PET during the subacute stage compared with preoperative CBF images on PET/SPECT. Regions-of-interest were then superimposed on other PET and MR images. For the rest of the patients in whom preoperative PET was performed, regions-of-interest, consisting of a 1-cm diameter circle along the cortical rim, avoiding the infarcted area, were manually placed over the frontal cortex (targeted to the central area where anastomosis was planned).
Statistical Analysis
All data are presented as the mean ± s.d. All data were analyzed by analysis of variance. If significance was obtained, then we used Scheffe's criteria for multiple comparison.
Results
Clinical Characteristics
Preoperative hemodynamic status was categorized using PET and SPECT in 23 (9 sides at stage I and 14 sides at stage II) and 19 (9 sides at stage I and 10 sides at stage II) hemispheres in 34 patients, respectively. In the qualitative 123I-IMP SPECT study on POD 1 to 3, a significant focal increase in CBF at the site of anastomosis was observed in 13 sides (31%), whereas decreased CBF was noted in 2 sides (4.8%). Of the patients with hyperperfusion on qualitative 123I-IMP SPECT, seven sides (16.7%) in six patients became symptomatic (symptomatic hyperperfusion) and subsequently underwent the PET study during POD 2 to 7. The rest of the study population were classified as asymptomatic hyperperfusion in 6 sides (14.3%) and others in 29 sides (69%) based on qualitative 123I-IMP SPECT and the appearance of postoperative new neurologic symptoms (the traditional definition of postoperative hyperperfusion in MMD).
