
Abstract
Despite an undisputed association between vasospasm and delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage (SAH), there is debate if this association implies causality. It has been suggested that cerebral infarction is a better outcome measure than vasospasm in clinical trials and observational studies. To further investigate the relationship between infarction and outcome, we performed a systematic review and meta-analysis of all randomized, double-blind, placebo-controlled trials that studied the efficacy of pharmaceutical preventive strategies in SAH patients, and had both cerebral infarction and clinical outcome as outcome events. Effect sizes were expressed in (pooled) risk ratio (RR) estimates with corresponding 95% confidence intervals (CIs). Sensitivity analyses were performed for studies with a low risk of bias and for those who reported outcome at 3 months after SAH. Twenty-four studies including 8,552 patients were included. Pharmaceutical treatments decreased the incidence of both cerebral infarction (RR: 0.83; 95% CI: 0.74 to 0.93) and of poor functional outcome (RR: 0.92; 95% CI: 0.86 to 0.98). The sensitivity analyses did not change the results essentially. These data suggest that the previously observed association between cerebral infarction and functional outcome implies causality, and that cerebral infarction is a better outcome measure than vasospasm in clinical trials and observational studies.
Keywords
Introduction
Patients with aneurysmal subarachnoid hemorrhage (SAH) are at high risk of developing delayed cerebral ischemia (DCI). Delayed cerebral ischemia can progress to cerebral infarction, resulting in severe disability or death in 50% of patients. The pathogenesis of DCI remains incompletely understood. Despite the undisputed association between arterial narrowing (‘vasospasm’) and DCI, there is debate if this association implies causality (Millikan, 1975).
Many randomized controlled trials have been performed over the last decades aiming to find a treatment that effectively prevents DCI. Although several drugs were identified that successfully prevent vasospasm, no effects on clinical outcome were observed (Macdonald et al, 2008; Etminan et al, 2011). It has been proposed that cerebral infarction and functional outcome, and not vasospasm, should be the main outcome measures in clinical trials and observational studies (Vergouwen et al, 2010). The aim of the present study was to investigate if a lower incidence of cerebral infarction after SAH correlates with better functional outcomes.
Materials and methods
For this systematic review, the Cochrane Collaboration format was used (Higgins and Green, 2008).
Selection Criteria
Statistics
Data were processed in Review manager 5.0.25 as supplied by the Cochrane Collaboration. Effect sizes were expressed in (pooled) risk ratio (RR) estimates. Statistical uncertainty was expressed in 95% confidence intervals (CIs). Pooled data were interpreted to be heterogeneous in case the probability value of the χ2 test was ≤0.10. If no heterogeneity could be demonstrated, we used a fixed-effects model. Otherwise, a random-effects model was used. Two authors (MDIV and NE) independently assessed risk of bias by reviewing methodological quality of the included studies for allocation concealment and blinding. Funnel plots, including Begg's and Egger's statistical tests, were generated in Stata (version 9, College Station, TX, USA) to investigate potential bias. Sensitivity analyses were performed for studies with a low risk of bias (both on the items ‘allocation concealment’ and ‘blinding’), and for studies that reported functional outcome at 3 months after SAH.
Results
The initial search yielded 780 articles, of which ultimately 756 were excluded. The remaining 24 trials were included in the analysis, including 8,552 patients (Macdonald et al, 2008; Asano et al, 1996; Chou et al, 2008; Gomis et al, 2010; Haley et al, 1993, 1997; Hop et al, 2000; Kassell et al, 1996; Lanzino et al, 1999; Lanzino and Kassell, 1999; Ohman and Heiskanen, 1988; Petruk et al, 1988; Pickard et al, 1989; Saito et al, 1998; Shaw et al, 2000; Shibuya et al, 1992; Siironen et al, 2003; Juvela et al, 2005; Springborg et al, 2007; Suzuki et al, 1989; Tseng et al, 2009; van den Bergh et al, 2005, 2006; Westermaier et al, 2010; Wong et al, 2010, 2011). A total of 4,818 patients were randomized to pharmaceutical treatment, and 3,734 patients to placebo. Characteristics of the included studies are listed in Table 1.
