
Abstract
Dopamine D2 receptor occupancy of antipsychotic drugs is calculated relative to the subject's D2 receptor binding potential (BP) in the drug-free state (baseline BP). Because baseline BP is seldom known in patients with schizophrenia, population means from unrelated control samples are often used to estimate it. However, this is likely to introduce bias and error into the occupancy measure. There is thus a need for a method to reliably estimate baseline BP for patient populations in whom it may be impractical or unethical to get baseline measurements. It has been previously found that the relationship between plasma concentration and dopamine receptor occupancy by antipsychotic drugs follows a sigmoid Emax model. Based on this, we developed a method for calculating dopamine D2 receptor occupancy by antipsychotic drugs using an inhibitory Emax model (Imax method) that estimates individual baseline BPs. To validate this, we compared the result from the Imax method with actual occupancy and estimated occupancy calculated from the average baseline BP (substitution method). The data for validation were obtained from two different receptor occupancy studies with the antipsychotic medications YKP1358 and aripiprazole. We estimated the reliability between the true measured occupancy and the predicted occupancy using the intraclass correlation coefficient (ICC), and the variability of occupancy was also compared between the Imax and substitution methods. In YKP1358 study, all the ICCs of the Imax method were above 0.8, but those of the substitution method showed values lower than 0.8. In aripiprazole study, the ICCs of the Imax method were higher than those of the substitution method, but all the ICCs showed higher values than 0.8. The variability of Imax method was significantly smaller than that of substitution method in both studies. The Imax method shows better reliability and less variability than the substitution method. The Imax method can be applied for receptor occupancy study, and bring more reliability and accuracy to the occupancy study in patients with schizophrenia.
Keywords
Introduction
Neuroimaging has been applied to characterize the pharmacological profiles of antipsychotic drugs (Farde et al, 1992; Fischman et al, 2002; McGuire et al, 2008; Pien et al, 2005; Willmann et al, 2008). In particular, [11C]raclopride positron emission tomography (PET) is a useful method for measuring dopamine D2 receptor occupancy by antipsychotic drugs. Dopamine D2 receptor occupancy is a meaningful biomarker in that it reflects the antipsychotic binding at the effect site and that it can predict the clinical response to antipsychotic drugs (Kapur et al, 2000).
The dopamine receptor occupancy is usually expressed as the percentage reduction of binding potential (BP): Occupancy (%) = (BPbaseline—BPdrug>)/ BPbaseline × 100, where BPbaseline is BP in drug-free state and BPdrug is BP after the administration of antipsychotic drugs. It follows from this that baseline BP needs to be measured before subjects receive the antipsychotic drug to calculate the dopamine receptor occupancy. However, in patients with schizophrenia, it is often not feasible or ethical to measure a drug-free baseline BP, because this would mean withholding treatment. For this reason, most studies that measure dopamine D2 receptor occupancy by antipsychotic drugs in patients have substituted baseline BPs of the enrolled patients with the average values reported previously for drug-näve patients or healthy volunteers (substitution method; Arakawa et al, 2008; Farde et al, 1992; Gefvert et al, 1998; Grunder et al, 2008; Kapur et al, 1999; Tauscher et al, 2002).
Although the substitution method has been widely accepted for calculation of dopamine D2 receptor occupancy in patients with schizophrenia, it has several significant limitations. First, it does not take into account population differences in baseline BP. This is an issue because, although there is a controversy about the issue (Farde et al, 1990; Wong et al, 1986), studies in drug-naïve patients with schizophrenia indicate that the disorder may be associated with elevated dopamine D2 receptor BP (see review by Laruelle (1998) for further discussion), which would cause occupancy levels to be overestimated when healthy control mean BP is used as the baseline BP. Second, it does not account for individual differences in baseline BP. There is greater variability in dopamine D2 receptor BP in schizophrenia than in controls, which may reflect heterogeneity in the disorder (Kestler et al, 2001; Laruelle, 1998), so that even where mean BP from drug-naïve patients is substituted, the true occupancy may be under- or overestimated in some patients. Finally, the possibility of dopamine receptor upregulation induced by antipsychotic drugs is not taken into consideration by the substitution method.