Table 1 presents a summary of the cases with symptomatic hyperperfusion. All patients complicated with symptomatic hyperperfusion presented with ischemic attacks. The incidence of symptomatic hyperperfusion was correlated with the degree of preoperative hemodynamic impairment; 5.9% (1 of 18 sides) at stage I and 25.0% (6 of 24 sides) at stage II. Hyperperfusion on the PET scan was observed in the area near the site of STA-MCA anastomosis. Symptoms related to hyperperfusion included seizure, sensory disturbance, and aphasia in three, two, and two cases, respectively. Symptoms occurred on POD 1 to 4, with the duration being 4 to 14 days. The modified Rankin scale score of patients complicated with symptomatic hyperperfusion was 0 or 1 at postoperative months 3 to 4.
Summary of seven cases in six patients with postoperative symptomatic hyperperfusion
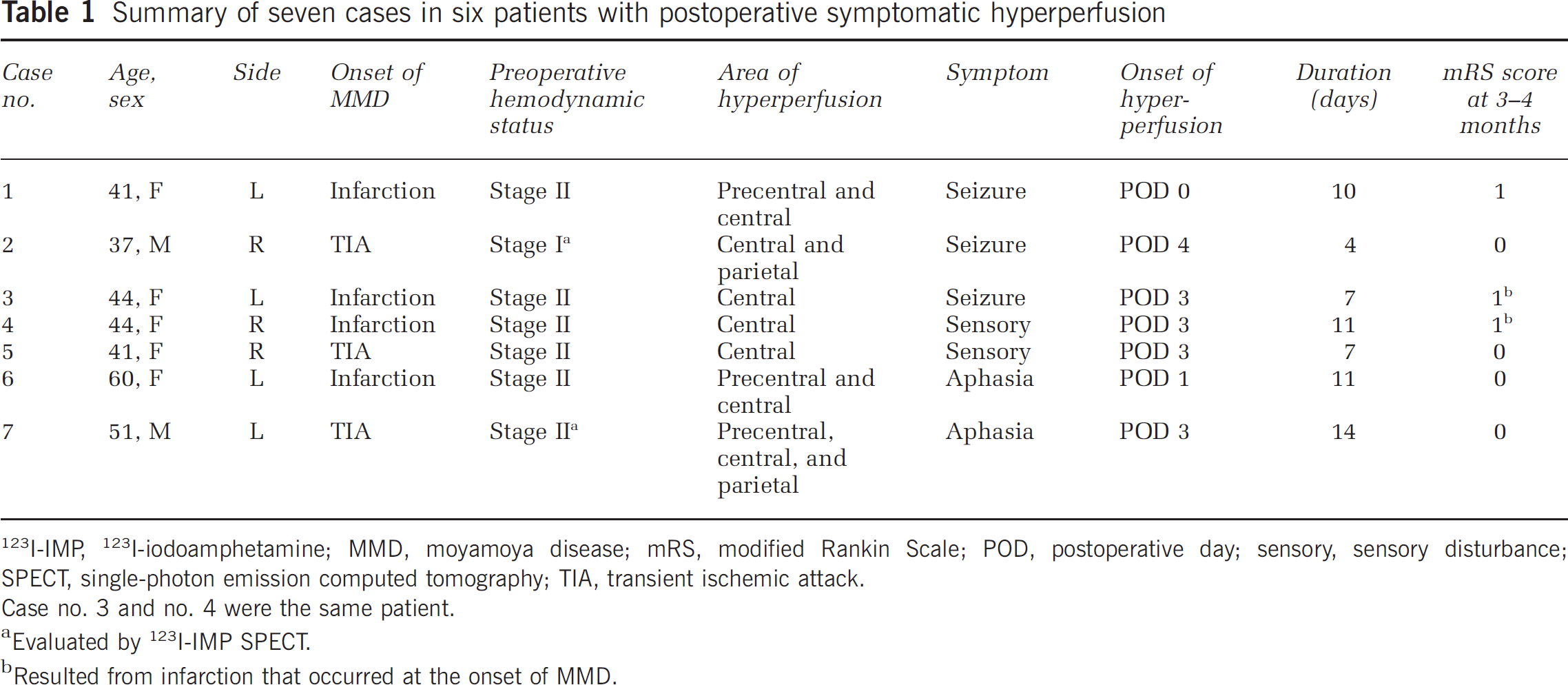
I-IMP, 123I-iodoamphetamine; MMD, moyamoya disease; mRS, modified Rankin Scale; POD, postoperative day; sensory, sensory disturbance; SPECT, single-photon emission computed tomography; TIA, transient ischemic attack.
Case no. 3 and no. 4 were the same patient.
Evaluated by 123I-IMP SPECT.
Resulted from infarction that occurred at the onset of MMD.
Correlation of Preoperative Positron Emission Tomography Parameters with Symptomatic Hyperperfusion
Table 2 presents preoperative PET parameters in 22 hemispheres of 18 patients. One patient with postoperative decreased CBF on qualitative 123I-IMP SPECT was excluded. These hemispheres were divided into symptomatic hyperperfusion (
Preoperative PET parameters in 22 hemispheres of 18 patients
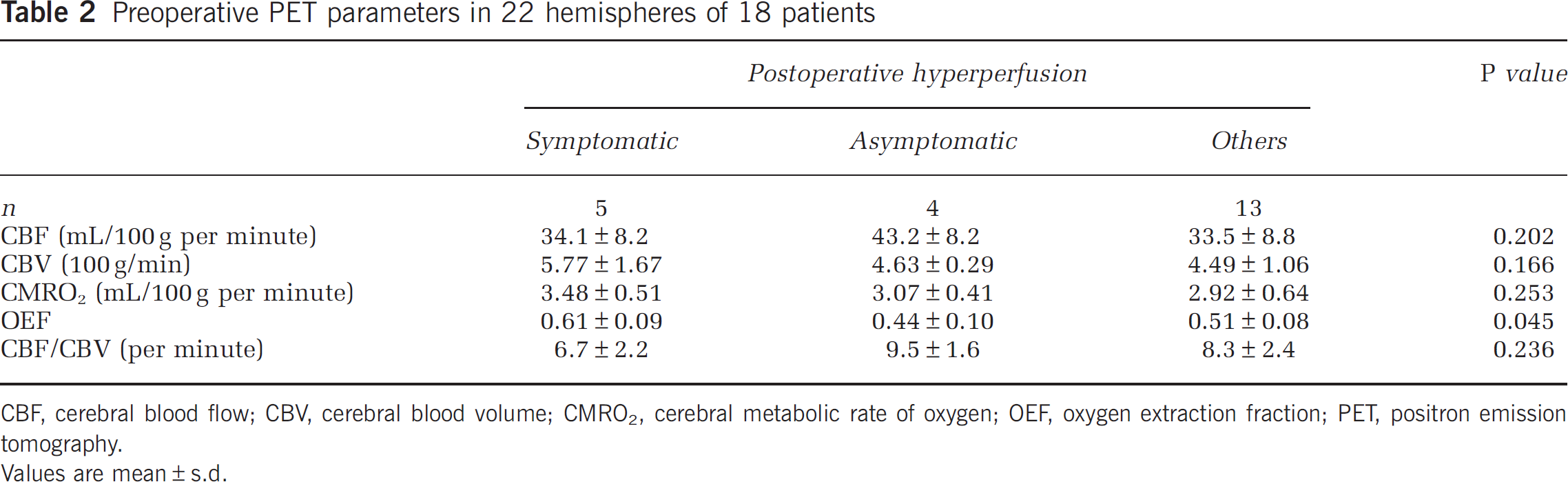
CBF, cerebral blood flow; CBV, cerebral blood volume; CMRO2, cerebral metabolic rate of oxygen; OEF, oxygen extraction fraction; PET, positron emission tomography.