Characteristics of included studies
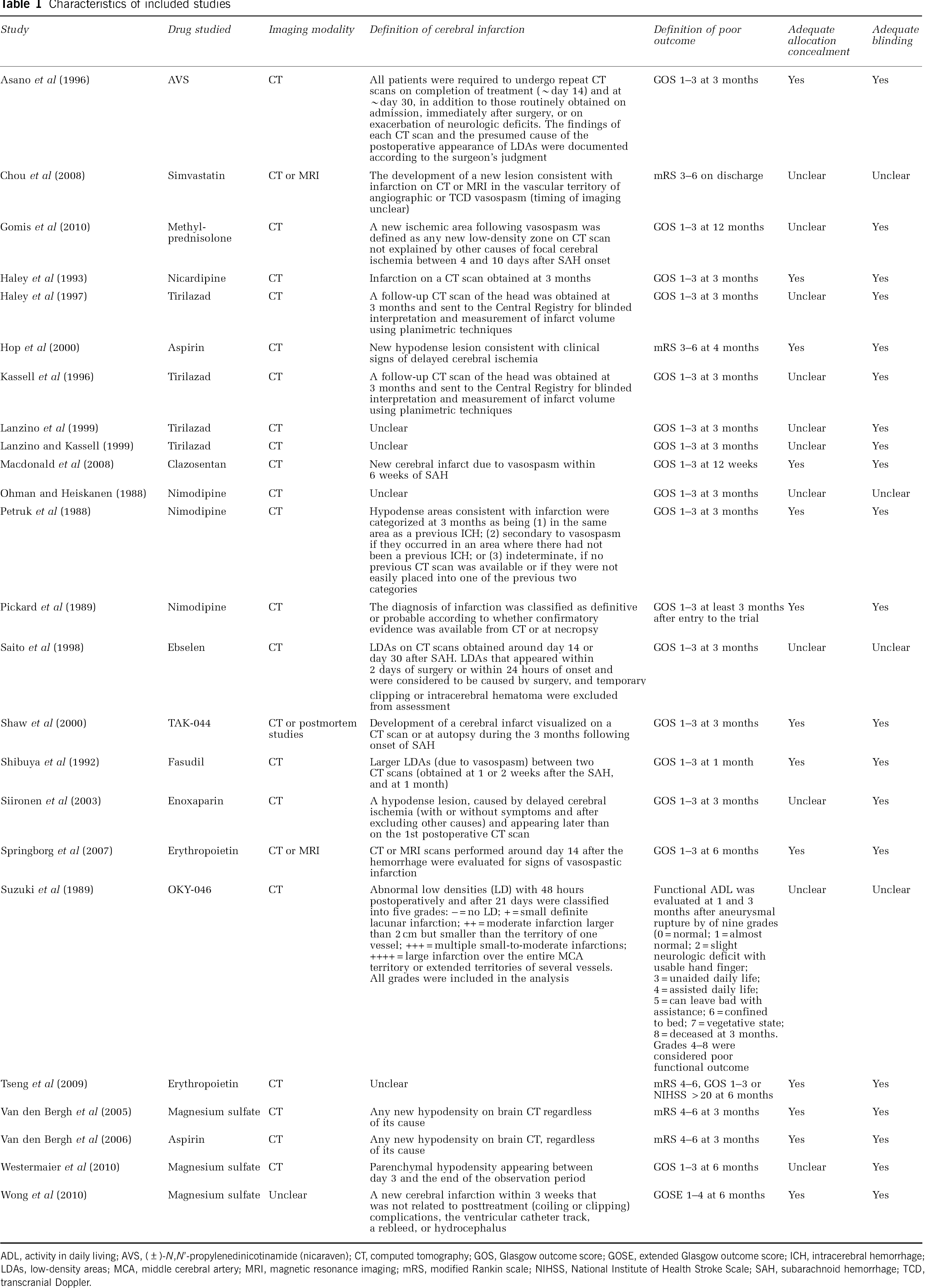
ADL, activity in daily living; AVS, (±)-
Analyses
For the analysis of cerebral infarction, data from 7,982 patients were available (4,508 patients randomized to pharmaceutical treatment and 3,474 to placebo). The overall number of patients with cerebral infarction was 1,282 in the group of patients randomized to pharmaceutical treatment