For these reasons, we developed an alternative method for calculation of dopamine D2 receptor occupancy. Many drug–response relationships can be modeled by an Emax model, which is based on the basic pharmacology of drug interactions with receptors and is used to model the saturable process of receptor occupancy by drugs (Alvan et al, 1999). This model is commonly used to predict the relationship between a response of interest (e.g., occupancy) and drug dose during drug development (Danhof and Mandema, 1992; Meibohm and Derendorf, 1997). The relationship between plasma concentration and dopamine receptor occupancy by antipsychotic drugs has been found to follow a sigmoid Emax model (Grunder et al, 2008; Kapur et al, 1999; Lim et al, 2007; Mamo et al, 2004; Remington et al,2006). Considering the equation for receptor occupancy can be described as (BPbaseline—BPdrug)/BPbaseline × 100 = Emax × concentration/(EC50 + concentration), we can obtain an inhibitory Emax model for the relationship between BP and concentration: BP = BPbaseline—Imax × concentration/(IC50 + concentration), where Emax is the maximum occupancy (100% of receptors occupied by drug), EC50 is the plasma drug concentration associated with 50% occupancy of dopamine receptors, Imax is the maximum inhibitory effect of drug on BP, and IC50 is the plasma drug concentration associated with 50% decrease of BP. This means that if BP is available for a range of plasma drug levels, the inhibitory Emax model can be used to estimate the BP at other plasma drug levels including the drug-free state. Using this model, we estimated individual baseline BP and calculated individual dopamine D2 receptor occupancy with the estimated baseline BP (Imax method).
To validate this, we calculated dopamine D2 receptor occupancy of two dataset using the Imax method, compared the results with actual dopamine D2 receptor occupancy and estimated occupancy calculated from the substitution method.
Materials and methods
The data for validation were obtained from two different studies investigating dopamine D2 receptor occupancy during antipsychotic drug administration. One study used YKP1358, a novel atypical antipsychotic drug currently under clinical development, and the other used aripiprazole. YKP1358 (C21H24ClFN2O3) has in vitro affinities for D2L, D2S, and 5-HT2A receptors of 85, 91, and 0.83 nmol/L, respectively, (Lim et al, 2007), and aripiprazole has in vitro affinities for D2 and 5-HT2A receptors of 0.34 and 3.4 nmol/L (Ki values), respectively (Hirose and Kikuchi, 2005). YKP1358 shows the general pharmacological profile of an atypical antipsychotic drug. Aripiprazole is a partial agonist, and is known to obtain very high receptor occupancy without evoking extrapyramidal side effects (Yokoi et al, 2002). Both projects were approved by the Institutional Review Board of Seoul National University Hospital, Seoul, Korea.
Participants
Healthy male volunteers participated in the studies. After complete description of the study to the volunteers, written informed consent was obtained. Screening tests included a complete blood count, blood electrolyte analysis, urine analysis, electrocardiography, and a psychiatric interview. Volunteers with medical and/or psychiatric disease were excluded. The number of participants was 9 for the YKP1358 study and 18 for the aripiprazole study. Mean (± s.d.) age, height, and body weight of healthy volunteers were 25.3 ± 4.7 years, 174.7 ± 6.7 cm, and 70.0 ± 6.6 kg, respectively, in the YKP1358 project, and 22.9 ± 2.4 years, 174.6 ± 4.9 cm, and 69.6 ± 6.3 kg in the aripiprazole project (Table 1).
Study Design
Both studies were conducted using a single oral dose, parallel dose group (YKP1358: 100, 200, and 250 mg; aripiprazole: 2, 5, 10, and 30 mg) study design.
In the YKP1358 study, [11C]raclopride PET scans were performed before dose administration and at 2, 5, and 10 hours after the YKP1358 administration. Serial blood samples for the measurement of YKP1358 plasma concentration were obtained at time 0 (before dose administration), 0.33, 0.67, 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 24, and 32 hours after dosing.
In the aripiprazole study, the PET scans were conducted before and at 3, 45, and 120 hours after the aripiprazole administration. The blood samples were collected at time 0 (before dose administration), 0.5, 1, 2, 3, 5, 8,11, 20, 24, 29, 45, and 120 hours after the administration.
PET Scanning Procedure and Image Analysis
All PET scans were performed on the ECAT EXACT 47 scanner (Siemens-CTI, Knoxville, TN, USA). Dynamic three-dimensional emission scans (15 seconds × 8 frames, 30 seconds × 16, 60 seconds × 10, and 240 seconds × 10) were initiated concomitantly with a bolus injection of 370 to 740mBq [11C]raclopride and continued for 60 minutes. The mean injected radioactivity dose and specific radioactivity of [11C] raclopride were 20 mCi per PET scan and 0.4 × 106Ci/mol, respectively.
The acquired data were reconstructed in a 128 × 128 × 47 matrix with a pixel size of 2.1 × 2.1 × 3.4 mm by means of a filtered back-projection algorithm employing a Shepp–Logan filter, with a cutoff frequency of 0.3 cycles/pixel.
Static PET images obtained by combining all the frames of dynamic images were coregistered with the magnetic resonance images of the same individual. The magnetic resonance images were used to define the region of interest on the striatum and cerebellum (reference region; Ito et al. 1998). The region of interest was transferred onto the dynamic PET images to obtain the time-activity curves using the transformation parameters obtained by the coregistration of the static PET and magnetic resonance images.