Values are mean±s.d.
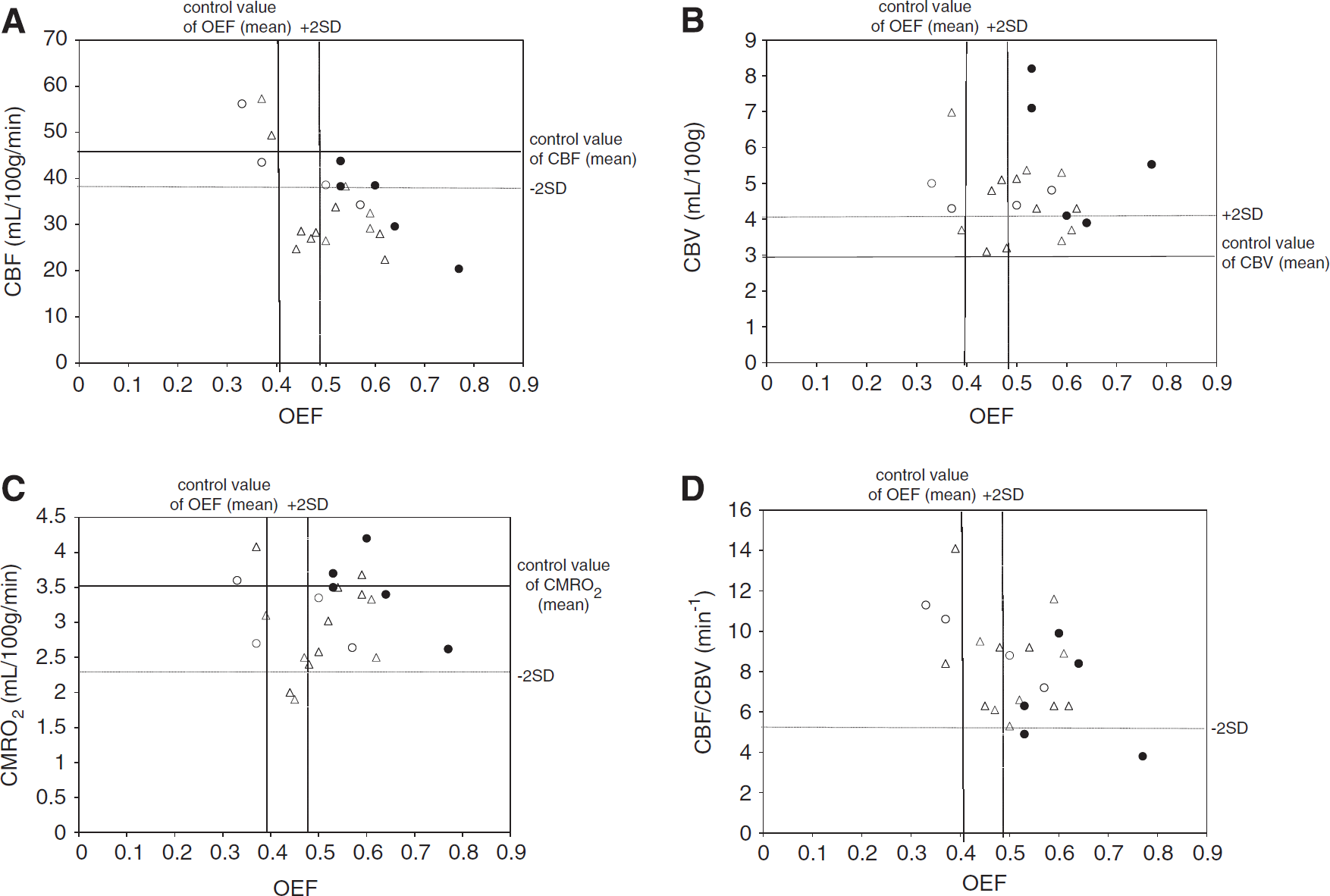
Plot of preoperative absolute values of oxygen extraction fraction (OEF) versus cerebral blood flow (CBF) (
Postoperative Positron Emission Tomography Parameters in Symptomatic Hyperperfusion
Figure 3 illustrates temporal changes in PET parameters in seven hemispheres of six patients with postoperative hyperperfusion. The CBF values in patients with postoperative hyperperfusion significantly increased from the preoperative baseline value of 34.1 ± 8.2 mL/100 g per minute (
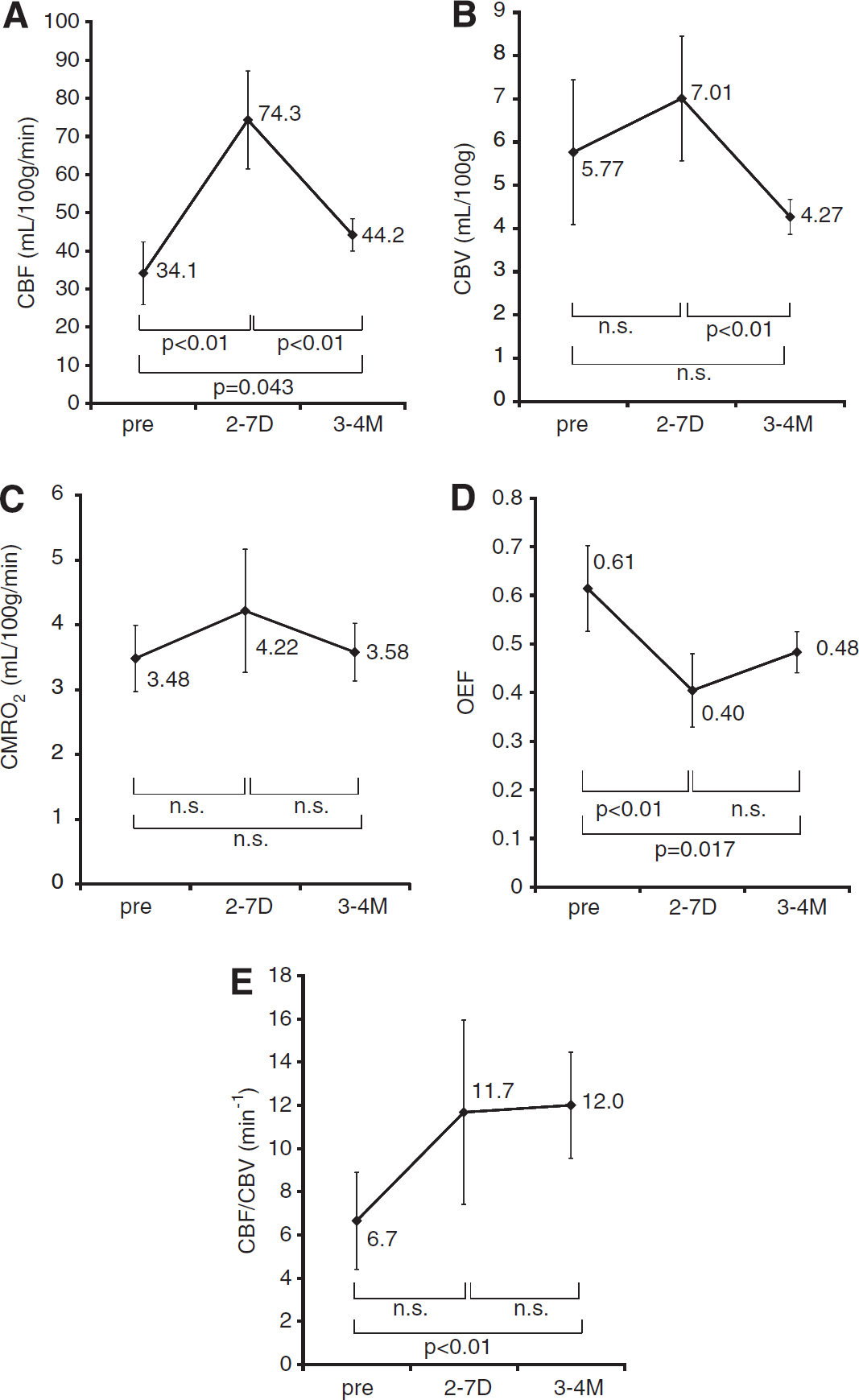
Graphs showing sequential changes in cerebral blood flow (CBF) (
Comparison of Cerebral Blood Flow with Cerebral Metabolic Rate of Oxygen
Figure 4 shows the correlation between CMRO2 and CBF. The simulated curve shows that increases in CBF lead to smaller changes in CMRO2. Applying the Renkin-Crone model (Crone, 1963; Renkin, 1959) to the relationship between CMRO2 and CBF, the best equation fitting our data for this relationship between them was
Graph showing the correlation between cerebral blood flow (CBF) and cerebral metabolic rate of oxygen (CMRO2). The Renkin-Crone model (Crone, 1963; Renkin, 1959) was applied to the relationship between CBF and CMRO2. The fitted curve shows that increases in flow lead to smaller changes in CMRO2. The relationship between CBF and CMRO2 almost fits the model for all cases, with the exception of two cases with postoperative seizure, in which the plots were above the curve. Number indicated the case number, respectively.