and 1,182 in the placebo group. Our meta-analysis demonstrated a significant and favorable effect of treatment compared with placebo on cerebral infarction (pooled RR: 0.83; 95% CI: 0.74 to 0.93). Heterogeneity between the trials was high (
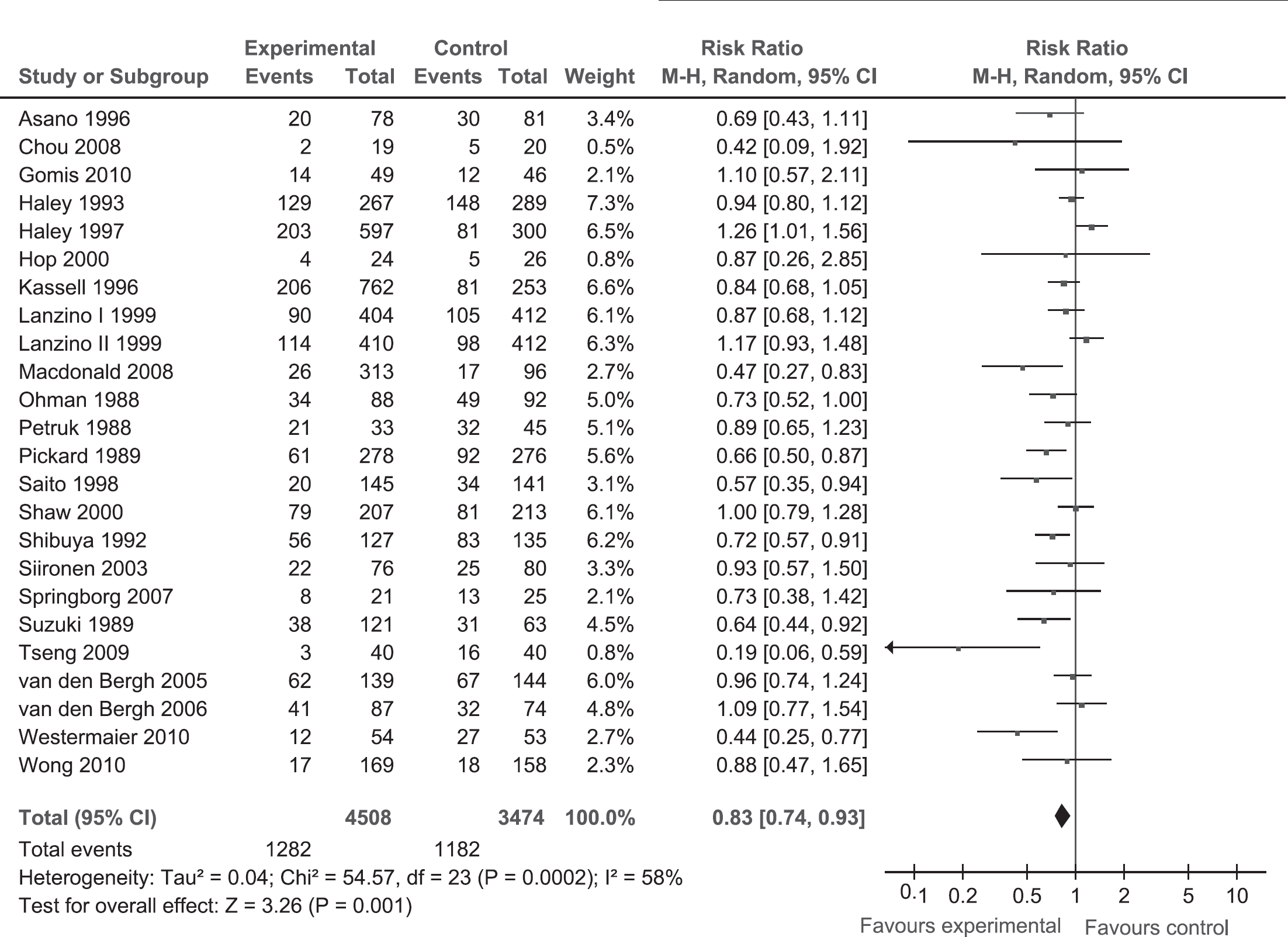
(Pooled) risk ratio (RR) estimates for patients on pharmaceutical treatment to have cerebral infarction. CI, confidence interval.