A three-compartment model was employed for the kinetic analysis of the binding of [11C]raclopride with the dopamine D2 receptor (Ito et al, 1998). These compartments represent the concentration of radioligand in plasma (Cp), free or nonspecifically bound radioligand in brain (Cf), and specifically bound radioligand to receptors (Cb). The dopamine D2 receptor BP (BP = Bmax/Kd) in the striatum was calculated using a simplified reference tissue model in which the following equation was fit to obtain the BP and related parameters:

where Ct(t) and Cr(t) are the respective time-activity curves for striatum and cerebellum, R1 is the ratio of rate constants for ligand delivery from the plasma into the striatum and cerebellum, and k2 is the rate constant for ligand washout from the striatum (Lammertsma and Hume, 1996; Olsson and Farde, 2001).
Estimation of Baseline BP Using Inhibitory Emax Model
Previous observations have shown that the Emax model provides a good fit to describe dopamine D2 receptor occupancy by antipsychotic drugs (Grunder et al, 2008; Kapur et al, 1999; Lim et al, 2007; Mamo et al, 2004; Remington et al, 2006). We assumed that the change in BP after the administration of antipsychotic drugs would follow the inhibitory Emax model:

where Imax is the maximum inhibitory effect of drug on BP, Conc is plasma concentration of antipsychotic drug, IC50 is the plasma concentration associated with a 50% decrease of BP, and r is the Hill coefficient. When a very high dose of antipsychotic drug is administered, BP is equal to zero, and it follows from equation (1) that Imax is equal to BPbaseline. This enables baseline BP to be estimated by determining Imax.
Nonlinear mixed effects modeling simultaneously estimated fixed effects and random effects in the inhibitory Emax model. The fixed effects determine the following parameters: Imax, IC50, and Hill coefficient, which describe the relationship between the plasma concentration and BP in population. The value of these parameters may vary between populations such as healthy volunteers and patients with schizophrenia. The random effects consist of interindividual variability and residual variability. The interindividual variability is the between-subject variability of parameters that explain the difference between individual BP and the population BP predicted from the model. The interindividual variability of the parameters is modeled using an exponential error model as follows:

where Pi represents the hypothetical true parameter value for the i-th individual, θ is the typical population value of the parameter, and η i is a random interindividual variability with zero mean and variance ɷ2.
The residual variability is within-subject variability or measurement error of BP, which results in the difference between individual BP from observation and prediction. The residual variability is modeled as a combined error model as follows:

where BPijpred and represent the i-th subject's j-th observed and predicted BP, respectively. The ηij is a normally distributed random variable with zero mean and variance σ2, and the superscripts P and A on the ∊ values represent the proportional and additive errors, respectively.
From the nonlinear mixed effect modeling, we obtained individual estimates of baseline BP as follows:

where baseline BPi represents the true baseline BP value for the i-th individual, Imax is typical population value of the maximum inhibitory effect, and η i is interindividual variability of the maximum inhibitory effect for the i-th individual.
The analysis was performed using NONMEM ver. VII, level 1.0 software (GloboMax, Ellicott City, MD, USA).
Calculation of Dopamine Receptor Occupancy
The dopamine D2 receptor occupancy by antipsychotic drugs was calculated as the percentage reduction of BP with drug treatment compared with the baseline:

We calculated dopamine receptor occupancy with true measured baseline BP, the age-corrected average baseline BP derived from the other data set (substitution method), and estimated individual baseline BP from the inhibitory Emax model (Imax method). The age-corrected average baseline BP for the substitution method was obtained as follows: age-corrected BP = mean BP—regression coefficient × (subject age—mean age).
Statistical Analysis
Independent t-tests were used to investigate differences in subject characteristics. The correlation between measured baseline BP and baseline BP estimated from the Imax method was explored using Pearson's correlation analysis.
We estimated the reliability between the true measured receptor occupancy and the predicted receptor occupancy using the intraclass correlation coefficient (ICC), as described by Shrout and Fleiss (1979). This model calculates the correlation between the true measured and the predicted occupancy values using a one-way analysis of variance with random subject effects. We selected this model over a one-way random effect model as the values were ordered into measured and predicted values.
We defined the variability of the receptor occupancy as follows:

where measured occupancy is the dopamine receptor occupancy calculated from measured baseline BP and predicted occupancy is the occupancy calculated from baseline BP estimated by the substitution or Imax method. The variability was tested by mixed effect models, with the method (modeled as a dummy variable: 1 = substitution and 2 = Imax) and the time after the administration of antipsychotic drugs as fixed effects.
Results
The mean baseline BP ± s.d. actually measured before the administration of YKP1358 or aripiprazole was 2.2 ± 0.3 in the YKP1358 group and 2.0 ± 0.2 in the aripiprazole group (Table 1).
Subject characteristics
Binding potential.