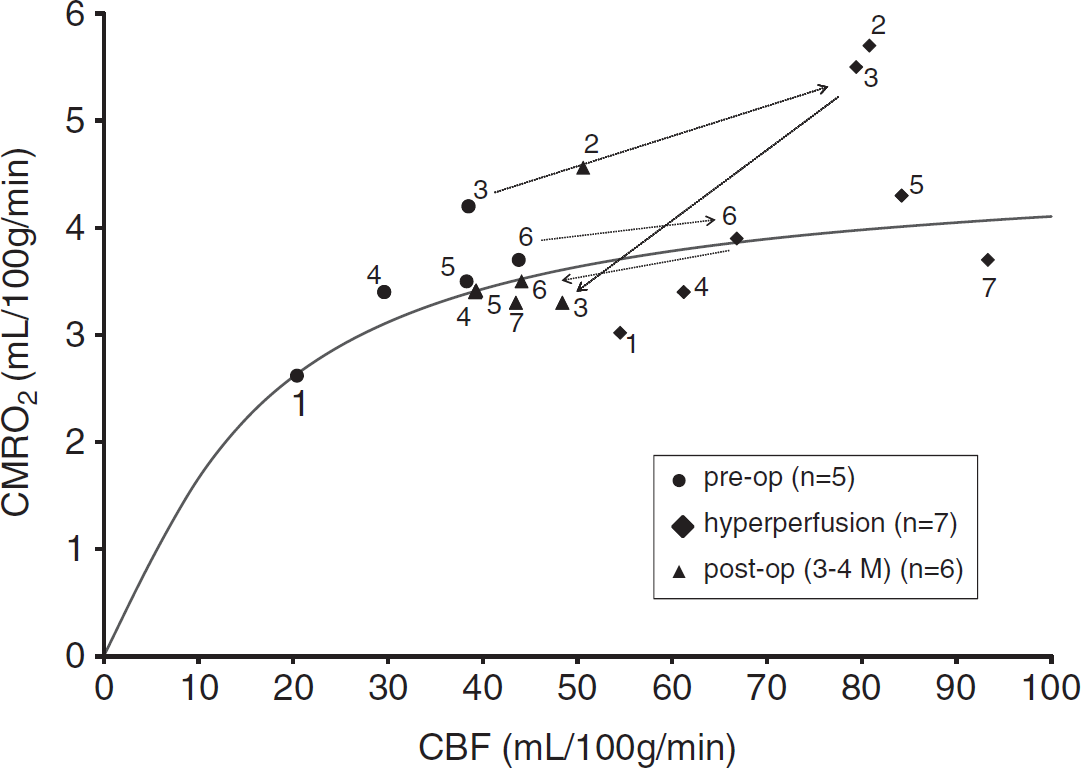
The fitted curve (Figure 4) showed that the increase in CMRO2 was linear until a flow of ~30 mL/100 g per minute was achieved, and it then increased more gradually as the flow increased. The relationship between CBF and CMRO2 almost fits the Rankin–Crone model (Crone, 1963; Renkin, 1959) with the exception of two cases with postoperative seizure, in which the plots were above the curve.
Representative Case
A 41-year-old woman (case 5) experienced a transient ischemic attack of left-sided sensory disturbance for a few minutes 5 years ago, and her symptoms gradually worsened. Neuroradiologic examinations showed typical findings compatible with MMD. A PET study indicated misery perfusion on the right hemisphere (Figure 5). The STA-MCA bypass surgery was performed successfully, and she awoke from anesthesia without neurologic deficits. On the third POD, sensory disturbance lasting 30 minutes occurred; similar episodes were repeated several times until the seventh POD. A PET study on POD 3 showed increased CBF and decreased OEF around the anastomotic site. Symptomatic hyperperfusion was diagnosed and her blood pressure was carefully monitored and controlled. Symptoms spontaneously resolved, and the patient was discharged on POD 10.