For clinical outcome, most studies used the Glasgow outcome scale (Macdonald et al, 2008; Asano et al, 1996; Gomis et al, 2010; Haley et al, 1993, 1997; Kassell et al, 1996; Lanzino et al, 1999; Lanzino and Kassell, 1999; Ohman and Heiskanen, 1988; Petruk et al, 1988; Pickard et al, 1989; Saito et al, 1998; Shaw et al, 2000; Shibuya et al, 1992; Siironen et al, 2003; Springborg et al, 2007; Westermaier et al, 2010; Wong et al, 2010) or modified Rankin scale (Chou et al, 2008; Hop et al, 2000; Tseng et al, 2009; van den Bergh et al, 2005, 2006) (Table 1). One study used a functional activity in daily living scale (Suzuki et al, 1989). For the meta-analysis of poor clinical outcome, data from 8,489 patients were available (4,784 patients randomized to pharmaceutical treatment, 3,705 to placebo). The number of patients with poor outcome was 1,352 in the pharmaceutically treated group and 1,133 in the placebo group. Meta-analysis showed a beneficial effect of treatment compared with placebo on poor clinical outcome (pooled RR: 0.92; 95% CI: 0.86 to 0.98). Heterogeneity between the trials was not significant (
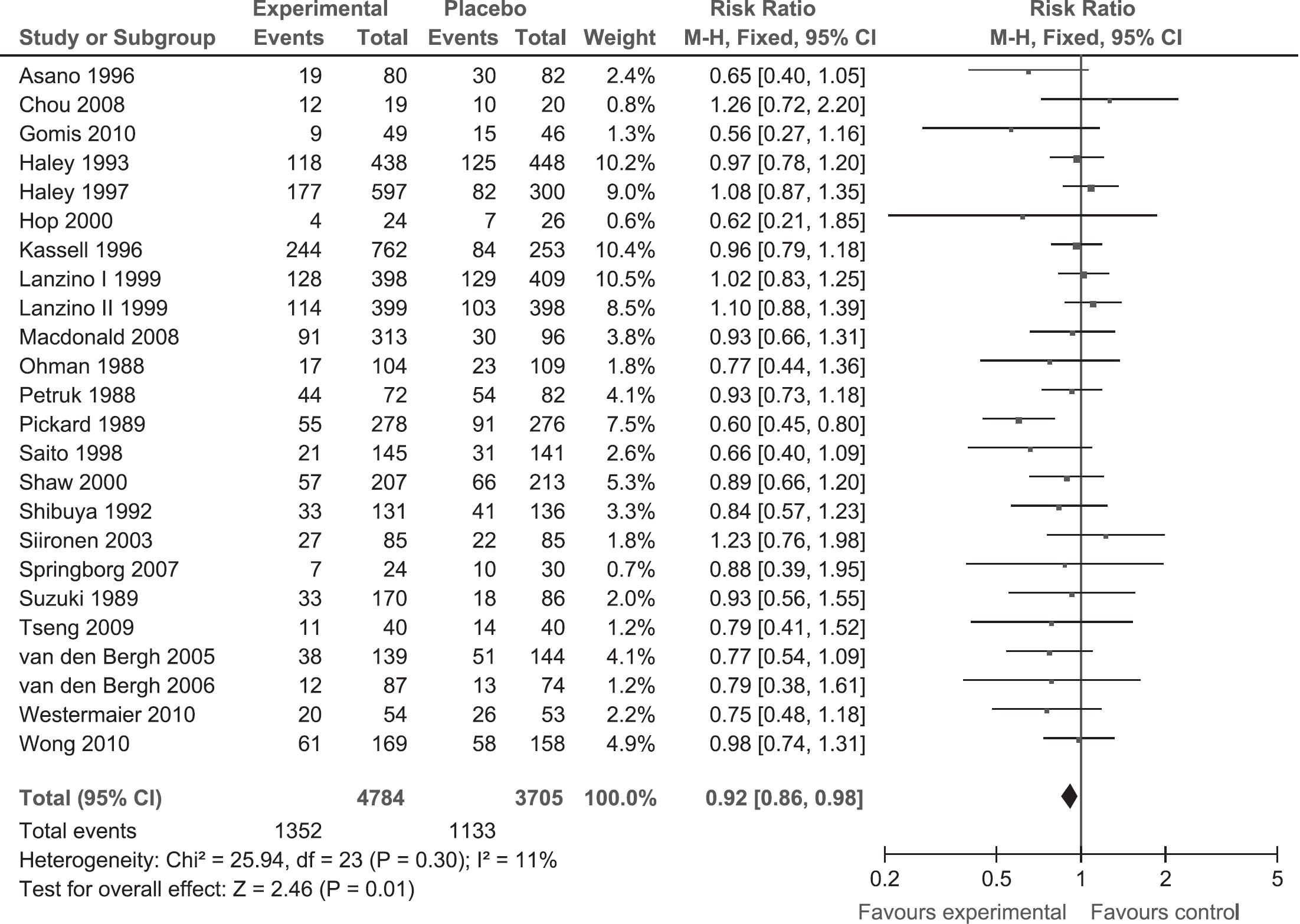
(Pooled) risk ratio (RR) estimates for patients on pharmaceutical treatment to have poor clinical outcome. CI, confidence interval.
Risk of Bias Assessments
For allocation concealment, risk of bias was low in 13 (Macdonald et al, 2008; Asano et al, 1996; Haley et al, 1993; Hop et al, 2000; Petruk et al, 1988; Pickard et al, 1989; Shaw et al, 2000; Shibuya et al, 1992; Springborg et al, 2007; Tseng et al, 2009; van den Bergh et al, 2005, 2006; Wong et al, 2010) and unclear in 11 studies (Chou et al, 2008; Gomis et al, 2010; Haley et al, 1997; Kassell et al, 1996; Lanzino et al, 1999; Lanzino and Kassell, 1999; Ohman and Heiskanen, 1988; Saito et al, 1998; Siironen et al, 2003; Suzuki et al, 1989; Westermaier et al, 2010) (Table 1). For blinding, risk of bias was low in 20 studies (Macdonald et al, 2008; Asano et al, 1996; Gomis et al, 2010; Haley et al, 1993, 