The relationship between plasma concentration and BP showed a good fit to the inhibitory Emax model (Figure 1). Imax was 2.1 (95% confidence interval (CI): 1.6 to 2.5) in the YKP1358 group and 1.8 (95% CI: 1.5 to 2.1) in the aripiprazole group. IC50 was 8.5 ng/mL (95% CI: 2.9 to 14.1) in the YKP1358 group and 14.2 ng/mL (95% CI: 8.8 to 19.6) in the aripiprazole group. Hill coefficient was 0.8 (95% CI: 0.6 to 0.9) in the YKP1358 group and 0.9 (95% CI: 0.7 to 1.1) in the aripiprazole group. The individual baseline BPs estimated by the inhibitory Emax model were correlated with the true measured baseline BPs (YKP1358: Pearson's correlation = 0.704 and P = 0.034; aripiprazole: Pearson correlation = 0.500 and P = 0.035).
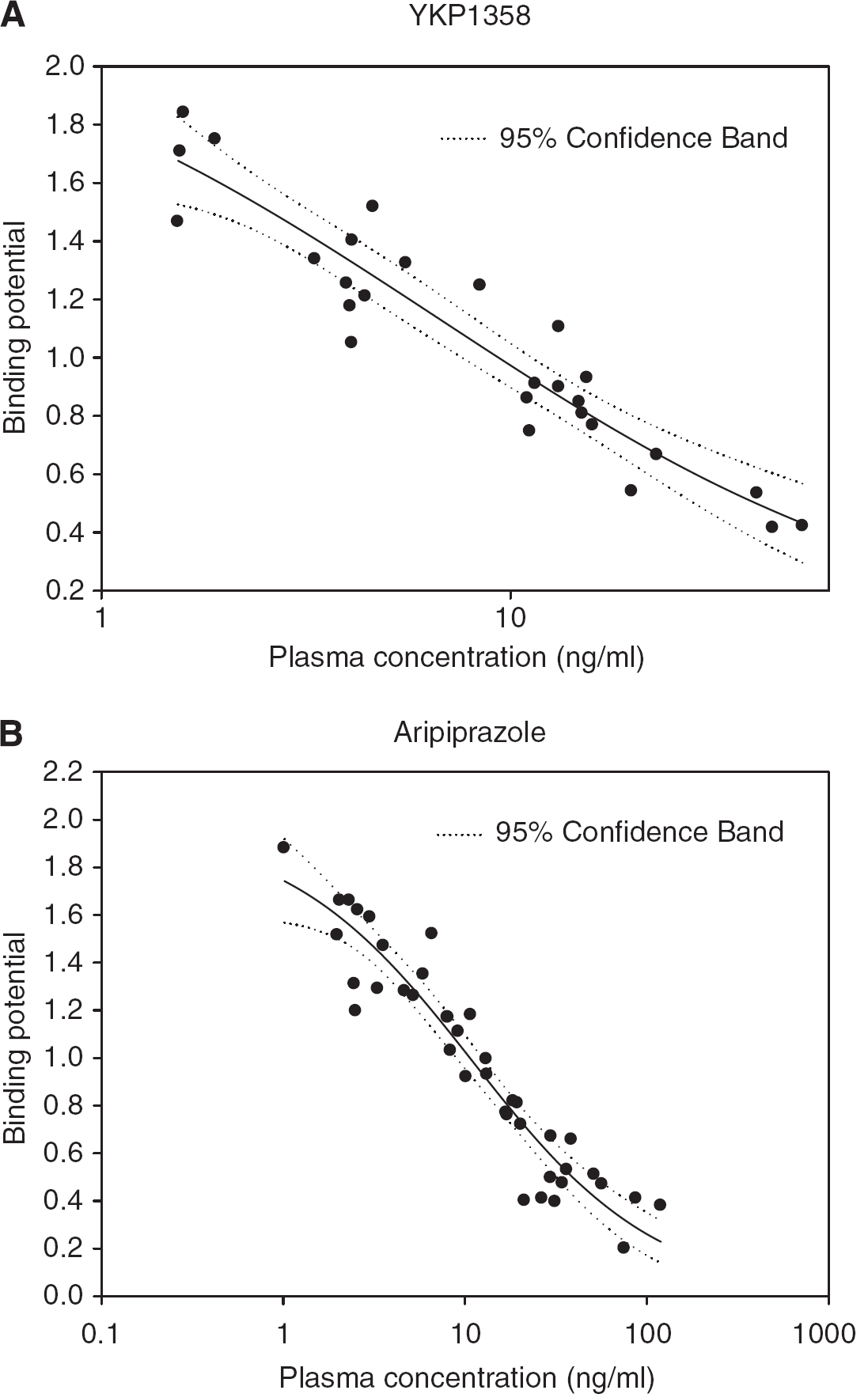
The relationship between plasma concentration and binding potential after the administration of YKP1358 (
Table 2 shows the ICCs between occupancies of YKP1358 calculated from measured and estimated baseline BP. All the ICCs of the Imax method are above 0.8, but those of the substitution method show lower values than 0.8.