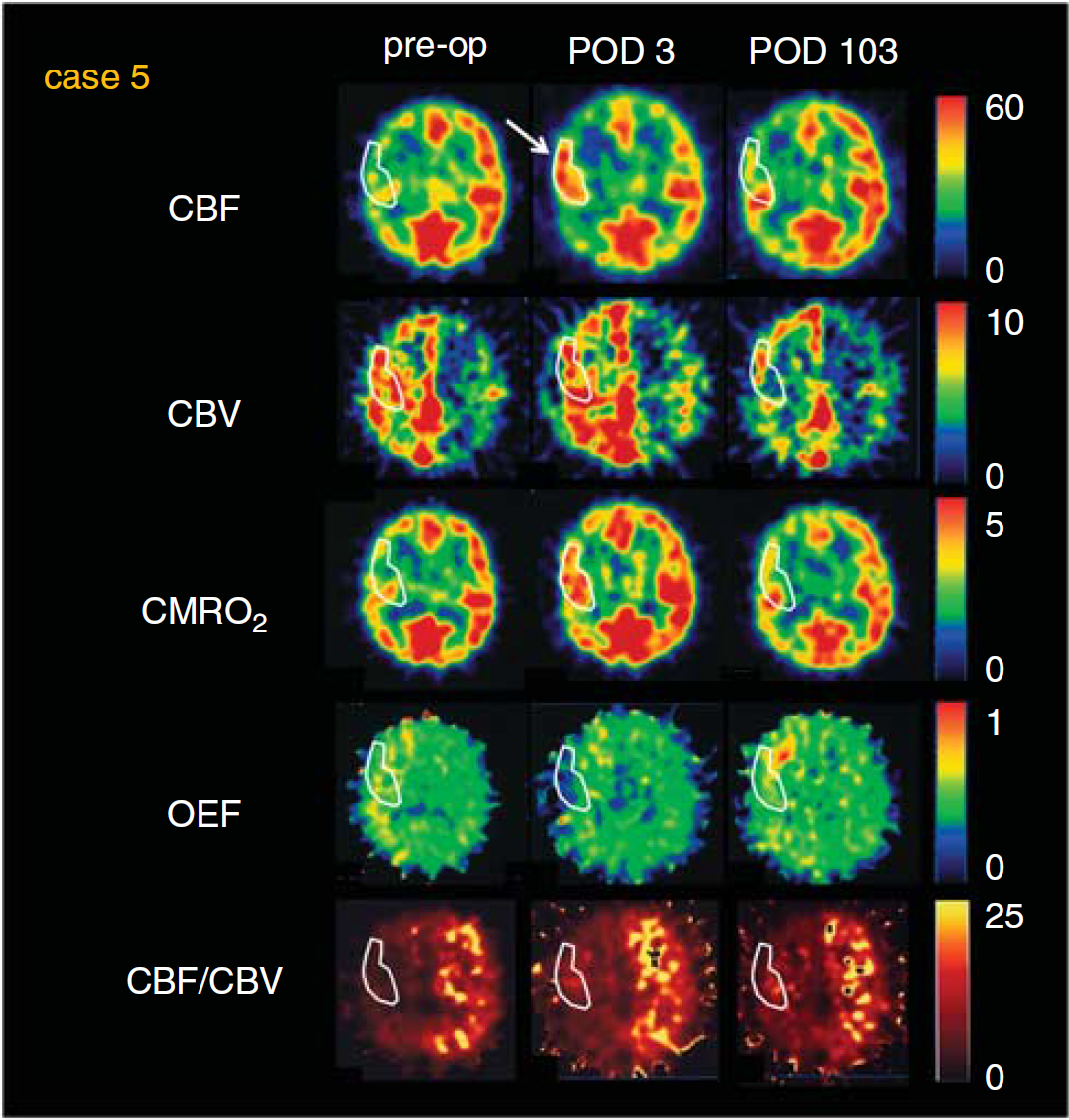
A series of positron emission tomography (PET) studies of a moyamoya disease (MMD) patient (case 5) with symptomatic hyperperfusion. Left: preoperative examinations revealed severe hypoperfusion in the right hemisphere with markedly increased cerebral blood volume (CBV) and oxygen extraction fraction (OEF). CBF/CBV was markedly decreased. Middle: studies obtained on postoperative day 3 showing a marked increase in CBF (white arrow), with persistent increased CBV. Although cerebral metabolic rate of oxygen (CMRO2) was slightly increased, OEF markedly decreased. Right: postoperative examinations obtained 3 months after revascularization. CBF, CMRO2, and OEF were normalized, and CBV and CBF/CBV were improved over the preoperative status. CBF, cerebral blood flow; POD, postoperative day.