1997; Hop et al, 2000; Kassell et al, 1996; Lanzino et al, 1999; Lanzino and Kassell, 1999; Petruk et al, 1988; Pickard et al, 1989; Shaw et al, 2000; Shibuya et al, 1992; Siironen et al, 2003; Springborg et al, 2007; Tseng et al, 2009; van den Bergh et al, 2005, 2006; Westermaier et al, 2010; Wong et al, 2010), and unclear in four studies (Chou et al, 2008; Ohman and Heiskanen, 1988; Saito et al, 1998; Suzuki et al, 1989). High risk of bias was not observed in any of the studies. One of the authors of this systematic review acknowledges potential risk of bias, because he is an author of one of the studies included in this systematic review (Macdonald et al, 2008). Funnel plots are shown in Figures 3A and 3B. For the cerebral infarction outcome measure, the Egger's test supports the evidence of significant level of bias (

Funnel plot for outcome measure cerebral infarction (
Sensitivity Analyses
In the sensitivity analysis that only included studies with a low risk of bias, as assessed on the items ‘allocation concealment’ and ‘blinding,’ 13 studies were included with 3,831 patients (Macdonald et al, 2008; Asano et al, 1996; Haley et al, 1993; Hop et al, 2000; Petruk et al, 1988; Pickard et al, 1989; Shaw et al, 2000; Shibuya et al, 1992; Springborg et al, 2007; Tseng et al, 2009; van den Bergh et al, 2005, 2006; Wong et al, 2010). The pooled RR for cerebral infarction was 0.70 (95% CI: 0.56 to 0.88) and for poor outcome 0.78 (95% CI: 0.67 to 0.90) (figures not shown). Heterogeneity between the trials was significant in the cerebral infarction analysis (
Discussion
This systematic review including 8,552 patients shows that a lower incidence of cerebral infarction after SAH correlates with a lower incidence of poor functional outcome. The sensitivity analysis that only included studies with a low risk of bias confirmed these findings. The sensitivity analysis that reported on functional outcome 3 months after SAH showed similar findings, though the poor outcome analysis had CIs that included 1.00.