Intraclass correlation coefficient (ICC) in YKP1358 study between dopamine D2 receptor occupancies calculated from measured and estimated baseline binding potential
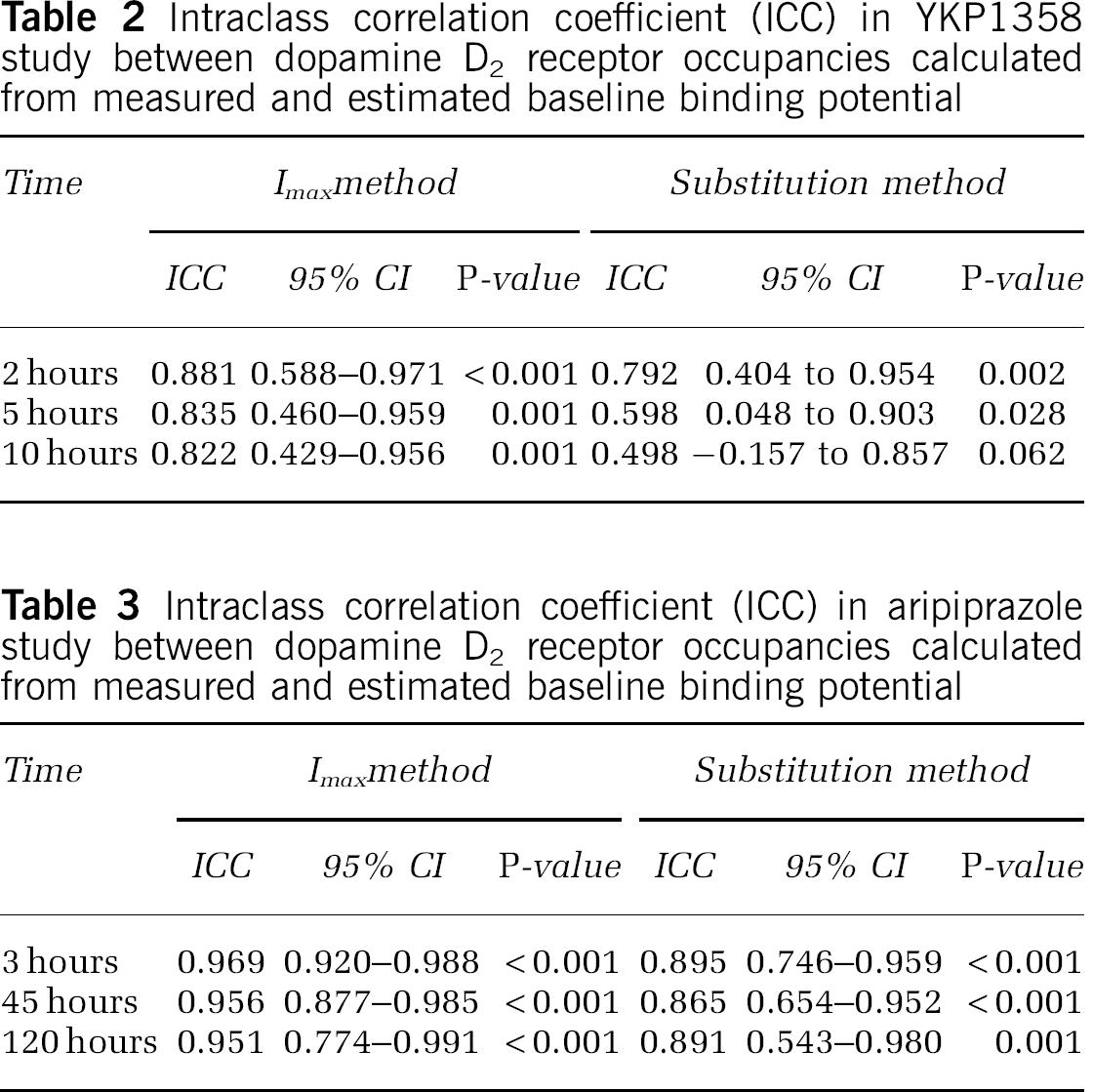
The ICCs between occupancies of aripiprazole calculated from measured and estimated baseline BP are presented in Table 3. The ICCs of the Imax method are higher than those of the substitution method, but all the ICCs show higher values than 0.8.