Discussion
Hyperperfusion Syndrome
Recently, cerebral hyperperfusion has received much attention as a possible cause of transient neurologic dysfunction after bypass surgery for MMD. The main neurologic deficits corresponding to dysfunctions around the bypass site at the perisylvian area include dysarthria, hand motor dysfunction, and motor or sensory dysphasia. Unlike the classical triad of symptoms such as severe unilateral headache, face and eye pain, and seizures and established criteria of CBF after CEA (Piepgras et al, 1988; Sundt et al, 1981; van Mook et al, 2005), a critical definition of CBF using PET, a gold standard, for the diagnosis of hyperperfusion after bypass surgery for MMD remains unestablished.
Here the authors reported, for the first time in MMD, CBF and oxygen metabolism with preoperative and postoperative PET, after screening patients with hyperperfusion first with qualitative 123I-IMP SPECT, the reported definition of postoperative hyperperfusion in MMD, and analyzed the correlation of preoperative PET parameters with development of symptomatic hyperperfusion, and found that preoperative OEF was significantly increase in the patients, whereas no differences were observed in the other parameters. A postoperative PET study, exclusively performed for cases with symptomatic hyperperfusion due to difficult logistic reasons, clearly showed that transient neurologic deterioration due to hyperperfusion was characterized by transient increases in CBF caused by prolonged recovery of CBV, as reported previously in hyperperfusion after CEA and carotid artery stenting (CAS). In terms of oxygen metabolism, however, patients with hyperperfusion were classified into two types, those with normal and elevated CMRO2, respectively, and the latter type was complicated with postoperative seizure.
Diagnosis of Symptomatic Hyperperfusion in Moyamoya Disease
In MMD patients, the incidence of symptomatic hyperperfusion after bypass surgery varies considerably from 21.5% to 38.2% (Fujimura et al, 2007, 2011), because of a lack of quantitative evaluation of postoperative CBF and different study populations. Unlike hyperperfusion after CEA, the operational definition of hyperperfusion after bypass surgery for MMD remains unestablished. In this paper, qualitative 123I-IMP SPECT was conducted first during POD 1 to 3 to screen all patients for the presence of hyperperfusion according to the previously reported diagnostic criteria of postoperative hyperperfusion in MMD. The incidence of hyperperfusion on qualitative 123I-IMP SPECT (31%) and symptomatic hyperperfusion (16.7%) in the present study was consistent with the previous report.
Here, the postoperative PET study clearly showed that once symptomatic, mean CBF values increased to 218% of preoperative values, which seems to be consistent with the original concept of post CEA perfusion, and peak CBF values at the subacute postoperative stage were equal to or more than the control + 2s.d. (57.8 mL/100 g per minute), the predefined value of hyperperfusion on PET calculated from the healthy hemisphere in patients with unilateral stenoocclusive lesions in all cases (Fink et al, 1993). This definition based on normal control values seems to be practical since preoperative CBF values on PET may not always be available because of inherent logistic difficulties as in the present study. Taken together, these results indicated that if patients with increased CBF on qualitative 123I-IMP SPECT develop corresponding symptoms postoperatively (the previously reported definition of symptomatic hyperperfusion), peak CBF values measured using PET during subacute stages would be almost consistent with the traditional concept of post CEA hyperperfusion (> 100% increase over the baseline) and more than predefined CBF threshold values (control + 2s.d.). The CBF values 3 to 4 months postoperatively remained higher than preoperative values, but returned to normal ranges, indicating that the state of hyperperfusion was temporary.
Mechanism of Hyperperfusion in Moyamoya Disease
Preoperative increases in CBV persisted during hyperperfusion and decreased 3 to 4 months postoperatively, suggesting the prolonged recovery of high CBV values, despite immediate increases in perfusion pressure after direct bypass, may have a key role in the development of hyperperfusion and the associated clinical symptoms lasting for 1 to 14 days in our patients. Accordingly, the preoperative decreased cerebral perfusion pressure increased rapidly within 2 to 7 days of surgery. However, the only PET study on postoperative hyperperfusion after CAS (Matsubara et al, 2009) showed significant increases in CBF and CBF/CBV ratios despite the lack of significant changes in CBV during the acute stage. Interestingly, such PET findings were observed in the contralateral hemisphere during the acute stage after CAS. Such differences in temporal changes of PET parameters between MMD and CAS are probably explained by the types of revascularization (high flow or low flow), presence of intracranial arterial stenosis in MMD, and the fact that our study on symptomatic MMD mainly consisted of cases with severe hemodynamic compromise than the CAS PET study (Matsubara et al, 2009). Therefore, fundamental mechanisms underlying postoperative hyperperfusion, prolonged recovery of vascular reserve, after bypass surgery for MMD seem to be similar to those after carotid revascularization, although the PET study on carotid stenosis with severe hemodynamic compromise is mandatory to conclude this point. Stringent blood pressure control is similarly necessary for patients with postoperative hyperperfusion in MMD (Fujimura et al, 2011), although the blood pressure-lowering effect on the untreated contralateral hemisphere should be carefully considered.