Previous studies found strong associations between vasospasm, DCI, cerebral infarction, and poor functional outcome (Fisher et al, 1977; Vergouwen et al, 2011; Rabinstein et al, 2004; Fergusen and Macdonald 2007). However, associations do not always represent causal relationships. Especially for vasospasm, it is debated if it causes DCI and poor functional outcome (Millikan, 1975; Vergouwen et al, 2008). A recent systematic review including 4,235 patients with SAH showed that pharmaceutical interventions decreased vasospasm after SAH, but not poor functional outcome (Etminan et al, 2011). This dissociation between vasospasm and clinical outcome could result from methodological problems, sample size, insensitivity of clinical outcome measures, or from mechanisms other than vasospasm that also contribute to poor outcome. Current understanding is that the pathogenesis of DCI is multifactorial. Microthromboembolism, cortical spreading ischemia, delayed effects of acute SAH-induced brain injury, and impaired cerebral autoregulation have been suggested to have a role in clinical outcome (Vergouwen et al, 2008; Dreier et al, 2009; Yundt et al, 1998). Since cerebral infarction is the ultimate outcome of DCI, it has been suggested that cerebral infarction is a better outcome measure in observational studies and clinical trials than vasospasm (Vergouwen et al, 2010). The findings of the present study support this suggestion. Obviously, the main outcome measure in such studies should be functional outcome (Vergouwen et al, 2010).
This study has some limitations. Significant heterogeneity was observed in the cerebral infarction meta-analyses. This might result from the many different drugs used in the various studies, which all have different pharmacological properties. The studies that were included did not use a uniform definition of cerebral infarction, which may introduce some variability. To account for the observed heterogeneity, we used a random-effects model instead of a fixed-effects model. In addition, the meta-analysis shows an association between cerebral infarction and poor outcome. As with the relation between angiographic vasospasm and DCI, it is still conceivable that this relation is not causal, although this seems unlikely since it would require one to accept that dead brain is not somehow detrimental to outcome. Furthermore, for the outcome measure ‘functional outcome,’ statistical tests showed evidence of bias. However, our sensitivity analysis that only included studies with low risk of bias confirmed our finding that lower rates of infarction are correlated with better functional outcomes. Finally, in many of the studies included in the meta-analysis, diagnosis of cerebral infarction was based on CT scans only. Since the sensitivity of CT to detect cerebral infarction is low, the result of the meta-analysis might significantly underestimate the presence of infarction (Dreier et al, 2002). Future studies should investigate the relationship between cerebral infarction on magnetic resonance imaging and functional outcome after SAH.
In conclusion, pharmaceutical treatments decreased both cerebral infarction and poor functional outcome after SAH. These data suggest that the previously observed association between cerebral infarction and functional outcome implies causality. Considering our prior meta-analysis studying the relationship between angiographic vasospasm and outcome that showed no relationship (Etminan et al, 2011), the present results suggest that cerebral infarction may be a better outcome measure than vasospasm in clinical trials and observational studies.
Footnotes
Acknowledgements
MDIV is financially supported by a grant from the Netherlands Thrombosis Foundation, The Netherlands (2010-4). Drs N Etminan and RL Macdonald received research support from The Physicians Services Incorporated Foundation.
Dr RL Macdonald is a consultant for Actelion Pharmaceuticals and Chief Scientific Officer of Edge Therapeutics, Inc.