Intraclass correlation coefficient (ICC) in aripiprazole study between dopamine D2 receptor occupancies calculated from measured and estimated baseline binding potential
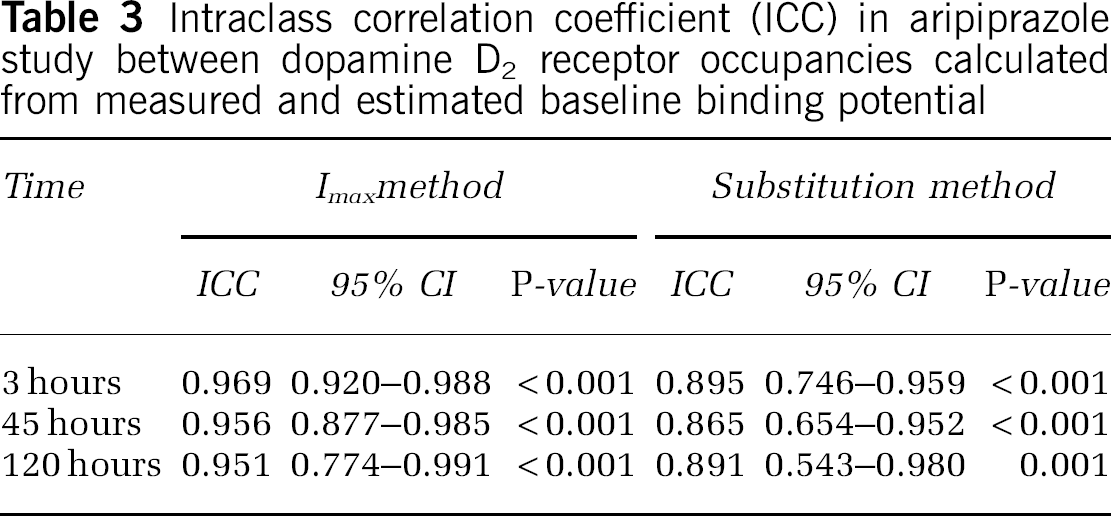
Figure 2 shows the correlation between the dopamine receptor occupancies of YKP1358 calculated from measured and estimated baseline BP. The correlation between the occupancies of aripiprazole is shown in Figure 3. The variability of dopamine receptor occupancy from the substitution method was significantly larger than that from the Imax method in the YKP1358 study (method: degrees of freedom (d.f.) = 1, 40, F = 8.635, and P = 0.005; time: d.f. = 2, 40, F = 12.355, and P = 0.001; and method × time: d.f. = 2, 40, F = 2.426, and P = 0.101; Figure 4A). In the aripiprazole group, the variability from the substitution method also exhibited larger value than that from the Imax method (method: d.f. = 1, 57, F = 6.544, and P = 0.013; time: d.f. = 2, 59, F = 8.229, and P = 0.001; and method × time: d.f. = 2, 57, F = 0.942, and P = 0.396; Figure 4B).
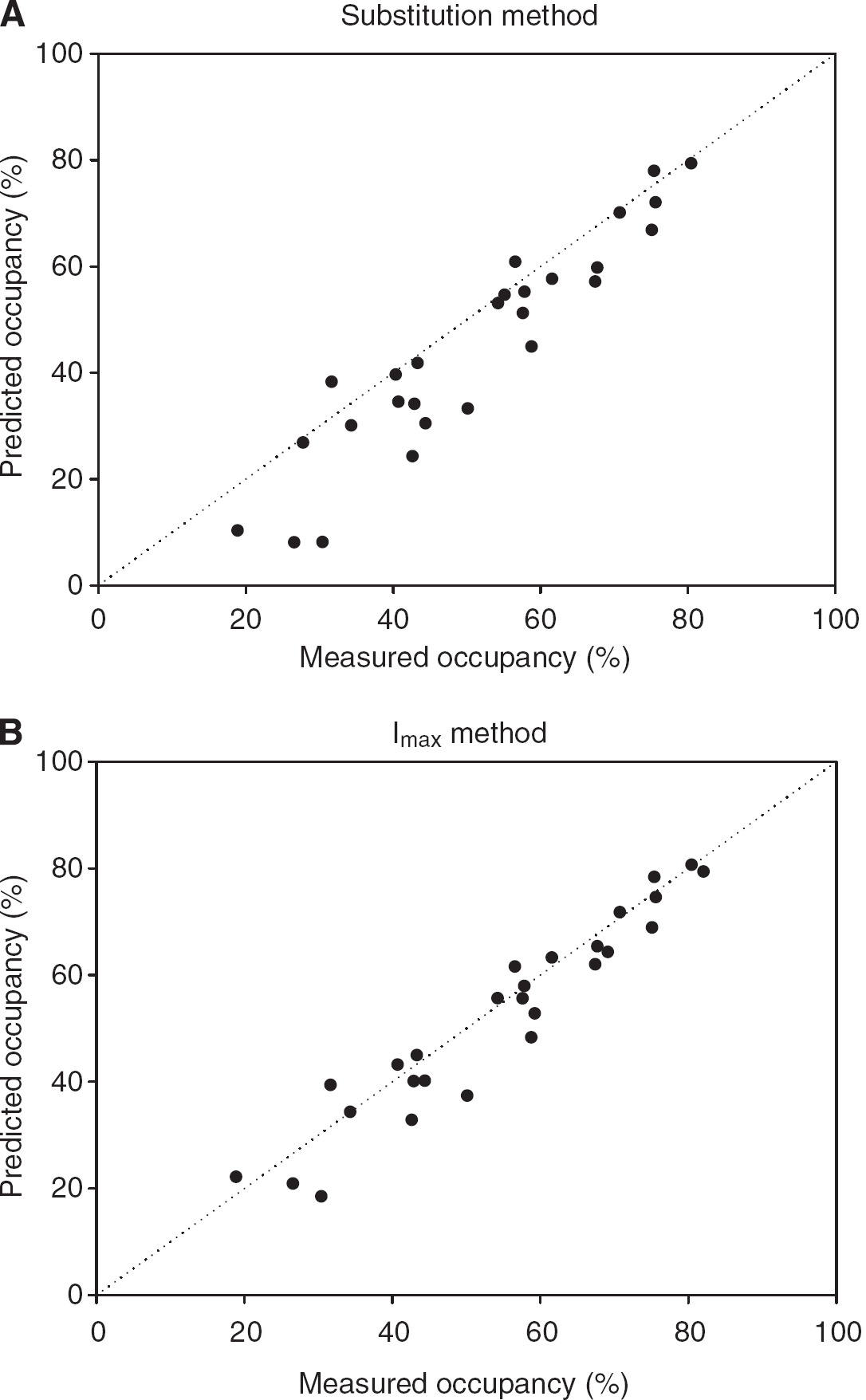