Risk of Symptomatic Hyperperfusion
Decreased vascular reserve on preoperative SPECT images has been reported as a predictor of hyperperfusion syndrome after CEA (Hosoda et al, 2001; Ogasawara et al, 2003). Cerebral perfusion pressure is generally considered to reflect cerebral vascular reserve and the CBF/CBV ratio is an index of cerebral perfusion pressure (Gibbs et al, 1984). Cerebral blood volume is closely related to arteriolar dilatation (Kontos et al, 1977; Wahl et al, 1970) in response to decreased perfusion pressure distal to hemodynamically significant arterial stenosis. Here, we showed among the preoperative PET parameters that increased OEF was the only significant risk factor for the development of symptomatic hyperperfusion. Also, it is interesting to note that although not significantly different, CBV values tended to be higher in symptomatic hyperperfusion. In this context, Derdeyn et al (2002) reported the revised concept of hemodynamic staging using PET and showed that among patients with increased OEF, those with increased CBV may indicate pronounced vasodilatation due to exhausted autoregulatory vasodilatation and be associated with a higher risk of subsequent stroke, whereas those with normal CBV may reflect preserved autoregulatory capacity and be associated with a smaller incidence of subsequent stroke. Taken together, our observations presented in Figure 2B may indicate that even in patients with increased OEF, preoperative increased CBV confers a higher risk of symptomatic hyperperfusion than those with normal CBV. Further studies are necessary to conclude this point.
Cerebral Oxygen Metabolism of Hyperperfusion
The present series consisted of patients with preoperative moderate/severe hemodynamic compromise, and temporary clamping of the recipient arteries may confer additional ischemic insult to the brain adjacent to the anastomotic site during bypass. Previous PET studies in patients with cerebral infarctions showed that rapid perfusion to a cerebrum that has been in a state of chronic ischemia may increase oxygen mechanism (postischemic oxygen hypermetabolism) (Marchal et al, 1996, 1999). The postulated mechanisms are (1) overexcitation of cellular metabolism in cells destined to survive or (2) excessive firing of neurons undergoing irreversible damage from a massive release of excitatory amino acids during the period of ischemia or early noxious inflammatory changes. Since no frank infarctions were noted in the area with hyperperfusion on magnetic resonance imaging in subacute or chronic periods in the present study, the above-mentioned overexcitation of cellular metabolism cannot be ruled out as a mechanism underlying postoperative hyperperfusion.
Repetitive neurologic symptoms in patients without overt postoperative convulsion may be caused by partial seizure. Postoperative seizure is considered to be caused by two basic mechanisms; free radical generation mainly caused by extravascular leakage of blood components, and disturbance of ionic balances across the cell membrane caused by ischemia or hypoxia, both of which are closely linked (Manaka et al, 2003). Since postoperative hyperperfusion and seizure share two common underlying mechanisms, that is, free radical generation and ischemic insult, the causal relationship between these two phenomena is difficult to answer conclusively based on this study.
Significant oxygen hypermetabolism was noted only in cases complicated with postoperative seizure. Seizure is an abnormal physiological state that, unlike somatosensory processing, places supranormal demands on autoregulatory mechanisms due to an enormous increase in CMRO2 (Folbergrova et al, 1981). During sustained seizures, CBF increases with a corresponding increase in CMRO2 (Brodersen et al, 1973; Theodore et al, 1996). Our analysis using the Renkin–Crone model (Crone, 1963; Renkin, 1959) showed, with the exception of two cases complicated with seizure, there was no mismatch with CBF and CMRO2. The increased tendency of oxygen hypermetabolism during symptomatic hyperperfusion compared with preoperative or chronic periods even in cases without postoperative seizure was also shown in hyperperfusion after CAS (Matsubara et al, 2009). Such oxygen hypermetabolism may explain the sustained neurologic deterioration after bypass surgery for MMD.
Conclusion
This study revealed that symptomatic hyperperfusion in MMD is characterized by temporary increases in CBF > 100% over preoperative values caused by prolonged recovery of increased CBV. Among preoperative PET parameters, increased OEF was the only significant risk factor for symptomatic hyperperfusion (
Disclosure/conflict of interest
The authors declare no conflict of interest.