The correlation between dopamine D2 receptor occupancies of YKP1358 calculated from measured and predicted baseline binding potential. Measured occupancy means dopamine D2 receptor occupancy calculated from measured baseline binding potential. Predicted occupancy indicates dopamine D2 receptor occupancy calculated from baseline binding potential estimated by the substitution (
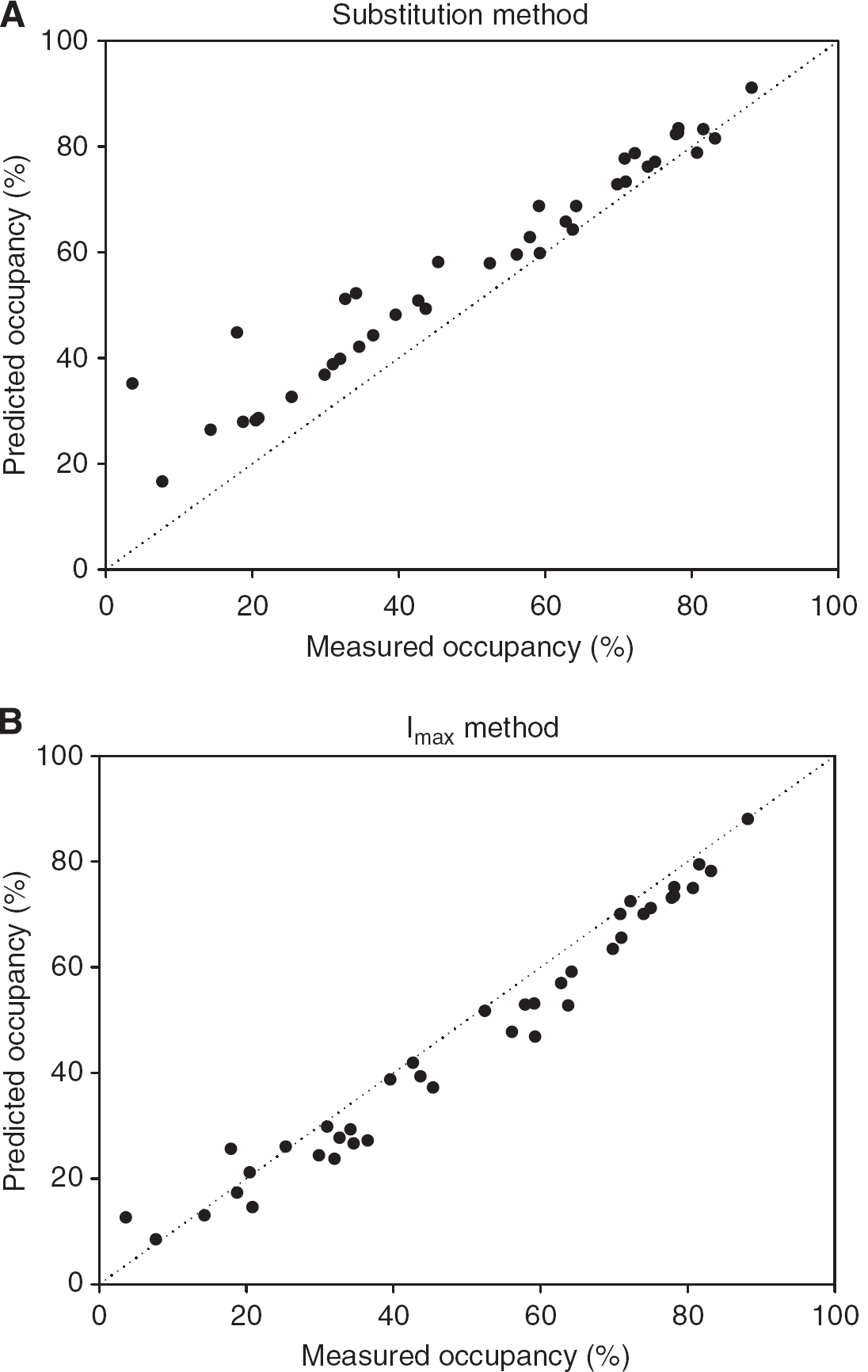
The correlation between dopamine D2 receptor occupancies of aripiprazole calculated from measured and predicted baseline binding potential. Measured occupancy means dopamine D2 receptor occupancy calculated from measured baseline binding potential. Predicted occupancy indicates dopamine D2 receptor occupancy calculated from baseline binding potential estimated by the substitution (

Variability of dopamine D2 receptor occupancy of YKP1358 (
Discussion
This study sought to determine whether the Imax method is an alternative to the substitution method for determining D2 receptor occupancy in clinical drug studies. Our main finding is that the Imax method shows excellent reliability and its estimate of baseline BP is highly correlated with the true baseline BP. Furthermore, in the first study with YKP1358, the Imax method showed greater reliability and lower variability than the substitution method, and the same pattern of results was found in the second study with aripiprazole.
The substitution method exhibited a trend toward underestimation or overestimation of the occupancy. As seen in the Figures 2 and 3, the underestimation or overestimation may happen in the lower occupancy range where the BP becomes close to baseline BP. The time effect on the variability reflects the trend. The underestimation can occur when a population-based baseline BP lower than the actual magnitude in the individual is used as in the YKP1358 study (Figure 2) and vice versa as in the aripiprazole study (Figure 3).
Such underestimation or overestimation may result from the individual or population difference in baseline BP from the average value of baseline BP used in the substitution method. Our sample showed a coefficient of variation of ~ 10% in baseline BP (Table 1), and the range of baseline BP was 1.7 to 2.7 in YKP1358 study group and 1.6 to 2.5 in aripiprazole study group. This means that the difference between true baseline BP and average baseline BP for the substitution method can be as high as 35% (average baseline BP for substitution method in YKP1358: 2.0 and highest baseline BP in YKP1358 study group: 2.7). Moreover, previous studies have reported larger coefficient of variation for baseline BP in patients with schizophrenia (healthy volunteers: 10% and patients: 20%; Kegeles et al, 2010) and upregulation of dopamine receptor after the exposure to antipsychotic drugs (Ginovart et al, 2009; Lee et al, 1978; Mackay et al, 1982; Silvestri et al, 2000). This suggests that the substitution method (with either the average baseline BP of healthy volunteers or drug-naïve patients) would lead to even greater inaccuracy in measuring the dopamine D2 receptor occupancy in patients with schizophrenia than found in our study in healthy volunteers.
In contrast, the Imax method accounts for interindividual and population variability in baseline BP in the determination of dopamine D2 receptor occupancy in a way that the substitution method does not, because the Imax method estimates the population value and interindividual variability of baseline BP based on data from the subjects being investigated rather than an unrelated sample. Consequently, receptor occupancy determined using the Imax method should be a better estimate of ‘true’ receptor occupancy than that based on baseline BP derived from an unrelated sample. The results show that ICCs for the Imax method are consistently higher than 0.8, which indicates ‘almost perfect’ reliability between occupancies calculated from measured baseline BP and estimated baseline BP from the Imax method (Landis and Koch, 1977). Some ICCs for the substitution method also show higher values than 0.8, but the ICCs are not consistent across the studies and time after drug administration. This means the reliability of the substitution method can be influenced by the distribution of actual baseline BP values and the substituted baseline BP value. Our findings, taken with evidence of the heterogeneity in D2 receptor BP in schizophrenia (Kegeles et al, 2010; Kestler et al, 2001; Laruelle, 1998), indicate that the Imax method is preferable to the substitution method for calculating dopamine D2 receptor occupancy in clinical studies where it is not possible to obtain a baseline BP.
We validated the Imax method with data from two different studies that conducted serial PET scans to give multiple data points in the same individual. The multiple data points might help build stable inhibitory Emax model and estimate reliable receptor occupancy. From this point of view, the Imax model may be less accurate when it is based on data made up of single observations in each individual. This could be a limitation of the Imax method. In the case with single observations, the substitution method could work better than the Imax method under the condition that the baseline BP for the substitution should be derived from the same kind of group as the target group (healthy volunteers, drug-free patients, or drug-naïve patients).
Conclusion
The Imax method shows good reliability and less variability than the substitution method. The Imax method can be applied for dopamine receptor occupancy study, and bring more reliability and accuracy to the study about receptor occupancy in patients with schizophrenia.
Footnotes
The authors declare no conflict of interest.